Isolated external jugular thrombophlebitis secondary to acute pharyngitis: a case report and a review of the literature
Uche C. Ezeh, Naomi Tesema, Sukaina Hasnie, Philip J. Kahn, Max M. April

TL;DR
A 13-year-old with severe throat infection developed rare external jugular vein blood clot on the opposite side of facial swelling.
Contribution
First reported case of external jugular thrombophlebitis with sinusitis on the contralateral side in a pediatric patient.
Findings
EJT occurred in a 13-year-old with acute pharyngitis and left-sided sinusitis.
Anticoagulation and antibiotics led to resolution of thrombosis and sinus disease.
No prior reports of contralateral EJT and sinusitis in pediatric populations exist.
Abstract
External Jugular Thrombophlebitis (EJT) is a rare clinical phenomenon with few reports in the literature, especially in the pediatric population. This is a report of an unusual case of right-sided EJT in a pediatric patient secondary to acute pharyngitis with sinusitis most prominent on the left side. A 13-year-old presented to the emergency department with worsening upper respiratory infectious (URI) symptoms and facial swelling, cough, throat pain, and emesis. The patient had traveled to Switzerland and received amoxicillin for strep throat 6 weeks before this hospitalization. Physical examination revealed nasal purulence, allodynia over the right side of the face without overlying erythema, and oropharyngeal exudate. CT scan revealed left-sided predominate sinusitis and right external jugular vein thrombosis. Blood cultures confirmed the presence of group A streptococcus infection.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
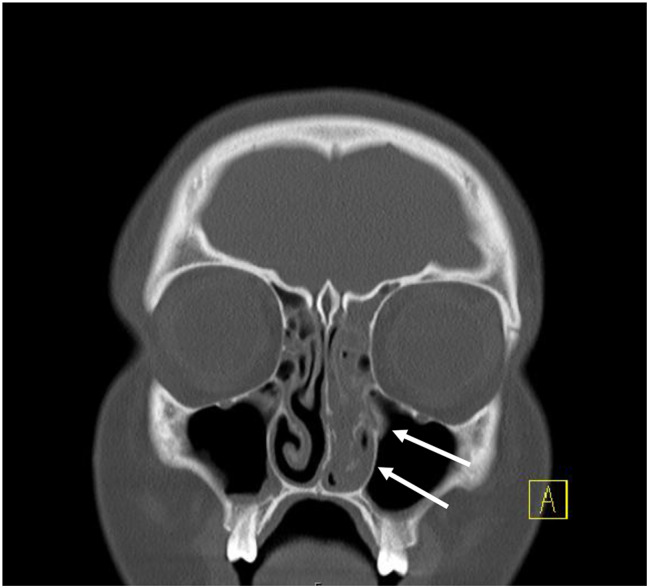 Figure 1
Figure 1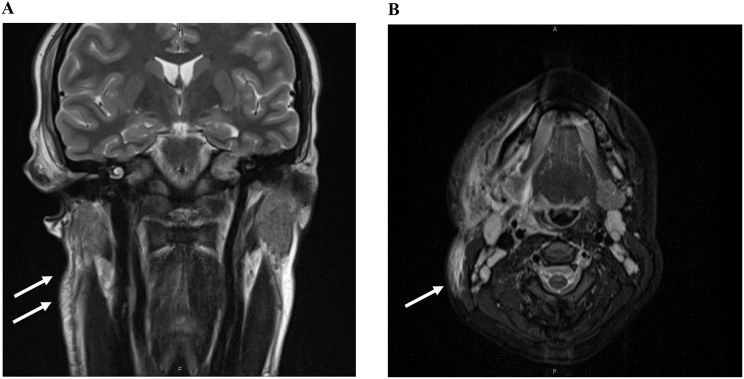 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Otolaryngology and Infectious Diseases · Streptococcal Infections and Treatments
Background
Jugular venous thrombosis is a severe condition primarily affecting the internal jugular vein (IJV), which originates at the jugular foramen and forms part of the carotid sheath. The most common causes of IJV thrombosis are cancer and central venous catheter use, with trauma, infection, and IV drug abuse also identified as contributing factors [1].
In contrast, external jugular vein (EJV) thrombosis is a rare clinical phenomenon, and there is a scarcity of published studies on this topic [2]. The leading causes of EJV thrombosis in adults include trauma, malignancy, catheterization, head and neck infections, intravenous drug use, and compression at the affected site. Additionally, factors such as age, gender, and obesity may potentially play a role [2]. Due to the infrequency of this condition, there is a lack of consensus regarding the optimal management strategies, and no controlled studies have been conducted in pediatric populations. In this report, we present the case of a pediatric patient who presented with isolated EJV thrombophlebitis (inflammation of a vein related to blood clot formation) secondary to acute pharyngitis with intracranial complications. We also provide a comprehensive review of the existing literature on cases of isolated EJV thrombophlebitis.
Case presentation
A 13-year female patient with mild oligoarticular juvenile idiopathic arthritis (JIA), with no history of immunosuppressive medication, presented to the emergency department (ED) with right facial swelling, cough, throat pain, bilateral frontal headache, and non-bloody emesis. She had traveled to Switzerland for 6 weeks before the hospitalization and tested positive for strep throat, for which she received 10 days of Augmentin treatment. Although her sore throat initially appeared to improve, it subsequently recurred along with pain and swelling over the right side of the face three days before she visited the ED. At an outpatient clinic, she exhibited a high fever (104 °F), and the physical examination revealed pain with neck motion in all directions, trismus, and erythema of the posterior oropharynx without exudates or petechiae. A strep test confirmed infection with beta-hemolytic streptococci Group A (Strep. Pyogenes). Laboratory tests in the ED showed an elevated white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels (Table 1). Computer tomography (CT) imaging confirmed acute sinusitis most severe on the left side, raising suspicion of a bacterial infection (Fig. 1).
Table 1. Laboratory results on day of ED admissionLaboratory Results (Admission Day)ResultsNormal RangeWhite Blood Cell (WBC) count 21.8 4.2–9.4 103/uLRed Blood Cell (RBC) count4.563.90–4.90 106/uLHemoglobin (Hb)1310.8–13.3 g/dLPlatelet Count251150–400 10*3/uLNeutrophil (%) 87 39–74%ESR 90 0–20 mm/hrCRP 269.1 0–5 mg/LD-dimer1,665< 230 ng/mL DDUGram StainGram (+) Cocci (Pairs)Blood cultureBeta-Hemolytic Streptococci Group A (Strep. pyogenes)
Fig. 1CT scan without contrast illustrating coronal image with sinusitis more severe on the left side (white arrows)
Physical examination revealed purulence in both nasal cavities, edema of the right temporalis muscle, allodynia over the right side of the face, and oropharyngeal exudate. She did not endorse vision changes, rash, dental pain, or pain with eye movements. On the second day of hospitalization, MRI findings indicated the possibility of intracranial dural/leptomeningeal inflammation, left sinusitis, right myositis, and right parotitis (Fig. 2). Treatment included the administration of ampicillin/sulbactam, analgesics, dexamethasone, and non-steroidal anti-inflammatory drugs (NSAIDs). Additionally, blood and sinus cultures were collected for further analysis.
Fig. 2MRI sinuses without contrast showing white arrows pointing right sided myositis and parotitis in coronal (A) and right sided EJV thrombophlebitis in axial images (B)
Blood cultures confirmed the presence of a group A Streptococcus (GAS) infection caused by Streptococcus pyogenes, which raised suspicion of Lemierre’s syndrome. Consequently, the antibiotic treatment regimen was adjusted to include ceftriaxone and clindamycin for anaerobic coverage. She remained afebrile after hospital day 2. A Doppler ultrasound revealed a non-occlusive thrombus in the right external jugular vein (EJV), while the internal jugular vein (IJV) and carotid arteries exhibited normal blood flow (Table 2). In response to the EJV thrombophlebitis, the treatment plan was further adjusted, and anticoagulation therapy with enoxaparin sodium was initiated.
During hospitalization, the patient experienced a desaturation event of 82% on room air, tachycardia, and tachypnea, prompting the use of a high-flow nasal cannula (20 L, 40%). Given the suspicion of pulmonary embolism, chest imaging was conducted on the third day of admission. Pleural effusions and atelectasis were observed on the chest X-ray, but a CT pulmonary angiogram did not reveal any evidence of a pulmonary embolism. The patient was transferred to the PICU due to a need for increased respiratory support and after stabilization, received high-dose intravenous 10 mg dexamethasone as her clinical decline was thought to be related to the worsening of the spreading inflammatory process across her face. After two days, she was transferred back to the floor with decreased facial swelling, resolution of pain, and resolution of respiratory symptoms.
Follow-up ultrasound imaging on the sixth day demonstrated an improvement in thrombophlebitis, cellulitis, and sinus disease. Of note, the patient had no mention of central line placement in the neck in her medical history and did not receive a central line during this admission. Once stable, the patient was discharged on enoxaparin therapy for 6 weeks before starting rivaroxaban daily for 4 weeks as it poses a reduced risk of bleeding in children [3]. The patient continued 4 weeks of IV antibiotics followed by 2 weeks of oral Augmentin. At 6-month follow-up, an ultrasound examination revealed no signs of acute deep or superficial vein thrombosis in the right EJV and other upper extremity vessels (Table 2). Anticoagulation treatment was discontinued 10 weeks after discharge. The patient’s juvenile idiopathic arthritis is in clinical remission, taking NSAIDS as needed. Follow-up is now on a yearly or as needed basis, and the patient no longer takes anticoagulation. Her long-term prognosis is excellent and there are no reported complications or recurrences in the medical record.
Table 2. Diagnostic studies and results during hospital course and at follow upDay of HospitalizationDiagnostic ImagingFindings1CT Head and NeckSinusitis predominately in left frontal and paranasal sinuses2Bilateral US Duplex carotid arteriesNo evidence of stenosis in both carotid arteries2Bilateral US Upper Extremities VenousNo evidence of thrombosis in bilateral internal jugular veins2MRI Brain and Neck with and w/o contrastDural and leptomeningeal enhancement likely a severe complication of sinusitis; severe sinonasal changes on the left side and right sided intracranial involvement; widespread transspatial inflammatory changes in right face, multifocal myositis and parotitis of the right side3MRI Sinuses w/o IV contrastInflammation of right periauricular soft tissue and cellulitis at right lower face; Spread of inflammation on right side of face, increased from previous MRI neck. Persistent linear T2 hypointense signal along the right external jugular vein concerning for thrombophlebitis.3CT Angio chest with IV contrastNo evidence of pulmonary embolism4Right US Duplex Upper Extremities VenousNo evidence of right internal jugular vein thrombosis; Right external Jugular Vein is dilated and non-compressible (above clavicleto mid neck)8MRI sinuses w/o IV contrastResolution of myositis; resolution of neck cellulitis; Decreased sinusitis; trace bilateral pleural effusions10Right US Duplex Upper Extremities VenousEvidence of DVT in right external jugular vein1 month followupRight US Duplex Upper Extremities VenousEvidence of DVT in right external jugular vein, no change from previous6 month followupRight US Duplex Upper Extremities VenousNo evidence of acute deep or superficial vein thrombosis in the upper extremity. Patent and compressible veins.
Review of the literature
A PubMed search was conducted using the terms “external jugular vein” OR “external jugular thrombophlebitis,” resulting in a total of 368 articles. Non-English articles were excluded from the search, as were articles that did not specifically focus on patients with isolated external jugular vein involvement. A comprehensive literature review identified 33 other studies (n = 37 cases) discussing isolated EJV thrombosis or thrombophlebitis (Table 3). Among these cases, most were associated with infectious causes. Notably, a study conducted by Schwartz et al. focusing on infections involving the EJV identified 21 relevant studies (n = 16 cases) [4]. In contrast, our literature review diverges from their specific focus and encompasses patients with isolated EJV thrombophlebitis attributed to various etiologies. After reviewing the abstracts and references, a total of 33 articles comprising solely case reports or case series were identified (Table 3).
Table 3. Clinical details of 33 studies, including the present case, with isolated EJV thrombosis in the literatureAuthorReferencePatientAgeSexJugular ThrombosisEtiologyOrganismChief ComplaintComplicationsTreatmentLength of TreatmentResolutionBahuth et al.[3]169FEJV only (extension into subclavian vein to the angle of the mandible)--swollen and tender neck-surgical excision-n/aColmina et al.[1]240FEJV onlystasisn/aright cervical pain, odynophagia-heparin10 daysfully resolvedCupit-Link et al.[4]318MEJV only---pulmonary septic emboli, pneumoniaanticoagulation (LMWH)n/afully resolved432MEJV only---pulmonary septic emboli, neck abcessanticoagulation (LMWH and warfarin)n/afully resolved542MEJV only---conservative treatment-fully resolvedEzeh et al. (current study)613FEJV onlystrep throatGroup A Streptococcusfacial swelling, cough, throat painsinusitis, facial cellulitisanticoagulants (LMWH, enoxaparin) and antibiotics (ceftriaxone, flagyl, vancomycin)6 monthsfully resolvedFishman et al.[5]737FEJV onlycatheterization-pain-conservative treatment-fully resolvedGale et al.[6]887FEJV onlyfracture and immobilizationn/apain, arm pitting edema-anticoagulants (warfarin, enoxaparin)3 monthsfully resolvedGonzalez et al.[7]956MEJV onlyTMJ arthroscopy-neck pain-anticoagulants (rivaroxaban)6 monthsfully resolvedHagiya et al.[8]1074FEJV onlyLemierre syndrome (laryngopharyngitis)Fusobacterium nucleatumpharyngeal pain, cold symptomsDICantibiotics (ampicillin/sulbactam, ceftriaxone/clindamycin) and anticoagulants (heparin, enoxaparin)antibiotics (4 weeks), anticoagulants (unknown)fully resolvedHindi et al.[9]1121MEJV only (bilaterally)-painless neck swellings, facial swelling-anticoagulation (heparin, warfarin)-fully resolvedHulinsky et al.[10]1227FEJV only (extension into subclavian vein to the angle of the mandible)ovarian hyperstimulation syndrome-supraclavicular pain-anticoagulants (LMWH)-n/aHutson et al.[11]1312MEJV onlyLemierre syndrome (secondary to tonsillitis)-unilateral face and neck swelling, sore throat and dysphagia-antibiotics (penicillin, metronidazole) and dexamethasone7 weeksfully resolvedIoanno et al.[12]1440FEJV onlyaneurysm-tender mass in cervical region-surgical excisionn/afully resolvedJudd et al.[13]1514FEJV onlyLemierre syndrome (secondary to tonsillitis)n/aneck pain, lethargy, sore throat, trismuspulmonary septic emboliAntibiotics (clindamycin, co-amoxyclav) and anticoagulation (LMWH, warfarin), surgical excisionantibiotics (14 days); anticoagulation (6 weeks)fully resolvedKim et al.[14]1646FEJV onlyaneurysm-n/a-anticoagulants (LMWH)-fully resolvedLu et al.[15]1719FEJV onlyLemierre syndromeFusobacterium necrophorumtender lymphadenopathy, pleuritic chest pain, dyspneapulmonary septic emboliantibiotics (piperacillin-tazobactam, metronidazole)6 weeksfully resolvedMorris et al.[16]1818FEJV onlyLemierre syndrome (secondary to tonsillitis)n/asore throat, neck pain, malaise, maculopapular rashpulmonary septic emboliantibiotics (clindamycin, ciprofloxacin) and anticoagulants (LMWH)antibiotics (4 weeks)fully resolvedPucci et al.[17]1959FEJV onlyneck mass-neck sorness-surgical excision--2069FEJV onlyneck mass--surgical excision--2124MEJV onlyneck mass--surgical excision--Quinn et al.[18]2245FEJV only--pain neck-surgical excision--Raju et al.[19]2385MEJV onlyneck trauman/aneck swellingconservative treatmentn/afully resolvedRamirez et al.[20]2416MEJV onlyLemierre syndromen/apharyngitis, weight loss, fever, should, elbow, knee pain, fatigue-Antibiotics (clindamycin) and anticoagulation (IV heparin, enoxaparin)8 weeksn/aReicher et al.[21]2565FEJV onlyLemierre syndrome (secondary to tonsillitis)n/asore throat, neck pain, fever, trismuspulmonary septic emboliantibiotics (co-amoxiclav) and anticoagulants (heparin, and oral anticoagulant)antibiotics (4 weeks) and anticoagulation (4 weeks)fully resolvedSafadi et al.[22]2693FEJV onlythyroid massn/apain, redness, neck swelling-anticoagulants (unspecified)n/afully resolvedSanivarapu et al.[23]2731MEJV only (extension into subclavian vein, brachiocephalic vein, superior mediastinum)Lemierre syndrome (secondary to COVID-19)-neck pain, swellingpulmonary septic emboli, parotitisantibiotics (linezolid, piperacillin and tazobactam, clindamycin, ertapenem) and anticoagulation (apixaban)antibiotics (4 weeks) and anticoagulation (4 weeks)partially resolved (developed parotitis)Schwartz et al.[24]2849MEJV onlygingiva traumaKlebsiella pneumoniaefever, chills, face and neck swelling-antibiotics (cefotaxime, metronidazole, ciprofloxacin), anticoagulation (unspecified) and surgical excisionantibiotics (2 weeks)fully resolvedSchwarz et al.[25]2917FEJV onlyLemierre syndrome (secondary to tonsillitis)n/achest pain, fever, mandibular tenderness, trismus, lymphadenitis, dyspnea-antibiotics (amoxicillin-clavulanic acid, ceftriaxone, metronidazole) and anticoagulation (enoxaparin)n/afully resolvedSengupta et al.[26]3045Mbilateral EJVidiopathic-face puffiness, neck swelling-anticoagulation (aspirin)n/afully resolvedSuzuki et al.[27]3185FEJV onlyLemierre syndromeStreptococcus intermediusn/a-antibiotics (clindamycin, tazobactam, piperacillin) anticoagulation (heparin, edoxaban solilate hydrate)antibiotics (37 days) and anticoagulation (37 days)fully resolvedSuzuki et al.[28]3241FEJV onlyLemierre syndromealpha-hemolytic Streptococcusmandibular pain, toothache, trismus, fever, chills-antibiotics (ampicillin sulbactam)antibiotics (4 weeks)fully resolvedTakiguchi et al.[29]3351FEJV onlyLemierre syndromegroup C Streptococcussore throat, jaw painshock, multiple organ failure, pulmonary septic emboliantibioticsn/afully resolvedVerma et al.[30]3445FEJV onlyaneurysm-progressive swelling in supraclavicular region, pain-surgical excision-n/aVillanueva et al.[31]3569FEJV onlyidiopathic-painful lump in cervical region-anticoagulation (unspecified)n/afully resolvedWarabi et al.[32]3659MEJV only (with peritonsillar vein involvement)Lemierre syndromen/aheadaches, fever, chills, temporal brainpulmonary septic emboli, brain abscessantibiotics (cefazolin, clindamycin) and anticoagulation (heparin)n/apartially resolved (developed facial nerve palsy, hearing disturbance)Williams et al.[33]3719MEJV onlyLemierre syndromeFusobacterium nucleatumfever, sore throat, chest pain, rigors, nausea, vomitingpulmonary septic emboliantibiotics (levofloxacin, metronidazole) and anticoagulation (heparin)n/an/aYoung et al.[34]3815FEJV onlyLemierre syndromeFusobacterium necrophorumfever, joint pain, dyspnea, throat pain, lymphadenopathyAntibiotics (clindamycin) and anticoagulation (IV heparin, enoxaparin)antibiotics (28 days), unknown anticoagulationfully resolved
Discussion and conclusions
This report presents a rare case of isolated EJV thrombophlebitis as a complication of acute pharyngitis. The diagnosis and management of our patient posed particular challenges due to concurrent sinusitis, which appeared more severe on the left side of the face based on CT imaging, while the EJV thrombophlebitis, myositis, and parotitis affected the right side of the face. Furthermore, initial concern for meningitis arose based on CT and MRI findings.
The external jugular veins are positioned laterally and superficially to the internal jugular veins. This anatomical arrangement, coupled with the common clinical utilization of the IJV as a route for accessing central circulation, likely contributes to a higher number of reported cases of IJV thrombosis compared to EJV thrombosis. Isolated thrombosis of the EJV is infrequently discussed in the literature, especially in the pediatric population [2, 5–7]. It is associated with head and neck infections [8–22], trauma [23], catheterization [24], tumor compression [25, 26], aneurysms [27, 28], or other unknown factors [5, 29, 30]. Less common factors, including obesity, orthopedic fractures, procedural complications, deep tissue massage, COVID-19 infection, and ovarian hyperstimulation syndrome, have also been implicated in EJV cases in adults [2, 23, 31–34]. Symptoms of EJV thrombosis include fever, neck pain and swelling, and sore throat [35].
The mechanism by which a head and neck infection selectively invades the EJV is not fully understood, considering its anatomical distance from the pharyngeal space compared to the IJV. Some studies have suggested that anatomical variations in the jugular venous system might contribute to this observation [4, 36, 37]. During our investigation into the underlying cause of thrombosis in our patient, the care team deliberated on the potential presence of Lemierre’s syndrome. However, the absence of typical symptoms and sequelae, such as pulmonary septic emboli, the identification of GAS as the cultured organism, and the isolated involvement of the EJV, made the diagnosis less likely at that time. Nevertheless, it is worth noting that the literature has documented instances of Lemierre’s syndrome solely affecting the EJV and involving other organisms besides Fusobacterium species (i.e. Streptococcus, Klebsiella) [19, 37]. Regardless, it is important to emphasize that this hypothetical diagnosis would not have affected the treatment course administered. Our leading hypothesis regarding the mechanism of EJV thrombophlebitis in our patient is that the barotrauma she experienced while traveling may have facilitated the spread of pharyngitis into the EJV. Existing literature supports the notion that patients with autoimmune conditions, notably juvenile rheumatic arthritis, are at a higher risk of VTE [38]. Furthermore, airplane travel has been associated with an increased risk of VTE, with a dose relationship starting at 4 h [39]. Consequently, the combination of these conditions in our patient could potentially elevate the risk of a thrombotic event. However, whether these factors also impact a more superficial vein such as the EJV remains an area of ongoing investigation.
Anticoagulation is considered the mainstay of treatment for internal jugular vein (IJV) thrombosis, while cases of IJV thrombosis resulting from infectious causes, such as Lemierre’s syndrome, require antibiotic therapy. The use of anticoagulation therapy in Lemierre’s syndrome remains a topic of debate and is typically recommended in specific situations. These include when the thrombus extends into the cerebral sinuses, in the presence of a large or bilateral clot burden, or when there is a lack of improvement despite appropriate antibiotic or surgical therapy [40]. A case report and review of the literature published in 2021 found that there is no consensus regarding the use of anticoagulation external jugular venous thrombosis [4]. However, a review found that 90% of pediatric patients who were given anticoagulation with low molecular weight heparin had thrombus improvement for resolution within a median of 3.4 months, and there were no adverse effects from anticoagulation therapy [41]. Our case was like other reported cases in the use of multimodal treatment to treat this condition involving antibiotics, anticoagulation, and fellowship trained physicians. Our case was unique in using oral anticoagulation agents, aligning with more up to date literature showing efficacy in Phase 2 trials.
In contrast, the treatment of EJV thrombosis or thrombophlebitis lacks consensus, offering a range of options that include antibiotics, anticoagulants either alone or in combination, surgical excision, or conservative management [42]. Several cases of EJV thrombosis cited in this study did use anticoagulation [4, 6, 9, 11, 13–16, 18, 20–23, 25, 27, 29–31, 33, 34, 42]. However, the use of anticoagulants remains controversial due to potential risks such as hemorrhage, thrombocytopenia, and skin necrosis. These risks must be carefully weighed against the potential of a fatal thromboembolic event.
Pulmonary embolism has been reported as a complication in approximately 10.3% of cases of internal jugular vein thrombosis [43]. Alternatively, a few documented cases of EJV thrombosis with clot propagation to the upper extremities and pulmonary vasculature exist [23, 44]. The reported number of PE complications in EJV thrombosis remains unknown, likely due to its rare occurrence. The EJV possesses a valve at its terminal end before entering the subclavian vein, preventing the regurgitation of blood from the subclavian vein to the EJV, which operates at relatively lower pressure [45]. In contrast, the internal jugular vein terminates in the brachiocephalic vein and subsequently empties directly into the superior vena cava (SVC). These anatomical considerations might explain the comparatively lower risk of pulmonary embolism in external jugular vein thrombosis when compared to internal jugular vein thrombosis. Given these distinctions, anticoagulation for EJT may not be necessary. Nevertheless, we encourage further research into this matter to gain a more comprehensive understanding of the appropriate management of EJV thrombosis.
Our study provides valuable insights into the unusual progression of an oropharyngeal infection that was appropriately treated to the severe complication of jugular embolism. EJV thrombophlebitis is a rare occurrence but our findings, supported by a comprehensive literature review, underscore the importance of heightened vigilance and clinical awareness among healthcare professionals when evaluating patients with oropharyngeal infections refractory to antibiotic treatment, and additional symptoms such as neck pain, headache, swelling, erythema, and a palpable neck mass. Prompt and accurate diagnosis is essential for effective management and the prevention of further complications. The use of anticoagulation is controversial, and the risk of embolism is far less clear with external jugular vein thrombosis [32]. Optimal treatment for EJV thrombosis has not been assessed, yet anticoagulation is likely not necessary unless the patient exhibits a severe infection or there is evidence of thrombus propagation. Further research is warranted to better understand the mechanisms underlying the selective invasion of the EJV by head and neck infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee Y, Siddiqui WJ. Internal Jugular Vein Thrombosis. In: Stat Pearls. Stat Pearls Publishing; 2023. Accessed July 11, 2023. http://www.ncbi.nlm.nih.gov/books/NBK 541111/31082155 · pubmed ↗
- 2González LV, López JP, Torres I, Martin-Granizo R. External jugular thrombosis: a previously unreported complication of Temporomandibular Joint Arthroscopy. Journal of oral and maxillofacial surgery. Published Online April. 2023;S 0278239123003464. 10.1016/j.joms.2023.04.001.10.1016/j.joms.2023.04.00137127149 · doi ↗ · pubmed ↗
- 3Allen BW, Anjum F, Bentley TP. Lemierre Syndrome. In: Stat Pearls. Stat Pearls Publishing; 2023. Accessed July 12, 2023. http://www.ncbi.nlm.nih.gov/books/NBK 499846/29763021 · pubmed ↗
- 4Bechmann S, Rahman S, Kashyap V, Anatomy. Head and Neck, External Jugular Veins. In: Stat Pearls. Stat Pearls Publishing; 2023. Accessed July 31, 2023. http://www.ncbi.nlm.nih.gov/books/NBK 538222/30855810 · pubmed ↗