Genotypes analysis and antifungal susceptibility of Candida albicans strains isolated from women with vaginal candidiasis in Jordan using PCR targeting 25SrDNA and ALT repeat sequences of the RPS
Rania M. Al-Groom, Rand Raid Mahmoud Ali, Qasem M. Abu Shaqra

TL;DR
This study analyzed the genetic diversity and antifungal drug susceptibility of Candida albicans strains causing vaginal infections in Jordanian women.
Contribution
The study identifies distinct genotypes of C. albicans and links them to varying antifungal susceptibility in a Jordanian population.
Findings
C. albicans was the most common cause of vaginal candidiasis among the studied population.
Three genotypes (A, B, C) were identified at the 25S rDNA gene, while nine subtypes were found using RPS markers.
Genotype A showed higher susceptibility to fluconazole, flucytosine, and ketoconazole compared to genotypes B and C.
Abstract
Genotypic identification of the etiologic agents of vaginal candidiasis (VC) is of significance in epidemiologic studies and in the establishment of adequate treatment protocol. The aim of this study was to determine the antifungal susceptibility and gene diversity of C. albicans isolated from a group of Jordanian women with VC. A total of 312 isolates of candida species, recovered from women with vaginal candidiasis who attended gynecology clinics affiliated to three major private hospitals in Amman over a period of five months (July 2020 to December 2020) were included in this study. The isolated Candida were characterized by phenotypic and genotypic means. Genotypic studies were performed using specific PCR primers of the rDNA and RPS genes. Susceptibility testing of all C. albicans isolates was conducted following the National Committee for Clinical Laboratory Standards and E-test…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
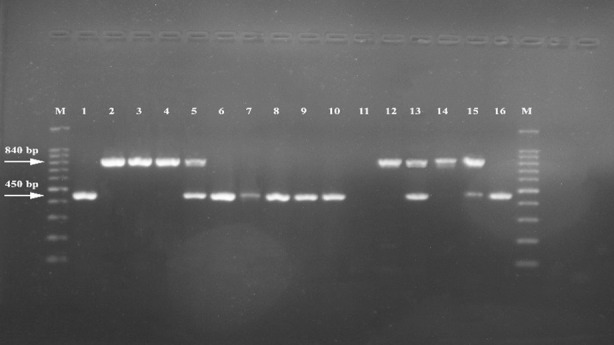 Fig.1
Fig.1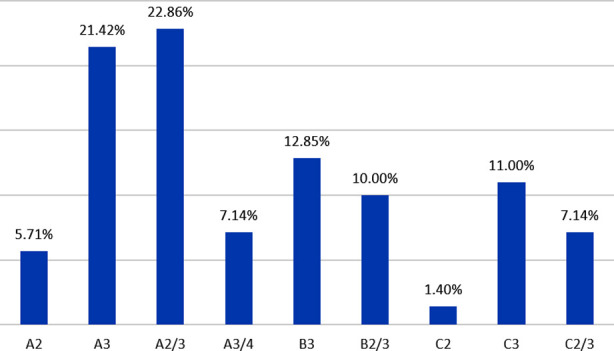 Histogram-1
Histogram-1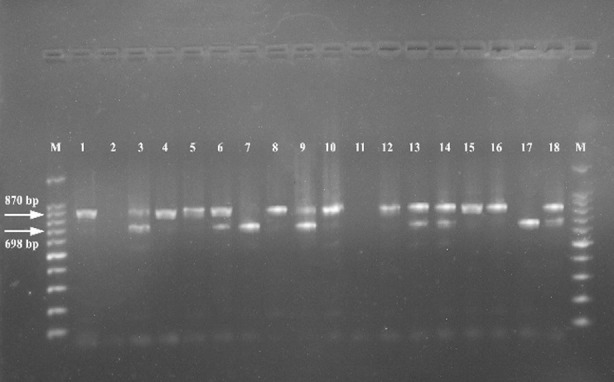 Fig.2
Fig.2| Primer (P-1) 25S rDNA | Nucleotides sequence |
| CA-INT-L CA-INT-R | Forward: ATAAGGGAAGTCGGCAAAATAGATCCGTAA |
| Primer (P-11) ALT repeat | Nucleotides sequence |
| ASDcF Pcscr | Forward: TGATGAACCACATGTGCTACAAAG |
| Age group / years | Number of cases | Percent of cases |
|---|---|---|
| 18-24 | 75 | 24 |
| 25-31 | 97 | 31 |
| 32- 38 | 50 | 16 |
| 39- 45 | 45 | 14.5 |
| > 46 | 45 | 14.5 |
| Candida Species | Number of Isolates | Percentage (%) | Color on Chromo agar |
|---|---|---|---|
|
| 175 | 56 | Light green |
|
| 105 | 33.6 | Rose pink |
|
| 30 | 9.60 | Pinkish purple |
|
| 2 | 0.80 | Metallic blue |
| Primer P-I | Band size (bp) | 25S rDNA type |
|---|---|---|
| CA-INT-L and CA-INT-R | 450 | A |
| 840 | B | |
| 450, and 840 | C | |
| 1040 | D | |
| 1080 | E |
| Primer P-II | Band size (bp) | ALT repeat |
|---|---|---|
| ASDcF Pcscr | 526 | 1 |
| 698 | 2 | |
| 870 | 3 | |
| 1042 | 4 | |
| 1214 | 5 | |
| 1386 | 6 |
| Genotypes | Number | Amphotracin B | Itraconazole | Ketoconazol | Flucytosine | Fluconazole |
|---|---|---|---|---|---|---|
| A | 100 | 98 | 95 | 100 | 100 | 100 |
| B | 40 | 40 | 5 | 38 | 40 | 40 |
| C | 35 | 35 | 21 | 35 | 35 | 35 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Reproductive tract infections research · Probiotics and Fermented Foods
INTRODUCTION
Vaginal Candidiasis (VC) is one of the most prevalent human fungal infections, and is estimated to affect approximately 75% of all women at least once in their lifetime.1,2 The infection is caused by a group of Candida spp with C. albicans being the most dominant, whereas, Candida glabrata is frequently reported as the second or third in prevalence.3 However, other Candida spp. can also cause the infection including C. tropicalis, C. parapsilosis, C. krusei and C. dubliniensis.4 The infection is characterized by a diversified symptom that includes; itching, edema, erythema of the vulva, white vaginal curdy discharge and pain.5
VC is rare before puberty; its first episode could be related with the onset of sexual activity and increases dramatically in the second decade of life and beyond. Although, Candida is a member of the normal flora in vagina and other sites of the human body, many predisposing factors can lead to infection such as pregnancy, long term use of antibiotics, diabetes, use of corticosteroids, HIV infection, and immunocompromised situations.6,7
Clinical symptoms alone cannot diagnose VC accurately. Other infections such as bacterial vaginosis and vaginal trichomoniasis can confuse the diagnosis of VC.8 Symptoms that may be prevalent in these two infections can be found in women with VC.8 Therefore, microbiological work up using culture methods is recommended for diagnosis.
The occurrence of VC in Jordan was the subject of few studies. These studies showed that C. albicans was by far the most dominant etiologic agent responsible for this infection. Study by Abu-Elteen et al.9, showed that Candida albicans was the dominant species which was isolated from 51.3% of patients, followed by C. glabrata “with an isolation rate of 17.9%”. However, the genetic makeup of these isolates was not determined.
The identification of C. albicans to the strain level is sometimes important because there is a correlation between the Candida genotype and antifungal susceptibility. Antifungal susceptibility test results indicated that isolates of genotype A of C. albicans were significantly less susceptible to flucytosine than either C. albicans genotype B or C.10-12 Another study from Nigeria showed that genotype A resistance to fluconazole was quite high as compared to other genotypes.13 The aim of this study was to determine the antifungal susceptibility and gene diversity of C. albicans isolated from a group of Jordanian women with VC.
METHODS
Three hundred and twelve vaginal samples, positive for VC were collected from married women (18-55 years old) attending gynecology clinics in the following hospitals: Jordan, Specialty, and Islamic. Each of these hospitals contains more than 300 beds and out patient’s poly clinics. The study period lasted from July 2020 to December 2020. Demographic data and symptoms for each patient were derived from hospital files. High vaginal swabs were collected by gynecologists practicing in the respective hospital clinic.
Ethical Approval:
A written consent was obtained from each woman and the work was approved by the Ethical Committee of the Islamic Hospital, Jordan. This approval was issued in September 12, 2020 under the number 4/2020/2493.
Culture Procedure:
Sabouraud Dextrose Agar (SDA) medium was obtained from Oxoid- Irland and prepared by following the manufacturer’s instructions.14 After autoclaving, the medium was allowed to cool at 50°C before 5 mg/ dl of Chloramphenicol was added to it. The medium and the antibiotic were mixed and then poured into sterile petri dishes. Subsequently, the plates were stored at 2°C to 8°C for two weeks. Each collected vaginal swab was inoculated onto a plate of SDA in less than 24 hours of collection. All inoculated plates were incubated at 37°C for 48 hours and inspected for the presence of creamy to yellowish colonies which indicated the isolation of Candida spp.
Chromogenic agar culture:
A single colony was picked up from the SDA plate and streaked on chromogenic agar (Biolife, Italy). The plate was then incubated for 24-48 hrs. at 37°C. Then, candida isolates were classified according to their color as proposed by the manufacturer of the medium. Candida albicans ATCC 90028 was used as a reference and gave good growth on the differential medium with greenish to blueish pigmentation.
Sugar fermentation:
Various Candida spp. was identified by inoculating pure colonies taken from SDA into peptone liquid media (Oxoid- Irland). This medium contained phenol red as indicator, an inverted Durham’s tube and 2% of the following Carbohydrates: glucose, maltose, sucrose, Lactose, galactose, and trehalose; these sugars were incorporated separately into each peptone containing tube. Inoculated tubes were incubated at 37°C for 48 hours before the production of yellow color and gas were observed. Tubes that remained red were considered as negative for the respective sugar fermentation.
Genomic DNA Extraction:
Genomic DNA extraction was achieved using i-genomic BYF DNA Extraction Mini Kit (South Korea). A colony of C. albicans was picked up from SDA plate and inoculated into a tube containing 5ml yeast peptone dextrose (YPD) broth (Condalab, Spain). The tube was incubated at 37°C for overnight to obtain an optical density of 600 nm. The detail of the procedure was typically the same as described in the manufacturer’s instructions manual. In brief, the first step was to break down the cell wall by lysis and to extract its intracellular contents. Once this content was obtained, it was treated with enzymatic solution to clear the DNA captured. The captured content was stirred with 80% ethanol to separate out any precipitate. The DNA was then collected and further immersed in a slightly alkaline buffer, “ready to use”. The quality and concentration of the DNA material in the sample was assayed spectrophotometrically.
PCR Amplification:
Aliquots of 1 μl of the Genomic DNA Extract obtained for each C. albicans “purified as described above” was amplified by PCR on the bases of 25S rDNA using primers obtained from IDT (United States). For typing of C. albicans on the basis of ALT repeats two further primers were used. The sequence of the forward and reverse primers was described in Table-I. The program of the PCR was fixed as follows: one cycle of initial denaturation for 3 min, followed by 35 amplification cycles of denaturation at 94°C for 30 seconds, annealing at 59°C for 30 sec. and extension at 72°C for 30 seconds. The final extension was performed at 72°C for 10 minutes. The amplicon was separated by 1.5 % agarose gel electrophoresis supplemented with red safe. The system was run for 45 minutes at 450 voltage and then visualized using a gel documentation system (Cleaver Scientific, United Kingdom).
Consent to participate:
None of the data reported could lead to identification of patient.
Antifungal susceptibility:
Yeast colonies were suspended in 0.85% sterile saline solution to adjust to 0.5 McFarland standard. This inoculum contained 1 × 10^6^ to 5 × 10^6^ cells per ml. A sterile cotton swab was used to spread evenly 500 μl fungal suspension on a 150-mm Petri dish containing Mueller-Hinton agar supplemented with 2% glucose and 0.5 μg/ml methylene blue dye. E-test strips “obtained from AB. Biodisk, Solna, Sweden” were placed on plates that had been dried for 15 minutes at room temperature. The strip end with a lower concentration of the antifungal was positioned first and placed in almost equal angles to the adjacent strip. The strips were purchased from AB. Biodisk, Solna, Sweden. After incubation for 48 hours, the test was read using the zone of inhibition to mark the point at which the ellipse-shaped growth intersects with the strip, indicating an MIC value.
Isolates with MICs ≤ 8 ug ml^-1^ for fluconazole (FLU) and 5 flucytosine (FC), ≤ 0.125 lg ml^-1^ for itraconazole (ITR) and ketoconazole (KET), and ≤1 lg ml^-1^ for Amphotericin B (AmB) were considered susceptible. Isolates with minimum inhibitory concentration (MICs) ≥ 64 ug ml^-1^ for FLU, ≥32 ug ml^-1^ for 5FC, ≥1 ug ml^-1^ for itraconazole (ITR) or KET, and ≥2 ug ml^-1^ for AmB were considered resistant.12 Candida albicans ATCC 90028 was used as a Control each time a susceptibility test was performed. The Validity of the Test was ascertained by comparing the susceptibility results with CLSI standards.15
Statistical analysis:
One-way ANOVA and Chi-square tests were performed using the statistical SPSS package. Differences were considered significant at P < 0.05.
RESULTS
A total of 312 positive vaginal swab samples for Candida spp. were included in this investigation. Positive samples were found to be more prevalent in the age group stratified between 25 and 31 years of age (Table-II). No statistical significance was found to exist between the occurrence of the infection and the various age groups. Growth pattern of Candida spp. isolated on chromogenic agar and their biochemical identification testing revealed the presence of four Candida spp. among the isolates (Table-III). The Table demonstrates that out of 312 Candida spp. tested, 175 (56.0%) were positive for Candida albicans while the remaining 137 (44%) harbored Candida spp. other than albicans.
Women included in this work complained of the following symptoms “in a descending order”:
Burning sensation during urination (46.4%), Pruritus (44.8%), vaginal erythema (24.8%), and dyspareunia (7.2%). The most astonishing observation was the high prevalence rate of VC in non-pregnant (88.8%) as compared to pregnant women.
Using the CHI-SQUARE test it was calculated that there were no statistically significant results between VC and the detected symptoms except in case of pruritis and burning. In the current study, a total of 175 isolates were identified by phenotypic testing as C. albicans. These isolates were further typed using PCR with P-I and P-II primers. These primers were capable of determining the genotypes of the isolates based on variation in the 25S rDNA and repeated numbers of the ALT sequence (Table-IV and Table-V). The PCR amplified products of C. albicans using P-I, defined the DNA into three bands. These bands indicated the recovery of type A, B, and C of Candida albicans. Fig.1 shows that none of the PCR products in the current study demonstrated a band formation at the 1040 bp that corresponds to genotype D or at 1080 bp which indicated genotype E. However, band formation was obtained separately at 450 and 840 bp, in addition to the combined occurrence of two bands at 450 plus 840 bp; these bands indicated the recovery of A, B and C genotypes, respectively.
Amplification profiles of PCR products (25S rDNA) of Candida albicans isolates. (Genotype A: 450; genotype B: 840 bp; and genotype C: 450 and 840 bp) bp.
When results obtained using the two genetic markers were combined together; the outcome was the identification of nine distinct genotypes (Histogram 1). On the basis of the repeated numbers of ALT sequence in the PCR amplification, the RPS profiles generated by primer P-II, indicated the detection of 4 subtypes of isolates (Fig.2). These were: Subtype 2 as 698 bp long (7.14% of isolates), subtype 3 as 870 bp long (45.70% of isolates), subtype 2/3 as “698 and 870” bp long (40.0% of isolates) and subtype 3/4 as “870 and 1040” bp, (7.14% of isolates).
Percentage genotypic distribution of all C. albicans strain based on the two markers (P-I and P-II).
Genotyping identification for C. albicans strains by PCR targeting ALT repeats at the RPS using P-II primer.
Antifungal susceptibility testing of the various genotypes showed variation in the susceptibility pattern of the different genotypes recovered. All isolates of genotype A, B and C were sensitive to flucytosine and fluconazole. However, only five out 40 genotype B isolates and 21 out of 35 genotype C isolates were sensitive to itraconazole. This antifungal was found to be the least effective inhibitory agent among the 5-antifungal studied (Table-VI).
DISCUSSION
Only four Candida spp. were identified in this investigation as etiologic agent of vaginal candidiasis (Table-III); they were C. albicans, C. krusei, C. glabrata, and C. tropicalis. It was revealed that the highest frequency of vaginal candidiasis in the group of women studied was caused by C. albicans (56.0%). This observation is in agreement with most published literature from all over the world.9,10 In fact there is a variation in the type of Candida spp. recovered from vaginal swabs and this depends largely on the location as well as the population studied.
Predisposing factors for VC are numerous, including pregnancy and prior use of antibiotics. In the current work pregnancy was not found to be statistically significant factor in relation to the occurrence of infection, while the use of antibiotics was. High percentage (59%) of infected women diagnosed herein were found to have used antifungal drugs. This percentage is a lot higher than the 38% which was reported by Yano et al.11 In Jordan, antibiotics are officially considered as prescription drugs but in practice they are dealt with as over the counter drugs and this might explain why antibiotic use was found to be an important predisposing factor for vaginal candidiasis.
Among the women studied, the highest prevalence rate was detected in the age group stratified at 25 and 31 years of age. This is likely a reflection to the hormonal activity which takes place in this particular age that acts as a predisposing factor to infection. The relatively high proportions of VC in the postmenopausal (45 years or older) populations may reflect potential age-related to health conditions such as exogenous estrogen use to treat atrophy. Fischer and Bradford12 reported that nearly 50% of women above 50 years of age were diagnosed with VC attributed to hormonal replacement therapy.
Pruritus, burning, Erythema, and dyspareunia are among the most widely reported clinical features in VC. Burning, pruritis, and erythema were detected in (46%), (45%) and (25%) cases, respectively. The occurrence rate of these symptoms was a lot lower than those reported by Yano et al.11 but higher than those disclosed by Rathod et al.13 In the current work burning and pruritis were the only symptoms that gave statistically significant relationship with their number of occurrences.
For epidemiological reasons and treatment options, Odds et al.,14 suggested that it was of importance to clarify the taxonomic position of C. albicans and to determine the subpopulation within this species. C. albicans can be grouped into several genotypes by Southern hybridization, Pulsed-field gel electrophoresis (PFGE), and/ or Random Amplification of Polymorphic DNA (RAPD) techniques. From a cost point of view, Kanbe et al.15 suggested that identification of C. albicans by PCR, targeting the ALT repeat is more convenient than PFGE sequencing and RFLP techniques.
Tantivitayakul et al.16 indicated that C. albicans can be divided into four subtypes. This division is related to the presence and the size of transposable intron region in the large ribosomal subunit 25S rDNA. Based on this approach, these authors were able to identify different lengths of the PCR products as belonging to C. albicans, genotype A (450 bp), genotype B (840 bp), genotype C (450- and 840-bp), and genotype E (1400 bp). The same authors16 indicated the presence of association between C. albicans genotypes and fungal invasiveness as well as antifungal susceptibility.
To the best of our knowledge, reports on genotypic typing of C. albicans recovered from vaginal candidiasis in Jordan is seldom if at all presented. The current research contains information that has never been reported from Jordan. Genotype identification of C. albicans subtypes in this work were determined by PCR technique targeting 25S rDNA. The 175 C. albicans recovered herein were differentiated into three genotypes (A, B, and C). None of the isolates belonged to genotype (E or D) and genotype A accounted for 57.1%. These results contradicted those of Ali Shtayeh et al.7 and Gharaghani et al.17 who reported that the dominant C. albicans in their work belonged to Genotype C followed by Genotypes A and B. However, findings reported in our work regarding the genotypes are in agreement with those of Sawadogo et al.18
The ALT repeat sequence of the RPS revealed the presence of two patterns assigned to each of the three genotypes. In this study, nine types of C. albicans RPS were detected. These types were close to the 10 types identified by Sawadogo et al.18 but a bit higher than the 7 types reported by Amanloo et al.19 The Subtypes isolated in this study were A2 (5.71%), A3 (21.42%), A2/3 (22.86%), B3 (12.85%), B2/3 (10.0%), C2 (1.40%), C3 (11%) and C2/3 (7.14%). These findings are similar to those reported in other studies which characterized hundreds of C. albicans isolated from clinical samples including vaginal secretions, sputum, and blood 20. In the current investigation, A3/4 subtype was found to label a few isolates (7.1%). This observation was similar to the finding of Sawadogo et al.18 who detected this subtype in 6.3% of isolates. The dominance of subtype A3 among C. albicans isolated from clinical samples was also noted by Amanloo et al.19 and Iwata et al.20
Antifungal “in vitro” studies on the isolates revealed that vaginal candidiasis can be possibly treated to the same level of effectiveness using flucytosine and fluconazole. Whereas, Itraconazole was the least susceptible to all genotypes isolated. In fact, different results of susceptibilities were reported by different authors. For example, Zhu et al.21 found that genotype A strains were much less susceptible to flucytosine than either strains of genotype B or genotype C. On the other hand, Ali-Shtayeh et al.7 established that C. albicans genotype A were most resistant to fluconazole and flucytosine than B and C genotypes. Our results however are in agreement with those obtained by of Liu et al.22
Limitations:
One of the limitations of this work was the lack of correlation between various genotypes of C. albicans with the established risk factors like uncontrolled diabetes and impaired immune response. It would have been of value to have performed some gene sequencing procedure to identify the genes responsible for antifungal resistance.
CONCLUSION
This study showed that C. albicans was the highest in prevalence among Candida spp. recovered from cases of vaginal candidiasis in Jordanian women. Dominance of C. albicans was followed by C. krusei, C. glabrata, and C. tropicalis. Molecular genotyping characterized isolated C. albicans into three genotypes (A, B, and C). Using the ALT repeat sequences of the RPS, it was found that a genetic variation between C. albicans genotypes exist. Therefore, C. albicans depicted as etiologic agent of vaginal candidiasis were genetically diverse. Antifungal drugs were found to be in vitro effective against C. albicans to various levels depending on the genotype isolated. To our knowledge, this is the first report about the prevalence and antibiotics susceptibility of C.albicans isolated from vaginal candidiasis cases in Jordan
Author`s Contribution:
RMAG Responsible and accountable for accuracy and integrity of the work. Helped in the design and supervision of the project. Analysis of result.
RRMA Design and carried out the experimental work, made the literature search. Helped in the interpretation and analysis of results.
QMAS Suggested and supervised the research project, prepared the original manuscript.
All authors discussed the results and revised the manuscript critically for important intellectual content.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Willems HME Ahmed SS Liu J Xu Z Peters BM Vulvovaginal Candidiasis:A Current Understanding and Burning Questions J Fungi (Basel)20206127 doi:10.3390/jof 60100273210643810.3390/jof 6010027 PMC 7151053 · doi ↗ · pubmed ↗
- 2Raja A Ahmed A Fareed S Raja NS Tariq A Naqvi SRA Incidence of Vulvo vaginal candidiasis in young women:Experience from a tertiary care hospital, Karachi, Pakistan Pak J Pathol 2023344124127 doi:10.55629/pakjpathol.v 34i 4.77
- 3Tasneem U Siddiqui MT Faryal R Shah AA Prevalence and antifungal susceptibility of Candida species in a tertiary care hospital in Islamabad, Pakistan J Pak Med Assoc 201767798699128770873 · pubmed ↗
- 4Sardi JCO Silva DR Anibal PC Baldin JJCMC Ramalho SR Rosalen PL Vulvovaginal Candidiasis:Epidemiology and Risk Factors, Pathogenesis, Resistance, and New Therapeutic Options Curr Fungal Infect Rep 2021153240 doi:10.1007/s 12281-021-00415-9
- 5Rezk S Alqabbasi O Bacterial vaginosis, vulvovaginal candidiasis, trichomonal vaginitis and aerobic vaginitis in women from Egypt Germs 2023132130136 doi:10.18683/germs.2023.13763814425010.18683/germs.2023.1376 PMC 10746338 · doi ↗ · pubmed ↗
- 6Abu-Elteen KH Abdul Malek AM Abdul Wahid NA Prevalence and susceptibility of vaginal yeast isolates in Jordan Mycoses 1997405-617985 doi:10.1111/j.1439-0507.1997.tb 00211.x 947648510.1111/j.1439-0507.1997.tb 00211.x · doi ↗ · pubmed ↗
- 7Ali Shtayeh MS Jamous RM Alothman NHA Abu Baker MH Abu Zaitoun SY Mallah OY Genotyping and antifungal susceptibility of Candida albicans strains from patients with vulvovaginal and cutaneous candidiasis in Palestine Afr J Microbiol Res 2015913952959
- 8Emmanuel NN Romeo O Mebi AG Mark OO Scordino F Bessy EI Criseo G Genotyping and fluconazole susceptibility of Candida albicans strains from patients with vulvovaginal candidiasis in Jos. Nigeria Asian Pac J Trop Dis 201234850 doi:10.1016/S 2222-1808(12)60011-5