Coexistence of non-Hodgkin lymphoma and multisystem hydatid cysts; successful albendazole therapy for muscular hydatid cysts: A case report
Zainab Srouji, Zeina Talla, Zain Douba, Wael Alkhaleel, Ahmad Ghazal

TL;DR
A 44-year-old man with multiple hydatid cysts and non-Hodgkin lymphoma was successfully treated with albendazole, highlighting a rare medical case.
Contribution
This case report documents the first known coexistence of non-Hodgkin lymphoma and muscular hydatidosis, successfully treated with albendazole.
Findings
Albendazole successfully reduced the size of a muscular hydatid cyst in a patient.
Non-Hodgkin lymphoma was diagnosed alongside multiple hydatid cysts in a single patient.
The coexistence of non-Hodgkin lymphoma and muscular hydatidosis is unprecedented in medical literature.
Abstract
“Hydatid cyst” or cystic Echinococcosis is a parasitic infection caused by the larval stage of Echinococcus granulosus. The liver and lungs are the most common sites to occur. Incidence in muscles is exceptionally rare. Surgery has been the traditional approach for treatment of cystic echinococcusis. We report a rare case of 44 years old man with multiple hydatid cysts; liver, lungs, paraspinal muscles. The muscular cyst had manifested as a swelling in his back and was the principal clinical presentation as it caused pain and discomfort. He was treated with Albendazole, and a thoracic surgery for the management of the lung cysts had been performed. On admission and after his surgery, lymphadenopathy had manifested and following adequate diagnostic modalities he was diagnosed with Non-Hodgkin lymphoma. Then, after three months, physical examination revealed significant reduction in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
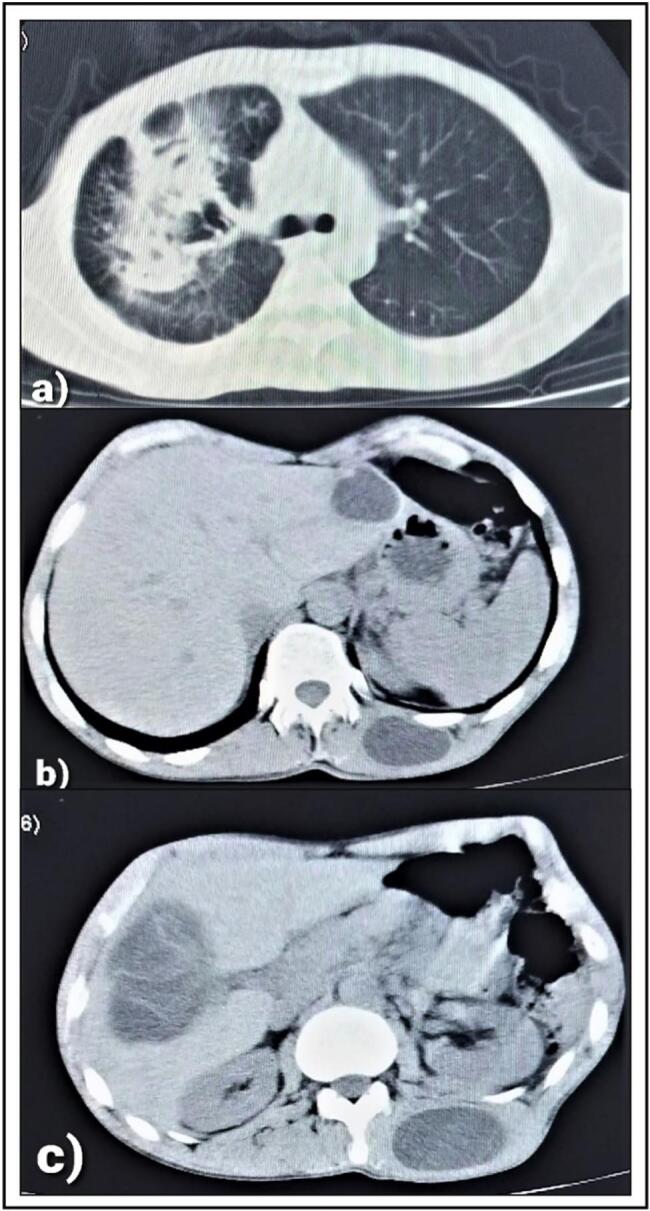 Figure 1
Figure 1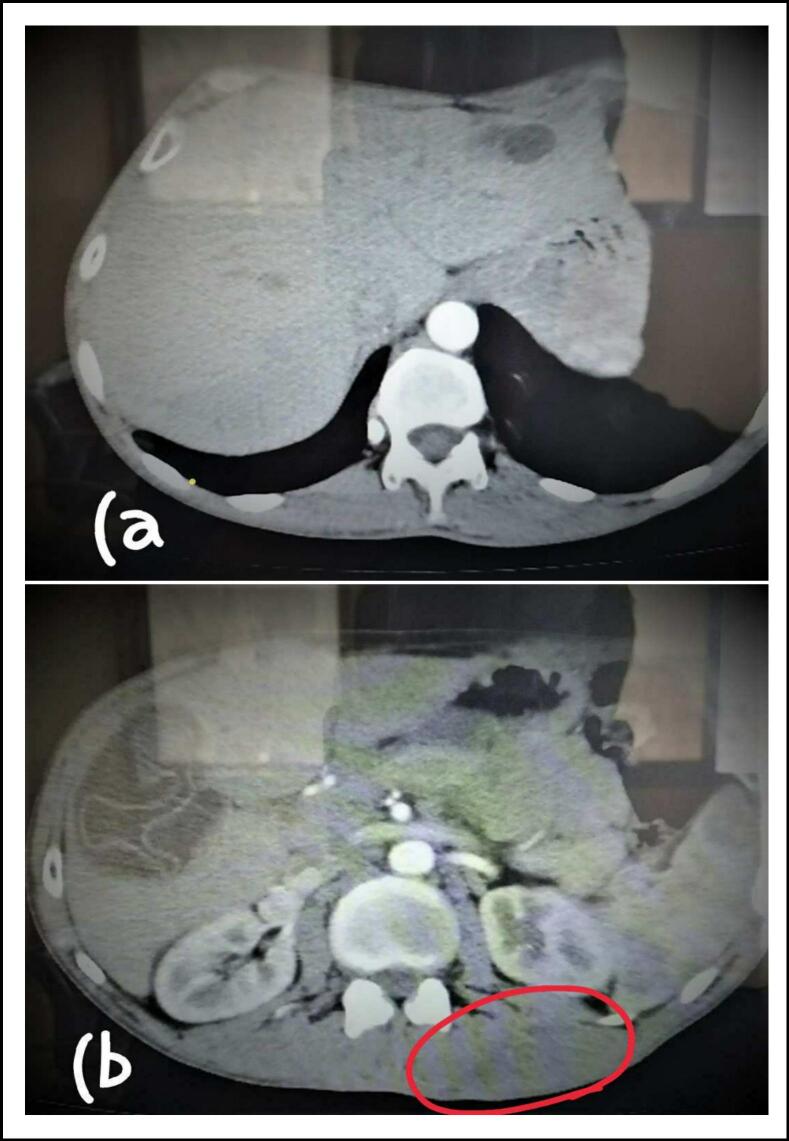 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Congenital Anomalies and Fetal Surgery · Parasitic Infections and Diagnostics
Introduction
1
Cystic hydatidosis is a zoonotic disease caused by the larvae of echinococcus species, in which humans are infected through the consumption of food and water contaminated with the eggs of parasites of the echinococcus granulosus or through direct contact with the host [1,2].
Although hydatid cyst can occur almost anywhere in the human body, it usually affects the liver (∼70 %) followed by the lungs (∼20 %), whereas musculoskeletal involvement is rare and contributes to (∼0.5 %–5 %) of cases [3].
Hydatid cysts are usually asymptomatic, and the symptoms usually develop depending on the size of the cyst and vary according to its location [1]. Hydatid cysts in the muscles show no characteristic clinical signs and symptoms [4].
The standard therapy of hydatid cysts is surgery while medical treatment plays a more significant role in inoperable patients and multiple organ involvement [5].
Our report handles a case of 44 years old man with multiple hydatid cysts in liver, lungs, paraspinal muscles and Non-Hodgkin lymphoma.
Prior reports on muscular localization of hydatid cysts have managed it principally through various surgical techniques, but our report is the first to mention association between muscular hydatidosis and Non-Hodgkin lymphoma in addition to an expected response for treatment with albendazole.
Method
2
This case has been reported in line with the SCARE criteria [6].
Presentation of case
3
A 44 years old man presented to our surgical unit with 1-year history of a painful swelling in his back under the left scapula.
His past medical history included cough, viscous bloody sputum, fever and extreme fatigue; the previous symptoms manifested a year ago and lasted for three months and then improved gradually.
He had no surgical or family histories. His appetite was good with minimal weight loss, smoked 35 packs/year and lived in a rural area.
Examination of the mass revealed mild tenderness and fluctuation.
A laboratory examination, including a complete blood cell count, serum chemistries and a coagulation profile showed values within normal ranges.
Initially, ultrasound examination of the lump demonstrated cystic formation, smooth edges, turbid content with membranes. The dimensions were 3.5 × 6.5 cm; most likely to be a hydatid cyst. The CT showed two open cysts in the right lung with air-fluid level, two cysts in the liver; 8 cm in the right lobe and 4 cm in the left lobe, in addition to the cyst in the paraspinal muscles on the left side (Fig. 1).Fig. 1CT scan reveals: (A) two open cysts in the right lung. (B) 4 cm cyst in the left hepatic lobe and the cyst in paraspinal muscles on the left side of the patient. (C) 8 cm cyst in the right hepatic lobe and the cyst in paraspinal muscles on the left side of the patient.Fig. 1
The patient was started on albendazole and it was decided to operate on the lung first. A right intercostal incision was made and two open cysts located in the right upper lobe were found. Their cavities were opened, the germinal membranes were excised, the fistulae were closed using vicryl and the cavities were reclosed.
Following thoracic surgery and during hospitalization period, the patient started complaining about a pain in the groin, palpation revealed lymph nodes enlargements in the inguinal area, the neck and the axilla.
US findings for the lymph nodes were suspicious. An excisional biopsy from the right axilla was taken and the pathology report came back with Non-Hodgkin lymphoma (T cell rich large B cell lymphoma).
Afterwards, contact with the patient was lost for two months for his own circumstances, but during this period, he continued on taking Albendazole. When he returned for follow up, physical examination revealed that the mass on the left side of his back had decreased significantly in size and was barely palpable.
Multislice CT showed regression of the cyst in the paraspinal muscles on the left side, and the cyst in the left hepatic lobe had reduced in size to 1 cm in diameter with no change in the cyst of the right lobe. These findings came after 3 months of treatment with Albendazole; (one month before surgery and two months after). The CT also revealed lymphadenopathy in the mediastinum; the largest measured 1 cm in diameter, and lymph nodes aggregation in the right and left axillae, the largest were in the left side 16 × 27 mm (Fig. 2).Fig. 2. Multislice CT reveals: (A) the cyst in the left lobe that has reduced to 1 cm. (B) The cyst in the right lobe and regression of the cyst in paraspinal muscles on the left side (red circle). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2
The oncologist decided to operate on the liver cyst before administration of chemotherapy, laparoscopy was done to remove the cyst in the right hepatic lobe and the patient received postoperative pharmacological therapy with Albendazole. He was then followed up by oncology department and received his chemotherapy.
Discussion
4
Echinococcal disease is a worldwide distributed parasitic infection caused by the tapeworm echinococcus with higher incidence rates at endemic regions such as the Mediterranean and the middle east including our country, Syria [7].
The most common sites for cysts to form are the liver and the lungs, and less frequently, the muscles.
When cysts form at the expense of back muscles, pain and discomfort especially while lying down will develop, as in our patient. It could also exhibit compressive neurological symptoms.
Surgery has been the traditional approach for treatment of cystic hydatidosis; chemical therapy may be used for definitive management in selected cases [8]. It is also a useful adjuvant therapy to surgery and percutaneous treatment.
Albendazole is the primary antiparasitic agent for treatment of echinococcus granulosus [9].
Cumulative experience with albendazole suggests that treatment leads to cyst resolution in up to 30 % of patients, size reduction in another 30 % to 50 % and no change in 20 % to 40 % [9].
Frankly, it was decided to operate on the muscular cyst, but due to the fact that the patient lived in a rural distant area and the difficulties in accessing prompt medical help in our afflicted country, his delay came back with benefit as his back cyst doesn't need excision anymore.
The cyst in the left hepatic lobe was not removed due to its small size.
Prior reports on muscular hydatid cysts had managed it mainly surgically. However, to our knowledge, the medical literature contains only one report of a complete cure of muscular hydatidosis only by means of albendazole therapy [10].
Non-Hodgkin lymphomas (NHLs) are tumors originating from lymphoid tissues, mainly of lymph nodes. NHL is the most prevalent hematopoietic neoplasm, representing approximately 4.3 % of all cancer diagnoses. Chemotherapy represents the main treatment.
When lymphadenopathy had manifested after thoracic surgery, it raised the suspicion of an underlying problem, so proper diagnostic modalities were performed which led eventually to the diagnosis of the tumor.
Although coexistence of NHL and hepatic cystic disease has been reported before, association between NHL and muscular hydatidosis has not been reported before.
Conclusion
5
Here we report a coexistence of NHL and multiple hydatid cysts in one case. This association is rare, and to our knowledge has not been reported before. In addition to the unprecedented response for albendazole therapy, on the other hand our patient was treated successfully for both conditions without any signs of relapse.
In endemic countries, cystic hydatid disease should be considered as a differential diagnosis for every cystic lesion in any anatomical location [2].
Here we present a successful treatment for multiple hydatid cysts; in which albendazole has played a significant role, in addition to the diagnosis of the lymphoma in the course of managing the parasitic infection.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval was waived by the board of Faculty of Medicine at Aleppo University for this type of articles “case report”.
Funding
None.
Author contribution
Zainab Srouji: Writing original draft, review and editing, visualization, literature review, and the corresponding author who submitted the paper for publication.
Zeina Talla: Writing, review and editing, visualization, literature review.
Zein Douba: Supervision, validation and reviewing.
Wael Alkhaleel: Conceptualization, investigation, resources and visualization.
Ahmad Ghazal: Performed and supervised the operation, conceptualization and reviewing.
All authors read and approved the final manuscript.
Guarantor
Zainab Srouji.
Research registration number
N/A.
Conflict of interest statement
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Douba Z.Sinno J.A.Jawish H.Hakim N.Mouselli A.Shihade M.B.Unusual localizations of hydatid cysts: a rare case report from Syria J. Surg. Case Rep. [Internet]202010 Oct 1, 2020[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/33133511/10.1093/jscr/rjaa 438PMC 758831133133511 · doi ↗ · pubmed ↗
- 2Sadeghian H.Motiei-Langroudi R.Hydatid cyst in the lumbar paravertebral muscle: a case report Cureus [Internet]118Aug 9, 2019[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/31608188/10.7759/cureus.5353 PMC 678321031608188 · doi ↗ · pubmed ↗
- 3Niazi A.Alibraheem A.Al-Mouakeh A.Abouzied M.K.Basha S.R.Suliman S.Gluteal muscles primary hydatid cyst after cortical bone destruction in the sacrum Ann Med Surg (Lond) [Internet]59Nov 1, 20208992[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/32994990/3299499010.1016/j.amsu.2020.09.019PMC 7501496 · doi ↗ · pubmed ↗
- 4Özdemir M.Kavak R.P.Kavak N.Akdur N.C.Primary hydatid cyst in the adductor magnus muscle BJR Case Rep. [Internet]63Sep 202020200019[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/32922845/10.1259/bjrcr.20200019 PMC 746574132922845 · doi ↗ · pubmed ↗
- 5Jamshidi M.Mohraz M.Zangeneh M.Jamshidi A.The effect of combination therapy with albendazole and praziquantel on hydatid cyst treatment Parasitol. Res. [Internet]1031 Jun 2008195199[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/18404278/1840427810.1007/s 00436-008-0954-z · doi ↗ · pubmed ↗
- 6Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg. [Internet]1095 May 1, 20231136[cited 2024 Jul 3]. (Available from: /pmc/articles/PMC 10389401/)3701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗
- 7Zazo A.Zazo R.Shashaa M.N.Alkarrash M.S.Brimo Alsaman M.Z.Niazi A.Uncommon musculoskeletal femoral hydatid cyst disturbs a female for a year: case report Ann. Med. Surg. (Lond.) [Internet]55Jul 1, 20203032[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/32435477/3243547710.1016/j.amsu.2020.04.025PMC 7231815 · doi ↗ · pubmed ↗
- 8Muratori F.de Gori M.D’Arienzo A.Bettini L.Roselli G.Campanacci D.A.Hydatid cyst in the vastus lateralis muscle: a case report Clin. Cases Miner. Bone Metab. [Internet]142Aug 1, 2017262264[cited 2024 Jun 16]. Available from:https://pubmed.ncbi.nlm.nih.gov/29263748/2926374810.11138/ccmbm/2017.14.2.262PMC 5726224 · doi ↗ · pubmed ↗