A Rare Case of Gastroparesis-Induced Takotsubo Cardiomyopathy
Joane Titus, Jacob Bentley, Kristin L Recker, Olga Karasik

TL;DR
A rare case shows that severe vomiting from gastroparesis can trigger takotsubo cardiomyopathy, a heart condition usually caused by stress.
Contribution
This case report identifies gastroparesis-induced vomiting as a novel trigger for takotsubo cardiomyopathy.
Findings
A patient with gastroparesis developed takotsubo cardiomyopathy following forceful vomiting.
The condition occurred without any emotional or physical stressors typically associated with TCM.
This case suggests non-traditional triggers should be considered in TCM diagnosis.
Abstract
This case report includes an extremely rare and intriguing presentation of takotsubo cardiomyopathy (TCM), triggered by forceful vomiting in the setting of gastroparesis, a condition characterized by delayed gastric emptying. TCM is a reversible form of cardiomyopathy that typically occurs following a severe emotional or physical stressor. In this exceptional case, we present a patient with an acute severe episode of gastroparesis, followed by TCM, devoid of any recognizable emotional or physical stressors. This case highlights the importance of considering non-traditional triggers in TCM cases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
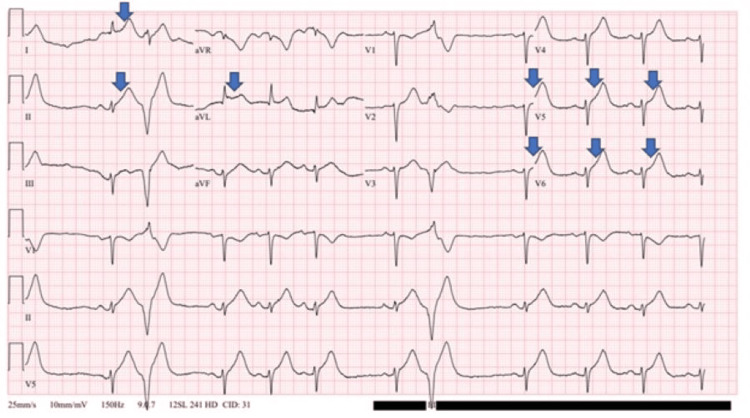 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTakotsubo Cardiomyopathy and Associated Phenomena · Neurosurgical Procedures and Complications · Alcoholism and Thiamine Deficiency
Introduction
Takotsubo cardiomyopathy (TCM), also known as stress-induced cardiomyopathy or "broken heart syndrome," is a reversible form of heart muscle dysfunction characterized by the sudden onset of left ventricle apical hypokinesia, akinesia, or dyskinesia [1]. TCM is typically associated with severe emotional or physical stressors, such as the death of a loved one, a natural disaster, or a medical illness [1]. However, the onset of TCM secondary to gastrointestinal (GI) disorders like gastroparesis is very rare and has not yet been documented. We present a case of gastroparesis-induced TCM to highlight this uncommon clinical association.
Case presentation
Our patient was a 45-year-old woman with a medical history of non-insulin-dependent diabetes mellitus and gastroparesis, on ondansetron and metoclopramide. She presented to the Emergency Department due to persistent nausea and vomiting, along with chest tightness, diaphoresis, palpitations, shortness of breath, abdominal discomfort, and chills for three days. She reported forceful vomiting around 10-15 times per day prior to admission. On arrival, her vitals included a blood pressure of 198/88 mmHg, an initial troponin of 518 ng/L followed by a second troponin of 3443 ng/L two hours later. Her initial electrocardiogram (EKG) demonstrated a heart rate of 69 bpm with marked sinus arrhythmia and occasional premature ventricular complexes (PVCs), in addition to ST elevations in leads I, II, aVL, V5, and V6, suggestive of acute inferolateral myocardial infarction or injury (Figure 1).
EKG on initial presentation demonstrating sinus arrhythmia with ST elevation in the inferolateral leads indicated by arrows, with occasional PVCsEKG: Electrocardiogram; PVCs: Premature ventricular complexes
Due to the acute onset of shortness of breath, chest discomfort, and GI symptoms, both computed tomography angiography (CTA) and computed tomography (CT) of the abdomen were obtained. CTA was negative for pulmonary embolus, and the CT of the abdomen was negative except for an incidental finding of subaortic stenosis. Aspartate aminotransferase (AST) was 33 units/L, alanine aminotransferase (ALT) was 13 units/L, and alkaline phosphatase was 49 units/L. An echocardiogram showed an ejection fraction of 30-35% with mild to moderate dilation of the left atrium, mild mitral regurgitation, no pericardial effusion, and most notably, apical ballooning of the apex suggestive of takotsubo syndrome (Video 1). Left heart catheterization revealed a discrete lesion in the left anterior descending artery, which did not warrant percutaneous intervention.
Echocardiogram showing a reduced ejection fraction of 30-35% with apical ballooning of the apex suggestive of takotsubo syndrome
Over the course of her hospitalization, the patient's troponin peaked at 7828 ng/L approximately six hours after arrival at the hospital before trending down. Her repeat EKG again showed elevations in the inferior and lateral leads. The persistently elevated troponin level and EKG findings are not uncommon for patients with TCM. For her gastroparesis, metoclopramide was resumed at a dose of 10 mg three times daily, and ondansetron was initiated at a dose of 4 mg every six hours as needed. The patient was eventually discharged with metoclopramide 10 mg three times daily as needed and ondansetron 4 mg every eight hours as needed. During her stay, she had improvement and resolution of her chest pain, nausea, and vomiting. The final recommendations were for the patient to be sent home on goal-directed medical therapy (GDMT) and a life vest. GDMT consisted of metoprolol succinate 12.5 mg once daily, spironolactone 12.5 mg once daily, and empagliflozin 10 mg once daily. Sacubitril/valsartan was also recommended for the patient, but she was unable to afford the medication due to a lack of insurance. Within a couple of months, the patient had clinically recovered and was able to return to her baseline activity.
Discussion
TCM is a result of severe stressors which can lead to heart dysfunction. In most cases, TCM is associated with acute emotional or physical stressors such as sepsis, trauma, or significant emotional events [1]. There have been few reported cases of TCM associated with forceful vomiting secondary to acute-on-chronic vomiting [2] and cyclical vomiting syndrome [3]. However, this is the first reported case that presents vomiting secondary to gastroparesis as a cause of TCM. The exact pathophysiological mechanisms by which forceful vomiting leads to TCM remain unclear. The prevailing hypothesis suggests that TCM results from elevated levels of plasma catecholamines and circulating metabolites due to stress [4]. Recognizing the diverse range of stressors that can precipitate TCM is crucial for clinicians. The overlap in clinical presentation between TCM and acute myocardial infarction (AMI) means that prompt and accurate diagnosis is essential to manage the condition effectively [1]. The risk of complications, such as heart failure and stroke, has been found to be higher in hospitalized TCM patients when compared to AMI patients, underscoring the importance of timely intervention [5].
Due to the risk of severe complications from TCM, it is imperative that a diagnosis be made expeditiously to identify the trigger and initiate treatment to resolve it. The incidence of TCM is about 0.02% of all hospitalizations in the United States, with an increased propensity in elderly women, smokers, alcohol abusers, and those with anxiety states [6,7]. For an official diagnosis of TCM based on the Mayo Clinic criteria, the following conditions must be met: suspicion of AMI based on the clinical presentation and ST-segment elevation noted on an EKG [6]. Then, imaging confirms ventriculography or an echocardiogram demonstrating transient hypokinesia or akinesia of the ventricle [6]. Then, heart catheterization or arteriography confirms normal coronary arteries, with less than 50% luminal narrowing in all coronary arteries [6]. Lastly, other conditions that may mimic TCM (such as myocarditis) should be excluded. In our case, this patient met all of the Mayo Clinic criteria for TCM. Her lack of recent illness, fever, or pericardial effusion helped exclude myocarditis as a likely cause.
With a review of the literature, there were other GI-related cases of TCM. One involved an 85-year-old man who was admitted for ileus with severe abdominal pain and vomiting. Ventriculography revealed an ejection fraction of 33% with apical dilation, supporting TCM. He was treated with similar medications and discharged without significant adverse events [8]. Another GI case involved a 27-year-old man with a history of alcohol abuse who developed TCM as a complication of pancreatitis in the absence of vomiting [9]. Both cases demonstrate the need for consideration of GI conditions contributing to the development of TCM.
Conclusions
TCM is rare, and its etiology is not well understood, but this case highlights the broad spectrum of potential causes for TCM. By detailing this atypical presentation, the authors want to emphasize the need to consider GI causes of TCM when evaluating a patient with no other risk factors and how treating gastroparesis will contribute to decreased morbidity in these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takotsubo cardiomyopathy J Gen Intern Med Sealove BA Tiyyagura S Fuster V 190419082320081868868110.1007/s 11606-008-0744-4PMC 2585677 · doi ↗ · pubmed ↗
- 2Takotsubo cardiomyopathy triggered by severe vomiting Am J Med Awais M Hernandez RA Bach DS 04121200810.1016/j.amjmed.2008.07.01919028187 · doi ↗ · pubmed ↗
- 3Recurrent takotsubo cardiomyopathy secondary to cyclical vomiting syndrome Cureus Akram A Kazi A Hyder S Saucier S 016202410.7759/cureus.60764 PMC 1118869638903280 · doi ↗ · pubmed ↗
- 4Stress (takotsubo) cardiomyopathy--a novel pathophysiological hypothesis to explain catecholamine-induced acute myocardial stunning Nat Clin Pract Cardiovasc Med Lyon AR Rees PS Prasad S Poole-Wilson PA Harding SE 2229520081809467010.1038/ncpcardio 1066 · doi ↗ · pubmed ↗
- 5Comparison of complications and in-hospital mortality in takotsubo (apical ballooning/stress) cardiomyopathy versus acute myocardial infarction Am J Cardiol Vallabhajosyula S Barsness GW Herrmann J Anavekar NS Gulati R Prasad A 293513220203276296310.1016/j.amjcard.2020.07.015 · doi ↗ · pubmed ↗
- 6Takotsubo cardiomyopathy: pathophysiology, diagnosis and treatment World J Cardiol Komamura K Fukui M Iwasaku T Hirotani S Masuyama T 602609620142506802010.4330/wjc.v 6.i 7.602PMC 4110608 · doi ↗ · pubmed ↗
- 7Prevalence of takotsubo cardiomyopathy in the United States Am Heart J Deshmukh A Kumar G Pant S Rihal C Murugiah K Mehta JL 667116420122279528410.1016/j.ahj.2012.03.020 · doi ↗ · pubmed ↗
- 8Takotsubo cardiomyopathy in a patient with ileus: a case report BMC Cardiovasc Disord Guo CC Chou NS 2661720172904191010.1186/s 12872-017-0700-5PMC 5645888 · doi ↗ · pubmed ↗