Small Intestinal Complications of Intestinal Transplant-Associated Microangiopathy Post-stem Cell Transplantation
Daisuke Kametaka, Masaya Iwamuro, Takehiro Tanaka, Ken-ichi Matsuoka, Motoyuki Otsuka

TL;DR
This paper reports a rare case of intestinal complications following a stem cell transplant, highlighting new insights into managing similar patients.
Contribution
The first report presenting images of possible small intestinal lesions in intestinal transplant-associated microangiopathy.
Findings
A patient developed intestinal transplant-associated microangiopathy (iTAM) seven weeks post-transplantation.
Video capsule enteroscopy revealed multiple erosions and shallow ulcers in the jejunum and ileum.
The presented images may aid in managing patients with similar conditions.
Abstract
We present the case of a patient who underwent human leukocyte antigen-haploidentical transplantation for T-cell acute lymphoblastic leukemia. Seven weeks after transplantation, the patient developed intestinal transplant-associated microangiopathy (iTAM). Although the iTAM was resolved temporarily, it recurred. Video capsule enteroscopy revealed multiple erosions and shallow ulcers in the jejunum and ileum. To the best of our knowledge, this is the first report to present images of possible small intestinal lesions in iTAM. The small intestinal mucosal images presented herein may potentially aid in the management of similar patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
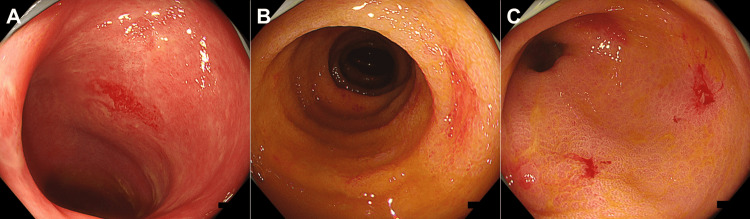 Figure 1
Figure 1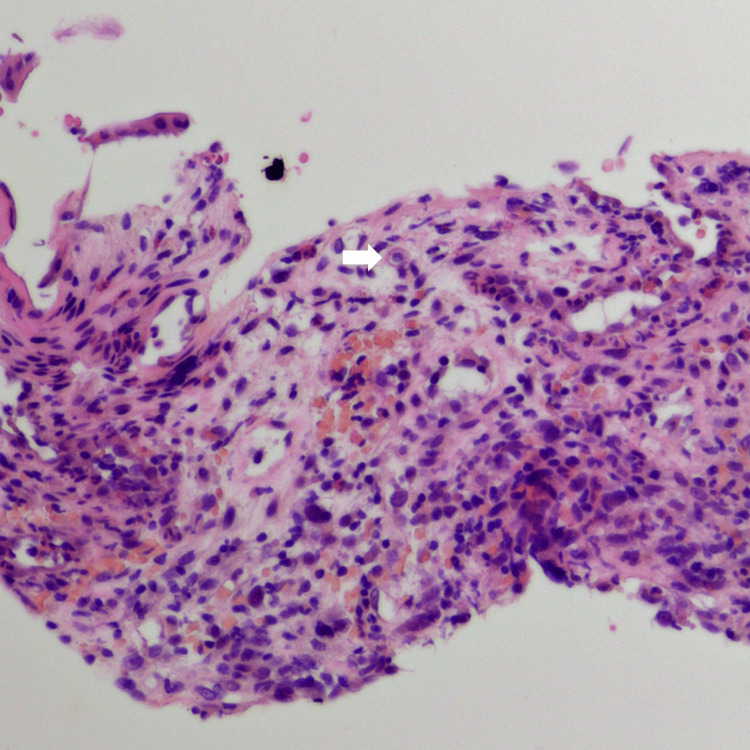 Figure 2
Figure 2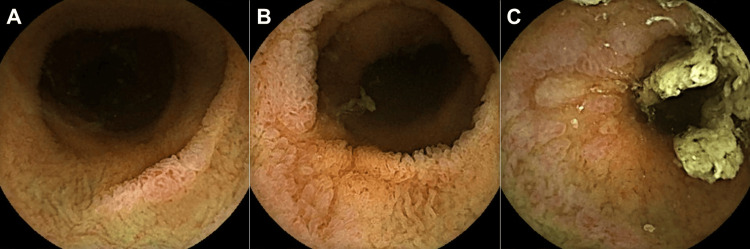 Figure 3
Figure 3| Blood test results (units) | Patient value | Reference range |
| White blood cells (/µL) | 3,440 | 3,300–8,600 |
| Neutrophils (%) | 32.5 | 40–70 |
| Lymphocytes (%) | 35 | 16.5–49.5 |
| Monocytes (%) | 28.5 | 2–10 |
| Hemoglobin (g/dL) | 7.9 | 11.6–14.8 |
| Schistocytes (%) | 2.8 | |
| Platelets (/µL) | 1.6 × 104 | 15.8 × 104–34.8 × 104 |
| Total protein (g/dL) | 4.9 | 6.6–8.1 |
| Albumin (g/dL) | 2.5 | 4.1–5.1 |
| Creatinine (mg/dL) | 0.74 | 0.46–0.79 |
| Lactate dehydrogenase (U/L) | 167 | 124–222 |
| Sodium (mmol/L) | 136 | 138–145 |
| Potassium (mmol/L) | 3.9 | 3.6–4.8 |
| Aspartate aminotransferase (U/L) | 19 | 13–30 |
| Alanine aminotransferase (U/L) | 32 | 7–2 |
| γ-Glutamyl transpeptidase (U/L) | 176 | 9–32 |
| C-reactive protein (mg/dL) | 1.77 | 0–0.15 |
| D-dimer (µg/mL) | 12.3 | 0–0.9 |
| Haptoglobin (mg/dL) | 203 | 19–170 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Renal Transplantation Outcomes and Treatments · Clinical Nutrition and Gastroenterology
Introduction
Intestinal transplant-associated microangiopathy (iTAM) is a condition characterized by damage to the small blood vessels (microangiopathy) in the intestine following a transplantation procedure, particularly after stem cell transplantation for blood disorders [1-4]. This damage can lead to complications such as tissue injury, impaired blood flow, and, ultimately, organ dysfunction. iTAM is a severe complication that can significantly affect the success of the transplant and the overall health of patients [5]. Treatment for iTAM typically involves a multifaceted approach to address the underlying causes and manage symptoms. It is important to note that the treatment differs from other intestinal complications, such as graft-versus-host disease (GVHD) or cytomegalovirus infection, that occur after hematopoietic stem cell transplantation [6-8]. Therefore, appropriate diagnostic and treatment interventions for iTAM are crucial for managing post-hematopoietic stem cell transplantation recipients. Although iTAM can cause mucosal damage in the small intestine, endoscopic images of the small intestinal lesions have not yet been reported. Herein, we present the case of a patient in whom small intestinal lesions were visualized using video capsule enteroscopy.
Case presentation
A Japanese man was diagnosed with acute T-cell lymphoblastic leukemia at the age of 23. He experienced refractory relapse and underwent the following treatments: umbilical cord blood transplantation at the age of 25, human leukocyte antigen (HLA)-haploidentical transplantation with post-transplant cyclophosphamide at the age of 27, a second umbilical cord blood transplantation at the age of 28, and HLA-haploidentical transplantation with post-transplant cyclophosphamide at the age of 29. The patient was hospitalized seven weeks after the last transplantation because of increased diarrhea. A colonoscopy revealed villous atrophy of the ileal mucosa. Edematous and coarse mucosa were observed throughout the colon, with erosion in the descending colon and multiple shallow ulcers in the rectum (Figure 1). Histopathological examination of endoscopic biopsy samples from the ileum to the rectum revealed denudation and atrophy of epithelial cells with areas of fibrosis. Hypertrophy of the vascular endothelium was also observed, leading to a diagnosis of iTAM (Figure 2). Additionally, a small number of cells tested positive for cytomegalovirus on immunohistochemical staining, suggesting concurrent cytomegalovirus enteritis. Tacrolimus was discontinued based on the diagnosis of iTAM. Ganciclovir was administered intravenously for cytomegalovirus enteritis.
Colonoscopy images performed seven weeks after HLA-haploidentical transplantation(A) The mucosa of the ileum exhibits villous atrophy. (B and C) Edematous and coarse mucosa was observed throughout the entire colon, with erosions in the descending colon and multiple shallow ulcers in the rectum.HLA, human leukocyte antigen
A pathology image of the colonic mucosaHypertrophy of the vascular endothelium is observed, leading to a diagnosis of iTAM (arrow).iTAM, intestinal transplant-associated microangiopathy
Additionally, prednisolone (1 mg/kg body weight) was administered to treat suspected concurrent GVHD. At 24 weeks post-transplantation, colonoscopy showed an improvement in mucosal damage, with no histopathological findings of iTAM or the presence of cytomegalovirus-positive cells. The patient was discharged; however, 30 weeks post-transplantation, he presented with watery diarrhea and bloody stools, leading to readmission. A colonoscopy revealed scattered erythematous erosions throughout the colon, which were suspected to be the source of the bleeding. A biopsy revealed segmental damage with epithelial apoptosis, loss of glands, and total mucosa denudation, indicating iTAM recurrence. Video capsule enteroscopy revealed multiple erosions and shallow ulcers, mainly in the folds of the jejunum and ileum (Figure 3). The blood test results at the time of the video capsule enteroscopy are shown in Table 1. Subsequently, the patient participated in a clinical trial of antibody therapy.
Video capsule enteroscopy imagesMultiple erosions and shallow ulcers are observed mainly on Kerckring’s folds of the jejunum and ileum.
Discussion
Endoscopic images of iTAM have not been sufficiently reported. Yamada-Fujiwara et al. reported nine cases of iTAM, of which six were concurrent with GVHD. They described mucosal petechiae and diffuse exfoliation as the criteria for the clinical diagnosis of iTAM based on colonoscopic findings [9]. Yamamoto et al. presented an endoscopic image of a case showing segmental longitudinal ulcerations with hemorrhagic edematous mucosa in the transverse colon, suggesting that iTAM may present endoscopic images resembling ischemic colitis [10]. In a previous study by Yamada et al., four patients were diagnosed with iTAM [11]. Concomitant GVHD was consistently observed in all the cases. Endoscopic examination revealed erythema and edema, along with erosions and ulcerations. Another investigation by Nishida et al. involving nine patients with concurrent iTAM and GVHD documented a range of gastrointestinal tract anomalies, notably mucosal edema, erythema, ulceration, and hemorrhage [12]. In light of the limited reports on endoscopic imaging of iTAM, we recently conducted a comprehensive investigation and reported the endoscopic findings in 14 cases of iTAM [13]. All the patients had erythematous mucosa in the gastrointestinal tract. Endoscopic findings in iTAM included erosions (93%), ulcers (64%), mucosal edema (64%), granular mucosa (64%), and villous atrophy (29%).
To date, endoscopic images of small intestinal lesions have not been reported, although iTAM can manifest as lesions in the small intestine [11]. This is the first report to present video capsule enteroscopy images of possible jejunal and ileal iTAM lesions. GVHD is characterized by extensive lymphocyte infiltration within the mucosa and infiltration of CD8+ T lymphocytes into the epithelium, along with apoptosis within the crypts [14], resulting in diffuse rather than regional changes in the gastrointestinal mucosa. In contrast, iTAM involves damage to small blood vessels (microangiopathy) in the intestine, leading to ischemia and subsequent wedge-shaped segmental tissue injury [3,4,15]. Therefore, the multiple erosions and shallow ulcers observed in this case, without extensive mucosal injuries such as edema, erythema, and villous atrophy, are consistent with small intestinal lesions of iTAM.
There are some limitations to our study that may impact the interpretation of the small intestinal lesions. Firstly, there are no established pathologic criteria for diagnosing iTAM. Secondly, histological diagnosis via biopsy was not performed for small intestinal lesions in this case due to obtaining images through video capsule enteroscopy. It is noteworthy that GVHD, cytomegalovirus infection, and iTAM can co-occur. Specifically, cytomegalovirus-positive cells were detected in the colorectum during the course of this case, and steroid treatment was initiated, suspecting GVHD. Consistent with our previous report, we diagnosed iTAM of the colorectum based on hypertrophy of the vascular endothelium (Figure 2). However, due to the patient not meeting the symptoms of TA-TMA [16] and the lack of established pathologic criteria, we cannot definitively assert whether the small intestinal lesions are iTAM or related to GVHD or cytomegalovirus infection in the small intestine. However, post-HSCT patients often have compromised overall health, and performing balloon-assisted enteroscopy to obtain small intestinal tissue for diagnosis carries a significant risk. Therefore, small intestinal mucosa evaluation using video capsule enteroscopy is a less invasive option for gastrointestinal assessment in post-hematopoietic stem cell transplant patients. Thirdly, the clinical significance of small intestinal lesions has not been clearly established. Recently, within TA-TMA, attention has focused on high-risk, complement-mediated, untreated transplant-associated thrombotic microangiopathy, which leads to dismal outcomes due to multi-organ dysfunction syndrome [17]. This case not only fails to meet the criteria for high-risk TA-TMA but also does not meet the standards for TA-TMA [16], indicating a clinically mild severity. The impact of small intestinal lesions on the clinical course of iTAM and the types of small intestinal lesions observed in severe cases remain unclear. Addressing these issues will require a further accumulation of cases. Nonetheless, this report represents the first presentation of endoscopic images of possible small intestinal lesions in iTAM, and we anticipate that the mucosal images presented here will contribute to the management of similar patients.
Conclusions
We present endoscopic images of possible small intestinal lesions in iTAM, demonstrating multiple erosions and shallow ulcers in the jejunum and ileum. To the best of our knowledge, this report is the first to present endoscopic images of small intestinal lesions associated with iTAM. Intestinal diseases that occur in patients post-hematopoietic stem cell transplantation include iTAM, GVHD, and cytomegalovirus infection. Given the distinct treatment approaches required for these conditions, precise diagnostic and therapeutic interventions are crucial for the effective management of patients following hematopoietic stem cell transplantation. Video capsule enteroscopy may help detect small intestinal involvement in post-hematopoietic stem cell transplant recipients with iTAM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thrombotic microangiopathy after hematopoietic stem cell and solid organ transplantation: a review for intensive care physicians J Intensive Care Med Nusrat S Davis H Mac Dougall K George JN Nakamura R Borogovac A 4064193920243799051610.1177/08850666231200193 · doi ↗ · pubmed ↗
- 2Transplant-associated thrombotic microangiopathy and immune haematological complications following intestine-containing organ transplantation: experience from over 100 consecutive cases Br J Haematol Thomas W Foukaneli T Cosgrove J 96197019320213395498910.1111/bjh.17430 · doi ↗ · pubmed ↗
- 3Intestinal thrombotic microangiopathy: a distinct entity in the spectrum of graft-versus-host disease Int J Hematol Gavriilaki E Sakellari I Karafoulidou I 52953211020193158630410.1007/s 12185-019-02750-7 · doi ↗ · pubmed ↗
- 4A complete histologic approach to gastrointestinal biopsy from hematopoietic stem cell transplant patients with evidence of transplant-associated gastrointestinal thrombotic microangiopathy Arch Pathol Lab Med Warren M Jodele S Dandoy C Myers KC Wallace G Nelson A El-Bietar J 1558156614120172879584010.5858/arpa.2016-0599-RA · doi ↗ · pubmed ↗
- 5Harmonizing definitions for diagnostic criteria and prognostic assessment of transplantation-associated thrombotic microangiopathy: a report on behalf of the European Society for Blood and Marrow Transplantation, American Society for Transplantation and Cellular Therapy, Asia-Pacific Blood and Marrow Transplantation Group, and Center for International Blood and Marrow Transplant Research Transplant Cell Ther Schoettler ML Carreras E Cho B 1511632920233644277010.1016/j.jtct.2022.11.015PMC 10119629 · doi ↗ · pubmed ↗
- 6Cell Therapy Transplant Canada (CTTC) consensus-based Guideline 2024 for management and treatment of chronic graft-versus-host disease and future directions for development Curr Oncol Kim DD Popradi G Lepic K 142614443120243853494110.3390/curroncol 31030108 PMC 10968999 · doi ↗ · pubmed ↗
- 7Guideline development for prevention of transfusion-associated graft-versus-host disease: reduction of indications for irradiated blood components after prestorage leukodepletion of blood components Br J Haematol Wiersum-Osselton JC Slomp J Frederik Falkenburg JH Geltink T van Duijnhoven HL Netelenbos T Schipperus MR 68168819520213449061910.1111/bjh.17822 · doi ↗ · pubmed ↗
- 8Guidelines for the prevention and management of graft-versus-host disease after cord blood transplantation Transplant Cell Ther Ponce DM Politikos I Alousi A 5405442720213421050010.1016/j.jtct.2021.03.012 · doi ↗ · pubmed ↗