First report of an acute case of chagas disease in the municipality of Miraflores, Guaviare, Colombia
José Ziadé Benítez, Diana Cedeño Díaz, Luz Alba Colorado, Laureano Mosquera Murillo, María Trinidad Orozco, Sandra Vallecilla, Julio Cesar Padilla, Mario J. Olivera, José Ziadé Benítez, Diana Cedeño Díaz, Luz Alba Colorado, Laureano Mosquera Murillo, María Trinidad Orozco

TL;DR
This paper reports the first case of acute Chagas disease in a 40-year-old man from Miraflores, Colombia, and outlines the diagnostic and public health responses.
Contribution
This is the first documented case of acute Chagas disease in the municipality of Miraflores, Guaviare, Colombia.
Findings
A 40-year-old man was diagnosed with acute Chagas disease after presenting with fever, headache, and other symptoms.
Five additional cases with similar symptoms were identified, but parasitological tests were negative.
Health education and community surveillance measures were implemented to prevent disease spread.
Abstract
We present a case of acute phase Chagas disease in a 40-year-old male patient from Vereda Buenos Aires, Municipality of Miraflores, Department of Guaviare. The patient attended the emergency department with fever, headache, asthenia, adynamia and dysuria. The blood smear and urinalysis were positive for symptomatic urinary tract infection, but negative for malaria. Five days later the diagnosis of acute phase Chagas disease was confirmed after a positive result for Trypanosoma cruzi. The patient was treated with nifurtimox and benznidazole, his contacts and risk areas were investigated, an active entomological community and institutional search was carried out, as well as in the reservoirs, finally, laboratory surveillance for possible cases of infection in the community was conducted. Five cases with similar symptoms were identified, but parasitological tests were negative. Health…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
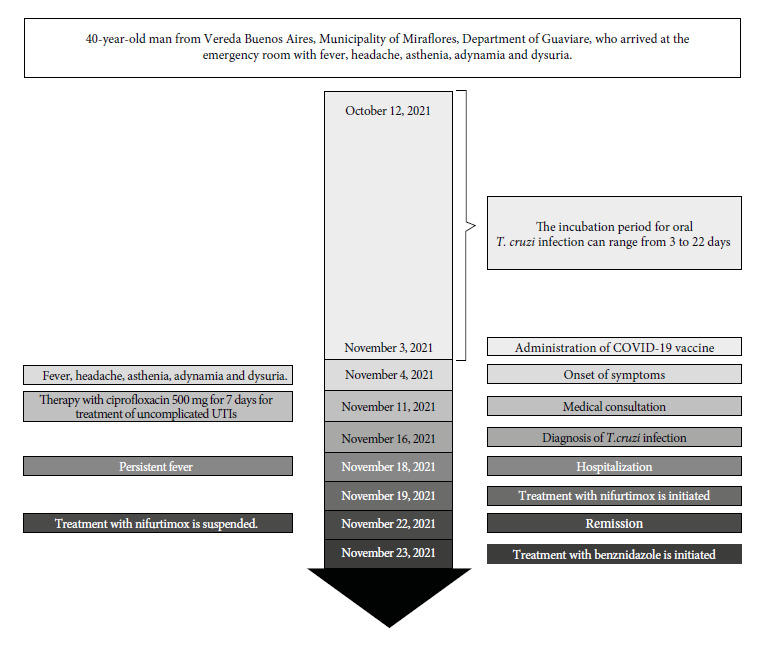 Figure 1
Figure 1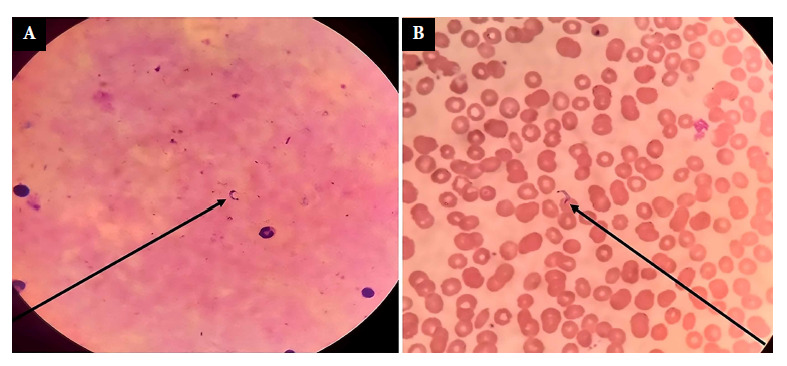 Figure 2
Figure 2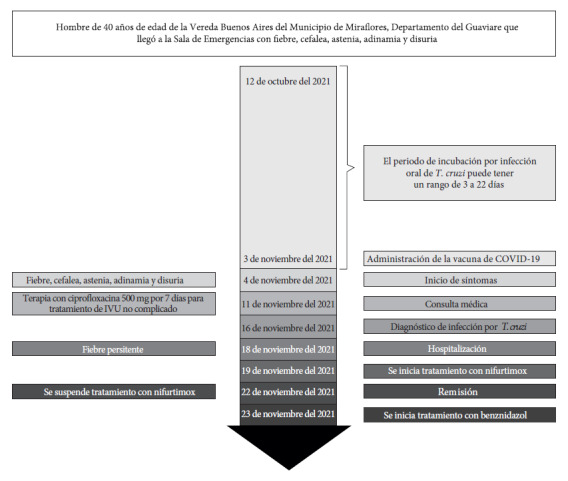 Figure 3
Figure 3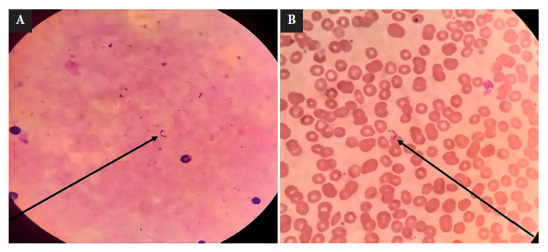 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrypanosoma species research and implications · Research on Leishmaniasis Studies
INTRODUCTION
Chagas disease, caused by the parasite Trypanosoma cruzi, is transmitted mainly by the infected feces of hematophagous triatomine bugs, but can also be transmitted in a variety of ways, including blood transfusions, organ and tissue transplants, mother-to-child transmission, laboratory accidents, and oral ingestion 1^,^2. The incubation period varies according to the mode of transmission: 3 to 22 days for oral transmission, 4 to 15 days for vector-borne transmission, and 8 to 160 days for transfusions and transplants 3. The disease has an acute and chronic phase. Most patients are asymptomatic or experience nonspecific febrile symptoms in the acute phase ^(^4. The chronic phase is divided into two forms: indeterminate (latent) and determinate (clinical), which include cardiac, digestive and cardiodigestive manifestations 5.
The estimated global prevalence of infection is 6 to 8 million people, mainly in Latin America 6. Several departments in Colombia, including Santander, Cundinamarca, Boyacá, Casanare, Arauca and the Sierra Nevada de Santa Marta, have reported high prevalence rates 7. However, in the Department of Guaviare, although the T. cruzi antibody seroprevalence is 2.1%, most cases are imported from endemic areas, which suggests low circulation of the disease in the department. Therefore, the recent documentation of an acute case of Chagas disease in Guaviare is of great interest, as it represents the first evidence of autochthonous transmission in the region. This report serves as initial documentation of such a case in the department, highlighting the novelty and importance of this finding.
CASE REPORT
This is the case of a 40-year-old male patient from Vereda Buenos Aires, Municipality of Miraflores, Department of Guaviare, who attended the emergency department of the Albert Schweitzer Hospital in Miraflores, level I, on November 11, 2021, with 7 days of unquantified fever, accompanied by headache, asthenia, adynamia, and dysuria (Figure 1). He had no photophobia, gastrointestinal or respiratory symptoms, and denied contact with persons positive for coronavirus disease (COVID-19). A thick blood smear test for malaria and a urinalysis were requested, the latter being positive for symptomatic urinary tract infection, which was later confirmed. Outpatient management began with ciprofloxacin 500 mg every 12 hours for 7 days and ibuprofen 400 mg every 8 hours for 5 days. After three days of treatment, the patient showed significant improvement of urinary symptoms. However, it is important to emphasize that the patient’s fever and general symptoms persisted. Five days later (November 16, 2021), a report was received indicating that the thick blood smear test was negative for malaria but positive for Trypanosoma cruzi, confirming the acute phase diagnosis of Chagas disease (Figure 2). Due to difficulties of access to the patient’s place of residence, he was informed and advised to go promptly to the nearest medical center (Albert Schweitzer Hospital in Miraflores, level I). The patient attended medical consultation on November 18, 2021 and was referred to Hospital San José del Guaviare, level II, for complementary tests and specialized management. The presence of parasites was confirmed again in the direct parasitological examination. The anti-T. cruzi IgG ELISA test using total extract antigens was positive. In addition, increased transaminases (aspartate transaminase 161.2 U/L; alanine transaminase 50.9 U/L) and increased C-reactive protein (24 mg/dL) were found. To date, the patient had had only occasional low-grade fevers with no other relevant symptoms or findings on physical examination (Table 1).
Figure 1. Complete timeline of acute Chagas disease, from incubation to hospitalization and initiation of treatment
Figure 2.(A).T**cruzi trypomastigotes in a thick blood smear from the patient, stained with Field’s stain at 100X. (B). T. cruzi trypomastigotes in a peripheral blood smear from the index case, stained with Wright at 100X.
Table 1. Clinical features and laboratory findings in the follow-up of a case of acute Chagas disease, Colombia 2021.Characteristics/date (dd/mm/yy)18/11/2119/11/2120/11/2121/11/2122/11/2123/11/2124/11/2125/11/2126/11/2127/11/2128/11/2130/11/2104/12/2105/12/21WBC (mm^3^)6900---13800----8000--1080011200LYM (%)21---31.2----65.5--47.644.8NEU (%)52---60.3----25.5--40.842.5EOS (%)3---0.2----1.2--3.34.9HGB (gm/dL)12.3---12.4----11.3--12.512.8PLA (/mm^3^)245000---366000----309000--221000247000C-reactive protein (mg/dL)24-------------Direct bilirubin (mg/dL)0.620.12--0.17----0.13--0.12-Total bilirubin (mg/dL)0.680.37--0.71----0.59--0.61-Glycemia (mg/dL)138---105---------ALT (IU/L)161125--72----12715611755-PT Seg12.412.4--11.9----11.4----PTT Seg32.332.3--29.4----36.8----AST (IU/L)50.948--107----1111074928-BUN (mg/dL)----12.2----12.3--11.310.5Creatinine (mg/dL)----0.71----0.92--0.850.8Troponin (ng/mL)Negative-------------Thick smear testT. cruzi trypomastigotes-------------AKP (IU/L)--139-98----77----Albumin (g/dL)--3.2-3.9----3.6----Potassium (mmol/L)-3.8-----------4.5Sodio (mEq/L)-137--135--------137CXR----Normal---------ECGNormal---Normal---------ECO----LVEF 61%, Normal---------EGD----Antral gastritis---------Abdominal Ultrasound-----Normal--------Vital signs
BT37.536.636.536.136.936.236.537.136.737.336.837.436.636.2HR8081788083727976857681787872RR1818192020181718191721192219BP120/70116/68112/71118/73124/72112/68126/76116/74122/70114/62128/74120/68126/72118/64WBC: white blood cell count; LYM: lymphocytes; NEU: neutrophils; EOS: eosinophils; HGB: hemoglobin; PLA: platelets; ALT: alanine aminotransferase; PT: prothrombin time; PTT: partial thromboplastin time; AST: aspartate transaminase; BUN: blood urea nitrogen; AKP: alkaline phosphatase; CXR: chest X-ray; ECG: electrocardiography; ECHO: echocardiography; EGD: esophagogastroduodenoscopy; BT: body temperature in degrees Celsius (°C); HR: heart rate (beats per minute); RR: respiratory rate (breaths per minute); BP: blood pressure (mmHg); BMI: body mass index.
The patient started etiologic treatment with nifurtimox 120 mg (weight: 58 kg), the prescribed dose was 8 mg/kg/day, administered as one tablet every 8 hours. The treatment started on November 19, 2021. However, due to the likelihood of complications during the course of the disease and being the first clinical case reported in Guaviare, the responsible medical team decided to refer the patient to a more complex healthcare level. Thus, the patient was transferred to San Carlos level III Hospital, in the city of Bogota, on November 22, 2021, for evaluation and specialized management. At the time of admission, the patient still had fever and was on his fourth day of treatment with nifurtimox. Laboratory tests showed mild leukocytosis with neutrophilia, as well as elevated transaminases and circulating parasitemia (Table 1). No tests were performed to rule out the possibility of other diseases associated with a compromised immune system. In addition, the patient did not disclose any previous medical conditions or diseases. The responsible medical team decided to change the treatment to benznidazole 100 mg every 12 hours for 60 days because the dose of the previous medication was insufficient, and because benznidazole is the treatment of choice according to current clinical practice guidelines.
During hospitalization, the patient did not present hemodynamic alterations or changes, and tolerated the antitrypanosome treatment adequately without any adverse events. The cardiological tests were within normal limits. Finally, the patient was discharged in good health and continued supervised outpatient treatment at the Albert Schweitzer Hospital near his home. Subsequent follow-up showed no evidence of parasitaemia by direct parasitological methods, and anti-T. cruzi IgG serology was negative.
Investigation of contacts and risk areas
The epidemiological field investigation showed that the patient identified as a native and resident of Miraflores, without a partner and with a six-year-old son. The patient frequently moved to two areas and moved infrequently to another: Vereda Mateguadua (zone 1), where he works and resides Monday through Friday; the center of the town of Buenos Aires (zone 2), where he visits his son, his only relative, on Saturdays and Sundays; and the town of Yavilla (zone 3), which he visits every 20 days, but does not stay overnight there. In addition, 16 direct contacts of the patient were identified, 5 in zone 1 and 11 in zone 2.
Active community search
Probable cases of acute Chagas disease were identified during the active community search in zones 1 and 2 using the case definition recommended in the surveillance protocol. A total of 67 social and family contacts were evaluated, 5 of whom presented symptoms and underwent direct parasitological testing, while the other 62 asymptomatic contacts underwent serological testing. Both direct parasitological and serological tests were negative. In addition, malaria antigen and COVID-19 rapid tests were performed, the results of which were also negative. Finally, health education activities were carried out for the community.
Active institutional search
An active institutional retrospective search was conducted at the Miraflores Hospital, in which the medical records of patients attended since October (one month before case presentation) were reviewed to find patients who met the case definition recommended in the surveillance protocol. As a result, 10 probable cases were identified and the serological tests were negative.
Entomological investigation
Entomological surveys and detailed home inspections were carried out in zones 1 and 2 to identify risk areas related to the presence of the vector in bedrooms, mattresses, roofs and common areas. In addition, wild vector traps were installed around the house, but no vectors were found in them. On the other hand, a Rhodnius prolixus specimen was identified in a room of an educational institution located in zone 2; fresh examination was conducted on the specimen without finding intestinal contents.
Reservoir investigation
Tomahawk traps were installed in zones 1 and 2 at strategic locations around houses with favorable biological conditions for the presence of wild animals. However, no reservoirs were captured in these traps. In addition, 10 blood samples were taken from canines, which were negative for T. cruzi.
DISCUSSION
This report is the first clinical description of an autochthonous case of acute Chagas disease in the department of Guaviare. The case suggests possible oral transmission in an adult male who was incidentally detected and had an unusual clinical presentation. The patient received an accurate diagnosis and appropriate treatment, underscoring the importance of prompt and effective management of Chagas disease.
Possible oral transmission of T. cruzi should be suspected when acute symptoms manifest without bipalpebral edema or the presence of the Romaña sign 8. In addition, the absence of localized indurations, known as inoculation chagomas, commonly associated with vector-borne transmission, further strengthens the hypothesis of contamination through ingestion of infectious metacyclic forms 8.
This case is interesting because the patient lives in a non-endemic area, where other vector-borne diseases are prevalent 9. In addition, his initial diagnosis was incidental, as the first differential diagnosis considered the most common diseases in the region.
The medical team followed the current clinical practice guideline during the patient’s treatment and administered nifurtimox, which is one of the etiologic drugs available 10^-^12. However, at a more complex level of care to which he was referred, the treatment was changed to benznidazole, apparently following the guideline first-line regimen 10^,^11.
In our opinion, the patient was already receiving the appropriate etiologic treatment, albeit underdosed. Therefore, it was only necessary to adjust the dose to four tablets per day without the need to change the drug 13. Although the change in the current clinical practice guideline is justified, other important aspects had to be considered, such as the duration of treatment the patient had already been receiving, that it was the only option available at the screening site and that no adverse effects had occurred 13.
At post-treatment follow-up, both direct parasitological methods and anti-T.cruzi IgG serological testing were used to assess the effectiveness of treatment. Direct parasitological methods revealed no evidence of parasitemia, indicating successful elimination of T. cruzi from the patient’s bloodstream. Similarly, anti-T. cruzi IgG serological testing showed negative results, confirming the absence of antibodies to T. cruzi. This comprehensive evaluation provides strong evidence of parasite eradication, resulting in a positive outcome and suggesting a complete cure of T. cruzi infection 1^,^2^,^14^,^15.
It is important to note that, although not necessary, the patient was hospitalized for several days. Therefore, the recommended criteria for considering outpatient management with close surveillance should be properly applied in future cases 16. This measure can contribute significantly to health care professionals learning from the situation and improving patient-centered care 17.
One lesson learned is that management and prevention of future cases of Chagas disease in Guaviare will require a multifaceted approach. This approach should include surveillance of current cases, educational campaigns to raise awareness of the disease among the local population, and efforts to control vector populations 16. This measure can significantly contribute to health care professionals learning from the situation and improving patient-centered care 17.
In conclusion, our study shows that the population of the Department of Guaviare may be at risk for T. cruzi infection through oral transmission within the region. This highlights the importance for physicians to remain vigilant regarding acute Chagas disease as a possible zoonotic parasitic infection, especially in cases of prolonged febrile syndrome. Improved diagnostic prediction, management, and follow-up protocols are crucial to ensure optimal care for affected individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jr. A Rassi Rassi A Marin-Neto JA Chagas disease Lancet 201037597231388140210.1016/S 0140-6736(10)60061-X 20399979 · doi ↗ · pubmed ↗
- 2de Sousa AS Vermeij D Ramos AN Jr Luquetti AO Chagas disease Lancet 20244031042220321810.1016/S 0140-6736(23)01787-738071985 · doi ↗ · pubmed ↗
- 3Coura JR The main sceneries of Chagas disease transmission The vectors, blood and oral transmissions-A comprehensive review Mem Inst Oswaldo Cruz 2015110327728210.1590/0074-027614036225466622 PMC 4489464 · doi ↗ · pubmed ↗
- 4Vega S Cabrera R Álvarez CA Uribe-Vilca I Guerrero-Quincho S Ancca-Juárez J Clinical and epidemiological characteristics of cases of acute Chagas disease in the Peruvian Amazon basin, 2009-2016 Rev Peru Med Exp Salud Publica 2021381707610.17843/rpmesp.2021.381.628634190928 · doi ↗ · pubmed ↗
- 5Olivera MJ Muñoz L Exploring the latency period in Chagas disease duration and determinants in a cohort from Colombia Trans R Soc Trop Med Hyg 2024 trae 004trae 00410.1093/trstmh/trae 00438411919 · doi ↗ · pubmed ↗
- 6World Helalth Organization Chagas disease in Latin America an epidemiological update based on 2010 estimates Wkly Epidemiol Rec 2015906334325671846 · pubmed ↗
- 7Olivera MJ Fory JA Porras JF Buitrago G Prevalence of Chagas disease in Colombia: A systematic review and meta-analysis P Lo S One 201914110.1371/journal.pone.0210156 PMC 632274830615644 · doi ↗ · pubmed ↗
- 8Instituto Nacional de Salud Protocolo de vigilancia de Chagas 2018 Bogota D Chttps://www.ins.gov.co/buscador-eventos/Lineamientos/Pro_Chagas%202022.pdf