The Use of Steroids to Treat Hypercalcemia Due to Granulomatous Disease From Disseminated Coccidioidomycosis
Tim Yu, Stephen Bruce, Diep Nguyen, Anika Patel, Mark MacElwee

TL;DR
This paper presents a case where steroids helped treat high blood calcium caused by a fungal infection called coccidioidomycosis.
Contribution
The paper contributes a novel case study on treating hypercalcemia in disseminated coccidioidomycosis using a combination of therapies including steroids.
Findings
Hypercalcemia in disseminated coccidioidomycosis can be effectively treated with calcitonin, bisphosphonates, and corticosteroids.
The patient showed a favorable outcome following combinatorial treatment despite controlled infection.
Abstract
The clinical course and treatment of hypercalcemia from a granulomatous disease in the setting of an infectious etiology, namely disseminated coccidioidomycosis, remains incompletely understood. The mechanism and treatment of hypercalcemia have been documented in most granulomatous disorders, with sarcoidosis being the most well-understood so far. We discuss a case of a patient with a recent diagnosis of disseminated coccidioidomycosis who presented with hypercalcemia despite adequate infection control. The treatment course involved combinatorial-calcitonin, low-dose bisphosphonates, and corticosteroids, which led to a favorable outcome.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
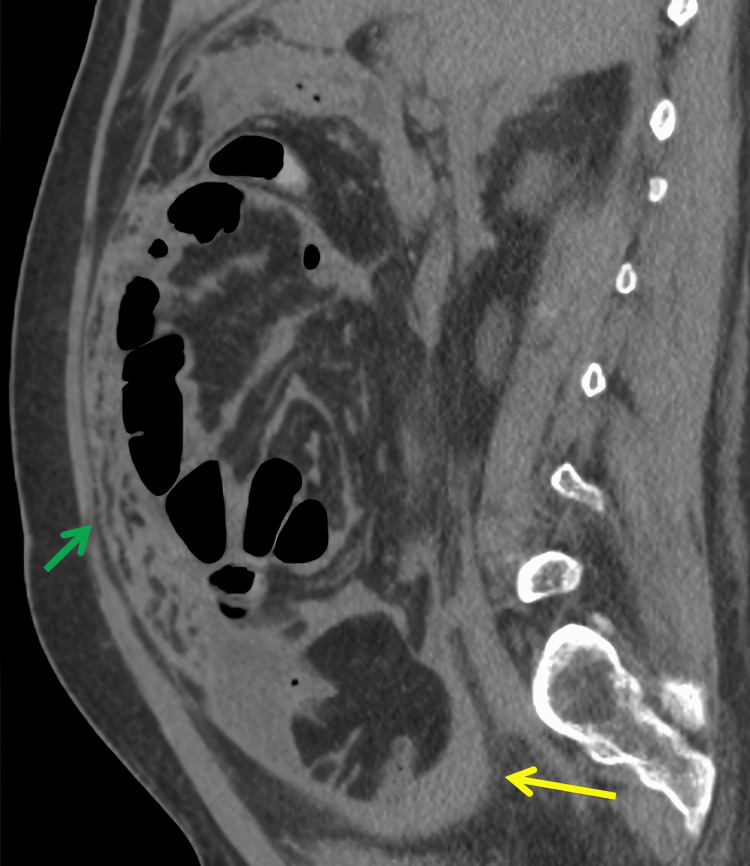 Figure 1
Figure 1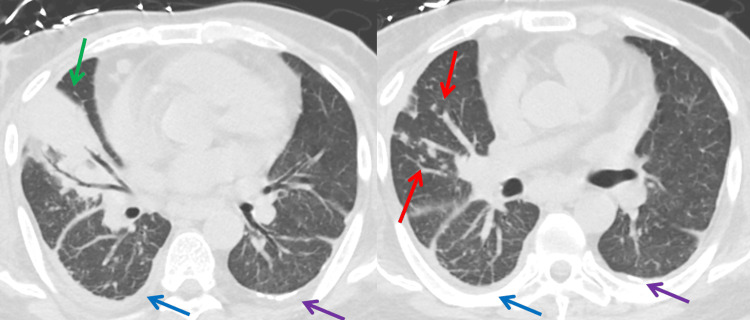 Figure 2
Figure 2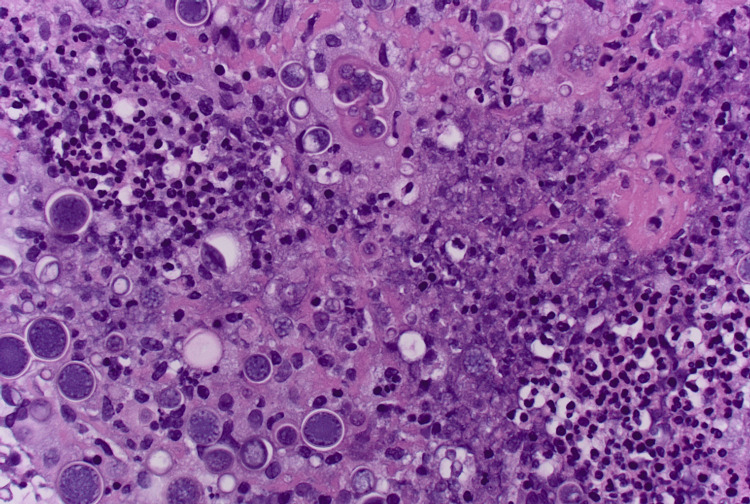 Figure 3
Figure 3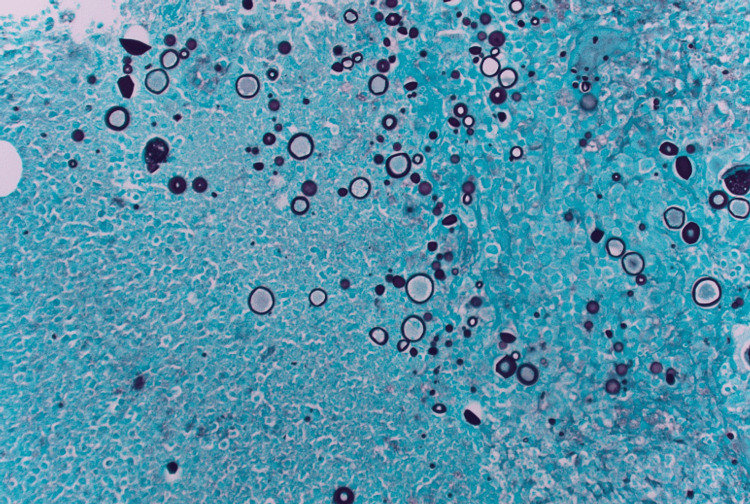 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Fungal Infections and Studies
Introduction
Coccidioidomycosis is a granulomatous fungal infection caused by the genus Coccidioides, which is endemic to the Southwestern United States; the majority of cases have been reported from Arizona (Phoenix and Tucson) and California (San Joaquin Valley). Over the past 30 years, the incidence of coccidioidomycosis in Arizona has increased considerably from 5.2 cases per 100,000 in 1990 to 160.6 cases per 100,000 in 2020 [1]. Coccidioides primarily grows in soil and infection occurs from the airborne inhalation of singular cells called arthroconidia [2]. While most patients remain asymptomatic after exposure, the clinical symptoms can range from pneumonia-like illness to extrapulmonary disseminated infection. The main risk factor for disseminated infection is cellular immunity suppression, and its extrapulmonary manifestations include meningitis, osteomyelitis, subcutaneous abscesses, and rarely, peritoneal involvement through lymphatic spread [3]. In rare cases, hypercalcemia may manifest in the setting of coccidioidomycosis. While hypercalcemia is a common finding in other granulomatous disorders like sarcoidosis [4] and tuberculosis [5], the mechanism of action and management for hypercalcemia in the setting of coccidioidomycosis is poorly understood. We present a patient with a rare case of hypercalcemia with low parathyroid hormone levels (PTH) and elevated parathyroid hormone-related peptide levels (PTHrP) in the setting of granulomatous coccidioidomycosis. We aim to discuss the clinical course and diagnostic challenges and highlight the use of steroids as a viable alternative to treat hypercalcemia in disseminated coccidioidomycosis.
Case presentation
A 41-year-old male with no significant past medical history presented to the hospital with three days of abdominal pain and a non-healing right calcaneal ulcer. MRI of the right ankle revealed acute osteomyelitis of the posterior calcaneus positive for methicillin-sensitive Staphylococcus aureus and Coccidioides. CT of the abdomen (Figures 1, 2) and subsequent omental biopsy (Figures 3, 4) at the time revealed granulomatous inflammation and coccidioidal peritonitis without malignancy, leading to a diagnosis of disseminated coccidioidomycosis.
Sagittal non-contrast CT of the abdomen and pelvisThe image shows scattered thickened mesenteric and omental nodularity (green arrow). In addition, there is a small amount of walled-off fluid in the pelvis (yellow arrow). The constellation of findings is concerning for peritonitis versus peritoneal carcinomatosisCT: computed tomography
Axial non-contrast CT of the abdomen and pelvisThe images show the middle (right panel) and lower (left panel) lung lobes. Right middle lobe consolidation (green arrows) with scattered centrilobular nodules throughout the right lung base(red arrows), trace right pleural effusion (blue arrows), and left pleural calcifications (purple arrows) can be seenCT: computed tomography
H & E stain of omental biopsyH & E stain showing thick-walled spherules with multiple endospores, suggesting coccidioidomycosis
GMS stain of omental biopsyGMS-positive stain showing Coccidioides immitis spherules
Labs were obtained to further rule out malignancy and common causes of immunodeficiency. Serum IgG1 levels were elevated and IgA and complement levels were normal. CD4 count was 304 cells/μl (normal: 328-1404 cells/μl) and CD3 and CD8 counts were within normal limits. HIV serology was negative. Carcinoembryonic antigen, alpha fetal protein, and carbohydrate antigen 19-9 were all within normal limits. MRI of the brain showed no acute intracranial abnormality. The patient completed a six-week inpatient course of amphotericin B and was started on lifelong fluconazole therapy. While on amphotericin B, the patient developed acute tubular necrosis and was ultimately diagnosed with end-stage renal disease requiring hemodialysis. He showed improvement in his symptoms after the initiation of antifungals and was subsequently discharged after treatment completion. A repeat CT at the time of discharge showed improved pulmonary coccidioidomycosis with no new lesions.
One month after discharge, the patient returned to the hospital with abdominal pain and headaches after the dialysis center noted a calcium level of 15.9 mg/dL (normal: 8.4-10.2 mg/dL). The physical exam was positive for abdominal tenderness without distension or palpable masses. No focal neurological deficits were noted. At this admission, laboratory results revealed a white blood cell count of 7.2 K/uL (90.8% neutrophils, 3.4% lymphocytes, 3.9% monocytes, 0.5% eosinophils, and 0.2% basophils), hemoglobin of 9.5 g/dL, platelets of 263 K/uL, creatinine of 1.89 mg/dL (normal: 0.66-1.25 mg/dL), albumin of 2.7 g/dL (normal: 3.5-5 g/dL), phosphorus of 6 mg/dL (normal: 2.5-4.5 mg/dL), magnesium of 1.8 mg/dL (normal: 1.6-2.3 mg/dL), alkaline phosphatase of 62, PTH of 5.9 pg/mL (normal: 7.5-53.5 pg/mL), and low 25-OH-Vitamin D of 23.6 ng/mL (normal: 30-80 ng/mL).
The patient was started on 250 units of calcitonin twice per day and one dose of intravenous pamidronate 30 mg the following day with minimal improvement to his symptoms. Subsequent lab results showed 1,25-OH-Vitamin D of 175 pg/mL (normal: 19.9-79.3 pg/mL) and PTHrP of 3.9 pmol/L (normal: 0-2.3 pmol/L). Chest X-ray showed a small right pleural effusion with right middle lobe opacity. Tuberculosis had been ruled out based on negative acid-fast bacilli (AFB) cultures during the initial admission three months prior. Given the recent diagnosis of widely disseminated coccidioidomycosis, PTH suppression, elevated PTHrP, and markedly elevated active Vitamin D levels, he was diagnosed with hypercalcemia due to granulomatous disease from disseminated coccidioidomycosis. At this time, we decided to discontinue bisphosphonate therapy as he had not been responding to treatment, instead initiating a 10-day course of prednisone 60 mg/day, tapering 10 mg/day until 20 mg/day was reached. On this regimen, his symptoms resolved with the normalization of calcium levels. While malignancy is a reasonable differential due to elevated PTHrP, the lack of significant cancer biomarkers, histological samples, imaging findings, and the resolution of hypercalcemia following prednisone therapy make this less likely.
Discussion
Disseminated coccidioidomycosis stands out as a rare and intriguing contributor to hypercalcemia, as its underlying mechanism and optimal treatment method remain elusive. Notably, our case aligns with the current literature that hypercalcemia associated with coccidioidomycosis is observed only in the disseminated form. A study involving 13 patients by Caldwell et al. found no correlation between elevated 1,25-dihydroxyvitamin D and hypercalcemia due to coccidioidomycosis, which contrasts with our case and known mechanisms such as those in sarcoidosis [6]. Another study by Fierer et al. suggested that granuloma PTHrP overexpression may contribute to hypercalcemia in disseminated coccidioidomycosis, consistent with our patient's case [7]. Nonetheless, larger and more extensive studies are needed to fully elucidate the mechanism behind hypercalcemia in disseminated coccidioidomycosis.
The management of hypercalcemia in granulomatous diseases, notably studied in sarcoidosis, usually involves moderate-dose steroid therapy [8]. In refractory conditions or steroid intolerance, bisphosphonates, chloroquine, and anti-TNF alpha therapy have shown efficacy [8-10]. Granulomatous hypercalcemia caused by infections typically resolves with successful infection treatment. Data are scarce on the treatment of patients who suffer from this condition despite adequate infection control, such as our patient, who had already undergone a six-week course of amphotericin B and was on lifelong fluconazole when hypercalcemia manifested. Bisphosphonate therapy has been shown to successfully resolve granulomatous hypercalcemia due to disseminated coccidioidomycosis [7,11]. The most commonly prescribed bisphosphonate therapy is pamidronate 60 mg. To our knowledge, there is only one case report documenting the favorable use of steroids, which involved administering one dose of hydrocortisone 10 mg followed by 5 mg [12].
Traditionally, glucocorticoids have been avoided in treating granulomatous diseases from infectious origins due to concerns about immune suppression [13]. Further studies are necessary to assess the potential risk of corticosteroids inducing exacerbations of disseminated coccidioidomycosis on adequate prophylaxis. In our case, glucocorticoids proved effective in resolving hypercalcemia associated with disseminated coccidioidomycosis without subsequent acute exacerbations of the disseminated infection. While a higher and more prolonged dose of bisphosphonate therapy might have proven effective, glucocorticoids should be considered as an effective alternative in treating patients with hypercalcemia due to granulomatous disseminated coccidioidomycosis.
Conclusions
Disseminated coccidioidomycosis is a relatively rare cause of hypercalcemia, and more serious causes such as malignancy must be ruled out in these patients. A diagnosis was made in our patient based on a combination of histological, radiological, clinical, and laboratory findings. Given the limited evidence on treating granulomatous hypercalcemia in disseminated coccidioidomycosis, we aim to underscore the effective use of steroids in this context, offering providers an alternative treatment option.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1California Department of Public Health: valley fever 6 2024 2022 https://www.azdhs.gov/preparedness/epidemiology-disease-control/index.php#data-stats-past-years
- 2Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis J Clin Microbiol Saubolle MA Mc Kellar PP Sussland D 26304520061710806710.1128/JCM.02230-06PMC 1828958 · doi ↗ · pubmed ↗
- 3The spectrum and presentation of disseminated coccidioidomycosis Am J Med Adam RD Elliott SP Taljanovic MS 77077712220091963527810.1016/j.amjmed.2008.12.024 · doi ↗ · pubmed ↗
- 4Vitamin D, calcium, and sarcoidosis Chest Sharma OP 5355391091996862073210.1378/chest.109.2.535 · doi ↗ · pubmed ↗
- 5Hypercalcemia in active pulmonary tuberculosis Ann Intern Med Abbasi AA Chemplavil JK Farah S Muller BF Arnstein AR 32432890197942640010.7326/0003-4819-90-3-324 · doi ↗ · pubmed ↗
- 6Hypercalcemia in patients with disseminated coccidioidomycosis Am J Med Sci Caldwell JW Arsura EL Kilgore WB Reddy CM Johnson RH 151832720041472239110.1097/00000441-200401000-00004 · doi ↗ · pubmed ↗
- 7Hypercalcemia in disseminated coccidioidomycosis: expression of parathyroid hormone-related peptide is characteristic of granulomatous inflammation Clin Infect Dis Fierer J Burton DW Haghighi P Deftos LJ 0655201210.1093/cid/cis 53622670039 · doi ↗ · pubmed ↗
- 8Diagnosis and treatment of pulmonary sarcoidosis: a review JAMA Belperio JA Shaikh F Abtin FG Fishbein MC Weigt SS Saggar R Lynch JP 3rd 85686732720223523038910.1001/jama.2022.1570 · doi ↗ · pubmed ↗