Improving Transition of Care for Pediatric Patients With Chronic Kidney Disease: A Pilot Project
Melvin Chan, Sarah Young, Melisha Hanna

TL;DR
This pilot project shows that younger age and being male are linked to poor transition readiness for pediatric CKD patients, and a remote curriculum can help improve their preparedness for adult care.
Contribution
A structured, remote curriculum was developed and shown to improve transition readiness in pediatric CKD patients.
Findings
Younger age and male gender were identified as risk factors for poor transition readiness.
The remote curriculum improved TRAQ scores by about 25% across all domains in six months.
Follow-up frequency (three vs. six months) did not significantly affect outcomes.
Abstract
Introduction Transition is the process of preparing an adolescent or young adult for the adult model of care. Poor transitions have been linked to increased medical utilization and poorer kidney outcomes. There are limited studies evaluating predictors of transition readiness or interventions in pediatric patients with chronic kidney disease (CKD). Methods We enrolled 42 non-dialysis, non-transplant patients with CKD stage 2 or higher and 14 years and older receiving care in our pediatric nephrology clinic. Data collected included demographics, clinical information, and transition readiness as measured by the Transition Readiness Assessment Questionnaire (TRAQ). Patients were provided with a structured, remote curriculum with resources that addressed areas of need. Patients were followed every three to six months. Repeat TRAQ questionnaires were administered six months after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
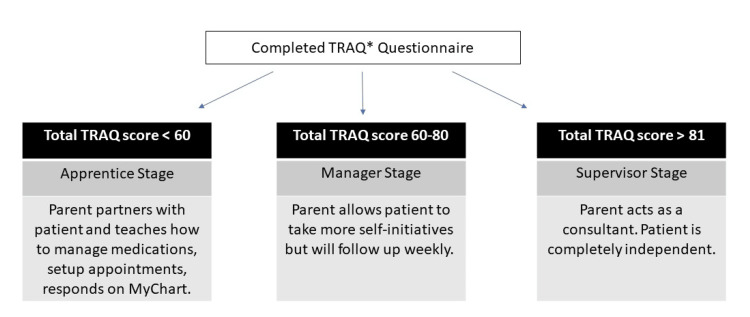 Figure 1
Figure 1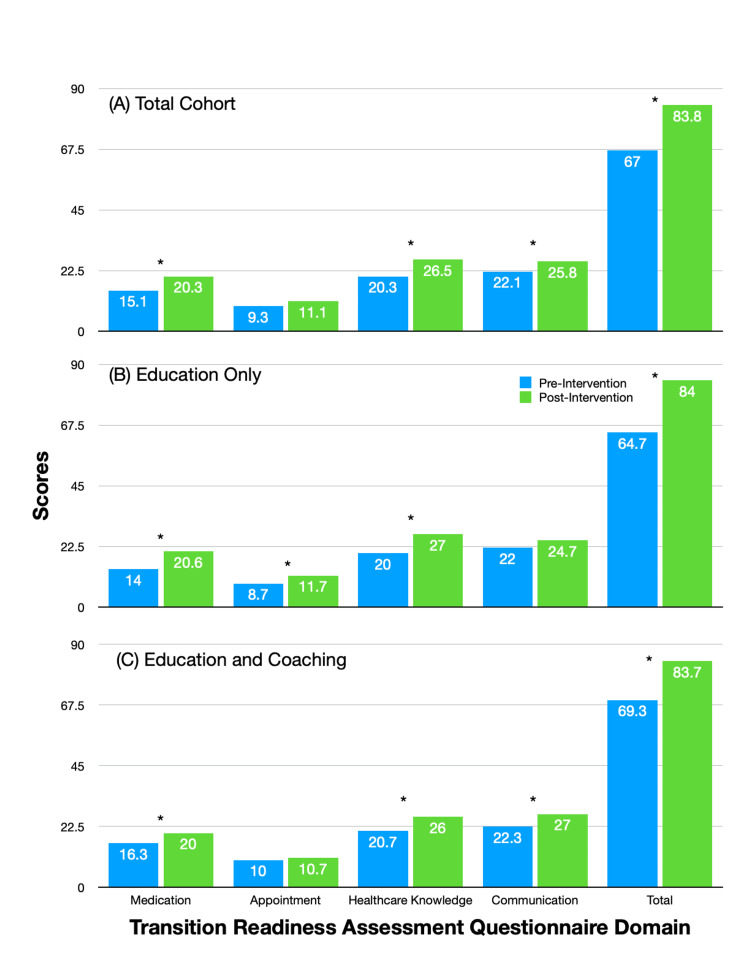 Figure 2
Figure 2| Variables | Eligible patients (n = 151) | Full enrolled cohort based on follow-up survey status (n = 42) | ||||
| Median (IQR)/count (%) | Unenrolled cohort (n = 109) | Enrolled cohort (n = 42) | p-value | No follow-up survey (n = 28) | Had follow-up survey (n = 14) | p-value |
| Age (years) | 16 (15-18) | 16 (15-17) | 0.227 | 16 (15-17) | 16 (15-17) | 0.65 |
| Gender | - | 0.601 | - | 0.166 | ||
| Male | 67 (62%) | 24 (57%) | - | 18 (64%) | 8 (57%) | - |
| Female | 42 (38%) | 18 (43%) | 10 (36%) | 6 (43%) | ||
| Race | - | 0.971 | - | 0.836 | ||
| Caucasian | 57 (53%) | 22 (52%) | - | 15 (54%) | 7 (50%) | - |
| Non-Caucasian | 52 (47%) | 20 (48%) | 13 (46%) | 7 (50%) | ||
| Insurance | - | 0.628 | - | 0.199 | ||
| Private insurance | 57 (53%) | 24 (57%) | - | 15 (54%) | 6 (43%) | - |
| Public insurance/no insurance | 52 (47%) | 18 (43%) | 13 (46%) | 8 (57%) | ||
| Kidney disease severity | - | 0.553 | - | 0.667 | ||
| Mild | 72 (66%) | 30 (71%) | - | 20 (71%) | 11 (79%) | - |
| Moderate/severe | 27 (34%) | 12 (29%) | 8 (29%) | 3 (21%) | ||
| Number of specialty clinics | NA | 4 (3-9.5) | - | 4 (2-9) | 6.5 (3-11) | 0.212 |
| TRAQ initial scores | - | |||||
| Medications | NA | 13.5 | - | 12.5 | 15.5 | 0.28 |
| Appointment | NA | 7.5 | 7 | 8.5 | 0.873 | |
| Healthcare knowledge | NA | 19 | 17.5 | 20.5 | 0.583 | |
| Provider communication | NA | 22 | 22 | 21.5 | 0.859 | |
| Total | NA | 59.5 | 55 | 63.5 | 0.34 | |
| TRAQ section/variables | Bivariate analysis | Multivariable analysis | ||
| β* | p-value | β* | p-value | |
| TRAQ: Medications | - | |||
| Age (years) | 1.24 | 0.039** | - | |
| Male gender | -1.44 | 0.464 | ||
| Non-Caucasian | 0.62 | 0.751 | ||
| Private insurance | 1.17 | 0.546 | ||
| Number of emergency room visits | -0.52 | 0.336 | ||
| Number of hospitalizations | -0.2 | 0.845 | ||
| Average length of stay | -0.29 | 0.38 | ||
| Number of subspecialty clinic appointments | -0.14 | 0.371 | ||
| Moderate/severe CKD | -0.04 | 0.987 | ||
| TRAQ: Appointments | - | |||
| Age (years) | 1.16 | 0.010** | 1.05 | 0.025** |
| Male gender | -2.13 | 0.043** | -1.12 | 0.167 |
| Non-Caucasian | 0.47 | 0.752 | - | |
| Private insurance | -0.87 | 0.56 | ||
| Number of emergency room visits | -0.71 | 0.083 | ||
| Number of hospitalizations | -0.43 | 0.578 | ||
| Average length of stay | -0.18 | 0.485 | ||
| Number of subspecialty clinic appointments | -0.21 | 0.081 | ||
| Moderate/severe CKD | -1.78 | 0.297 | ||
| TRAQ: Healthcare knowledge | - | |||
| Age (years) | 0.16 | 0.92 | - | |
| Male gender | -7.65 | 0.131 | ||
| Non-Caucasian | 6.46 | 0.198 | ||
| Private insurance | -4.8 | 0.342 | ||
| Number of emergency room visits | -0.51 | 0.718 | ||
| Number of hospitalizations | -1.18 | 0.655 | ||
| Average length of stay | -0.42 | 0.628 | ||
| Number of subspecialty clinic appointments | -0.33 | 0.436 | ||
| Moderate/severe CKD | -2.56 | 0.662 | ||
| TRAQ: Provider communication | - | |||
| Age (years) | 0.07 | 0.965 | - | |
| Male gender | -8.65 | 0.042** | ||
| Non-Caucasian | 4.82 | 0.336 | ||
| Private insurance | -2.99 | 0.553 | ||
| Number of emergency room visits | -0.13 | 0.929 | ||
| Number of hospitalizations | -0.4 | 0.879 | ||
| Average length of stay | -0.2 | 0.814 | ||
| Number of subspecialty clinic appointments | -0.23 | 0.578 | ||
| Moderate/severe CKD | -1.78 | 0.76 | ||
| TRAQ: Total score | - | |||
| Age (years) | 7.03 | 0.002** | - | |
| Male gender | -6.93 | 0.374 | ||
| Non-Caucasian | -0.51 | 0.948 | ||
| Private insurance | 3.07 | 0.692 | ||
| Number of emergency room visits | -1.92 | 0.372 | ||
| Number of hospitalizations | 1.01 | 0.802 | ||
| Average length of stay | -0.36 | 0.782 | ||
| Number of subspecialty clinic appointments | -0.33 | 0.606 | ||
| Moderate/severe CKD | -4.59 | 0.607 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent and Pediatric Healthcare · Childhood Cancer Survivors' Quality of Life · Bipolar Disorder and Treatment
Introduction
Medical treatment improvements have resulted in as much as 90% of children with chronic illnesses surviving into adulthood, all of whom will need an adult provider [1]. Poor transition can result in increased medical utilization and a higher risk of graft rejections in kidney transplant recipients [1,2]. A recent report from the National Survey of Children’s Health in 2019 showed that only 23% of children with chronic illness received a formal transition education, which has been shown to improve adherence to care, disease-specific measures, quality of life, satisfaction with care, and healthcare utilization [1,3,4].
Transitioning adolescents and young adults (AYA) with childhood-onset conditions to adult medical care is challenging for multiple reasons. Adolescence is an important period of multiple changes, specifically as it relates to identity, education, and sexuality [5]. Having a chronic condition, such as sickle cell disease or chronic kidney disease (CKD), can complicate this developmental period [5]. Studies among AYA with chronic health conditions have shown lower self-esteem and higher rates of depressive symptoms and suicidal thoughts [6,7]. Therefore, a multidisciplinary team is required to help AYA through this developmental period.
From a provider perspective, there are logistical and financial barriers. At our institution, patients come from seven states, making it difficult to coordinate fragmented care. Additionally, limited clinic time is focused on medical care rather than educating patients about transition. Dedicated transition clinics are resource-intensive, requiring multidisciplinary personnel, including social workers, navigators, providers, and pharmacists. Lastly, payment systems do not reimburse this complex care coordination; multiple studies have highlighted the importance of navigators for successful transitions [5,8,9].
Because of these challenges, there are no standard best practices for developing a transition program [5]. Previous interventions include transition camps, mentorship programs, and transition coordinators, with most studies finding positive qualitative outcomes, like increased motivation [10]. Of the studies evaluating quantitative outcomes, most come from multidisciplinary transition clinics involving AYA solid organ transplant recipients; these clinics improve follow-up with adult providers, medication adherence, and renal function [11,12]. In our review of the literature, none have evaluated improving transition readiness through a structured curriculum and correlating readiness with outcomes.
The goal of this pilot project is to evaluate the effectiveness of a structured education curriculum for AYA with CKD. This paper will describe predictors of transition readiness, a remote transition curriculum and its impact on transition readiness, and feedback from participants and their families. A follow-up study will evaluate the outcomes, such as medical utilization and clinical parameters, for patients who transfer to an adult provider.
Materials and methods
We conducted a prospective pilot project at Children’s Hospital Colorado in Aurora, a freestanding children’s hospital with over 600 beds across four campuses and a quaternary referral center in the western United States. The study included all follow-up patients aged 14 and older with CKD stage 2 or higher. Exclusion criteria included those with intellectual disabilities, who had a transplant, or who were on dialysis, as these patients had different transition processes. Eligible patients were recruited through the patient portal or by telephone call. At our center, over 90% of patients used MyChart to communicate with their healthcare team (Epic, Verona, United States). Interested patients were sent a message with the Transition Readiness Assessment Questionnaire (TRAQ) and received postcard consent through the patient portal or email. The Colorado Multiple Institutional Review Board approved this study (approval number 21-4622).
Predictors
Patient demographic data was collected from the electronic health record (EHR), including age, gender, and type of insurance. Additionally, the following information on medical utilization in the prior year was gathered: the number of emergency room visits, hospitalizations, average length of stay per hospitalization, and number of specialty appointments attended at our institution. Finally, the patient’s CKD staging was recorded as defined by the Kidney Disease: Improving Global Outcomes [13]. Patients who had stage 1 or 2 CKD were categorized as having mild kidney disease, whereas the other stages were categorized as being moderate to severe.
Transition readiness
The primary outcome was transition readiness, as measured by TRAQ. This questionnaire is a well-validated, 20-item patient-report survey that has four key domains assessing confidence in medication management, appointment keeping, healthcare knowledge, and communication (Appendix A) [14].
All patients completed the survey before enrollment. After enrollment, patients were placed into stages based on their total scores and encouraged to collaborate with their parents, as shown in Figure 1.
Staging based on TRAQ scoreBased on the total TRAQ score, patients were placed in different stages. The “apprentice” stage corresponded to patients scoring less than 60 points and required the most parental support. Scores of 60-80 points corresponded to the “manager” stage needing less supervision. Patients scoring over 80 points were in the “supervisor” stage and were the most independent.TRAQ, Transition Readiness Assessment Questionnaire
If patients scored less than 90% of the total domain score, handouts were sent via the patient portal. Patients struggling with medication knowledge or skills were given a tip sheet (Appendix B). For patients who needed help with healthcare knowledge, they were provided a kidney passport, a handout on CKD basics, and commonly used CKD medications (Appendices C-E). Patients needing help with appointments and communications were encouraged to get access to their own patient portal in addition to their parent’s account.
After these initial interventions, patients were provided two follow-up options: education only (EO) or education and coaching (EC). In the EO cohort, patients had a follow-up every six months, whereas those in the other cohort had one every three months. These follow-up sessions were conducted via the patient portal and a telephone call. During the follow-up, patients were commended for their progress and coached in deficient areas, and key elements of the handouts were reinforced. During these follow-ups, read receipt notifications were used to track adherence to handouts. TRAQ was readministered every six months, regardless of the follow-up option. Failure to complete the follow-up question was characterized as a lost to follow-up.
Feedback
During TRAQ readministration at six months, patients were asked the following: (1) How is the program going?; (2) What are the strengths of this program?; (3) What are the weaknesses of this program?; (4) How can we improve these weaknesses?
Statistical analysis
Patient characteristics were summarized using medians (IQRs) for continuous variables and counts (percentages) for categorical data. Statistical comparisons of patients who did and did not complete their follow-up surveys were performed using the Mann-Whitney U test for continuous variables and the Pearson chi-square test for categorical data. Bivariate associations between predictors and TRAQ scores were analyzed using linear regression. Multivariable linear regression models, based on variables with p < 0.05 in bivariate analysis, were used to account for potential confounding variables. A Wilcoxon signed-rank test was used to compare initial and six-month follow-up TRAQ scores. A repeated measures ANOVA was used to evaluate the effects of the EC and EO cohorts. Analysis was performed using IBM SPSS Statistics for Windows, Version 29.0 (Released 2022; IBM Corp., Armonk, NY, USA).
Results
Out of a total of 151 eligible patients, 42 patients were enrolled in this pilot project, with a participation rate of 27.8%. Table 1 describes the clinical characteristics of these patients.
There were no differences between non-enrollees and enrollees, particularly in terms of age, race, gender, insurance type, and CKD severity. Among non-enrollees, 22% reported interest in participating but did not return a survey. The median age of the full cohort of participants was 16 years old. Approximately 70% of the patients had mild CKD. In the prior year, the median specialty clinic attendance was four visits. The median total TRAQ score was 59.5 out of a total of 100 points. When this cohort was divided based on the completion of the follow-up survey, there were no statistical differences between cohorts.
Predictors
Table 2 depicts the association between predictors and baseline TRAQ scores. Age was consistently a positive predictor of higher TRAQ scores in the medication, appointment, and total score domains (p < 0.05). Male gender was a risk factor for lower TRAQ scores in the appointment and communication domains (p < 0.05). After adjusting for potential confounding factors, age was still a positive factor in the appointment domain. None of the other variables correlated with TRAQ scores.
Table 2: Predictors of transition readinessA single hyphen denotes a blank cell. A positive β indicates a protective predictor, whereas a negative β indicates a risk factor.* p < 0.05CKD, chronic kidney disease; TRAQ, Transition Readiness Assessment Questionnaire**
Transition readiness
A total of 27 of the 42 patients (64%) were eligible for the six-month follow-up survey. The remainder of the participants were ineligible, as they had been in the program for less than six months. Four patients were transferred to an adult provider, and one had passed away, leaving 22 patients in the follow-up analysis. These patients were noted to have used the handouts based on their receipt notification. Altogether, we received 14 follow-up surveys, with a return rate of 63.6%; nine patients were in the EO cohort and five were in the EC cohort. Across both cohorts, scores were significantly improved from baseline across all domains except appointments. In the total cohort, the total score improved by 25% in six months (Figure 2A). One-year TRAQ scores were not compared, as only three patients had available data. Further analysis showed that the EO cohort had significant improvements in all domains except communication; the EC cohort also showed significant improvements except in appointments (Figure 2B, 2C). When the relative improvements were compared in the EO and EC cohorts, we were not able to find a significant difference (p > 0.05).
Changes in TRAQ scores over six months p < 0.05Baseline scores are shown in blue. Handouts are given to all patients, addressing areas of deficit. A repeat evaluation of transition readiness is done six months later, with scores shown in green. The total cohort is shown in panel A. The total cohort is further broken down based on follow-up options: EO (panel B) and EC (panel C). In the EO option, patients are followed up at six months during reevaluation. In the EC option, patients are followed up at three months with a telephone call and again at six months during reevaluation.EC, education and coaching; EO, education only; TRAQ, Transition Readiness Assessment Questionnaire*
Feedback
All patients with completed follow-up surveys gave positive feedback. Major strengths included a structured curriculum, available resources, and routine follow-ups. Almost all parents reported that the project helped them realize the importance of transition planning. One commonly reported weakness was the lack of interactive material. Suggestions included the use of videos or animations and the employment of transition coordinators.
Discussion
This study signifies that demographic factors need to be considered in determining transition readiness in AYA with CKD. In this study, we have two significant findings: age and male gender. Older patients have higher TRAQ scores than younger patients. This result has been reported in a previous CKD study [15]. Additionally, the male gender is a risk factor for lower TRAQ scores. The female gender is possibly protective because of its greater developmental maturity [16]. However, the role of gender still remains mixed; some studies have found male gender to be a risk factor and others protective [17,18].
Our study also demonstrates the effectiveness of a remote transition curriculum. Across all TRAQ domains except in appointments, there have been score improvements over the past six months. When the total cohort is divided based on follow-up, we are not able to find more robust score improvements. In the EC cohort, there are only five patients, and these participants have higher baseline scores than the EO cohort. Such a difference and a small sample size can explain why we have not seen an additive improvement with closer follow-up. Regardless, these results imply that time-intensive interventions may not always be more effective. Feedback has been positive, with most patients citing the benefits of a structured curriculum. Additionally, caregivers have a greater appreciation for transition planning. Taken together, our data show that transition readiness can be improved with regular screening and a simple, structured curriculum; a resource-intense multidisciplinary clinic is not always necessary to help improve readiness [11,12].
There are several limitations to our study. First, this study uses a convenience sample and only has a participation rate of 27.8%. There can be a selection bias where only highly motivated patients are enrolled. Such a bias can overestimate the improvement in scores. Additionally, the sample size of follow-up surveys is small, making it difficult to draw more significant conclusions. Furthermore, there is only a six-month follow-up period. It can be helpful to see if scores are sustained or continue to improve. Our study does have three one-year follow-up surveys, and scores continue to improve. Finally, it is difficult to tease apart whether scores show improvement from the educational curriculum, the survey, or both. A mother, after completing the initial survey, once mentioned, “I did not realize how much I was doing for my son. It just became a habit.”
There are several future directions for this project. We hope to evaluate the effectiveness of implementing this project with males younger than 14 years of age. Our hypothesis is that males need more time in a structured program to improve their TRAQ scores. Additionally, we wish to evaluate the curriculum’s effectiveness with more participants. Next, we want to evaluate whether improved TRAQ scores at the time of transfer translate to less medical utilization, improved adherence, and less progression of kidney disease. Finally, we are working with the information technology team to automate this process using artificial intelligence [19]. Specifically, we are creating a program to have the EHR identify eligible patients and automatically send the transition surveys through the patient portal; additionally, the EHR will provide quick response codes that link to the appropriate resources based on survey responses.
Conclusions
Preparing for the pediatric-to-adult transition is crucial for limiting unnecessary medical utilization and poor longitudinal kidney outcomes. Unfortunately, there is scarce data on risk factors and best practices for improving transition readiness in patients with CKD. Similar to other subspecialty studies, our study adds to a growing body of literature that has found younger age and male gender to be risk factors for transition readiness. Additionally, our study shows that a structured, remote curriculum can improve transition readiness over a six-month period for pediatric patients in a CKD clinic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Transitional care interventions for youth with disabilities: a systematic review Pediatrics Levy BB Song JZ Luong D 146202010.1542/peds.2020-018733046586 · doi ↗ · pubmed ↗
- 2A long way from transfer to transition: challenges for pediatric and adult nephrologists Child Kidney Dis Lemke J Pape L Oh J 711222018
- 3National, Region, and State Health Care Transition Performance for Youth with and without Special Health Care Needs: The National Survey of Children’s Health 2019-2020 7 2023 2022 https://www.gottransition.org/resource/?state-regional-national-hct-performance-yschn
- 4Outcomes of pediatric to adult health care transition interventions: an updated systematic review J Pediatr Nurs Schmidt A Ilango SM Mc Manus MA Rogers KK White PH 921075120203198196910.1016/j.pedn.2020.01.002 · doi ↗ · pubmed ↗
- 5Prioritizing a research agenda of transitional care interventions for childhood-onset disabilities Front Pediatr Duncan A Luong D Perrier L 682078920213458944810.3389/fped.2021.682078 PMC 8475648 · doi ↗ · pubmed ↗
- 6Risk behaviors and emotional well-being in youth with chronic health conditions Child Health Care Erickson JD Patterson JM Wall M Neumark-Sztainer D 181192342005
- 7Depressive symptoms in children and adolescents with chronic physical illness: an updated meta-analysis J Pediatr Psychol Pinquart M Shen Y 3753843620112108807210.1093/jpepsy/jsq 104 · doi ↗ · pubmed ↗
- 8Transition navigator intervention improves transition readiness to adult care for youth with sickle cell disease Acad Pediatr Manwani D Doyle MH Davidson L 4224302220223438951610.1016/j.acap.2021.08.005 · doi ↗ · pubmed ↗