Alcohol Endotheliitis: A Report of a Rare Case
Deepaswi Bhavsar, Khushboo Goyal, Renu Magdum, Iqra Mushtaq, Shreya Gandhi

TL;DR
A rare case of sudden vision loss in a chronic alcoholic patient due to alcohol-induced eye inflammation is reported and treated with steroids.
Contribution
This paper presents a rare clinical case of acute toxic endotheliitis caused by ethanol toxicity in a chronic alcoholic patient.
Findings
A 60-year-old male experienced sudden vision loss and redness after heavy alcohol consumption.
The condition was diagnosed as acute toxic endotheliitis due to ethanol toxicity.
Treatment with corticosteroids led to recovery.
Abstract
Sudden transient loss of vision after an acute bout of alcohol consumption in patients with chronic alcoholism is rare. The underlying mechanism is a transient depression of the endothelial pump due to ethanol toxicity following a large amount of alcohol consumption in chronic alcoholic patients. Here, we report a rare case of a 60-year-old male patient who came to the outpatient department with complaints of sudden loss of vision associated with redness following a large amount of alcohol consumption. The case was managed by prompt diagnosis and topical and oral corticosteroid therapy. This is a rare case of acute toxic endotheliitis due to ethanol toxicity with only a few cases reported in the past.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
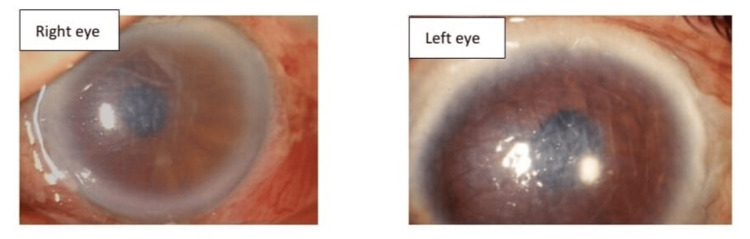 Figure 1
Figure 1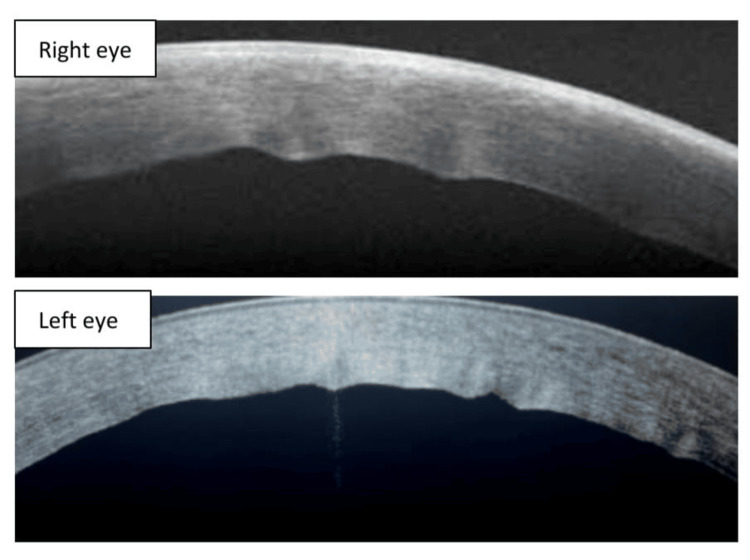 Figure 2
Figure 2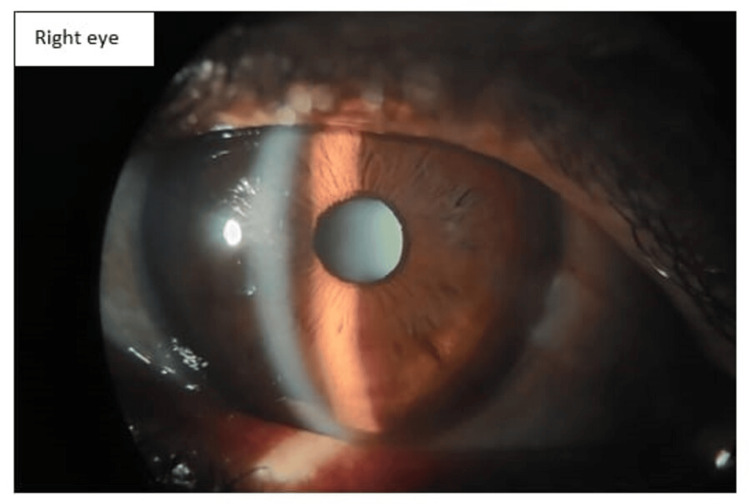 Figure 3
Figure 3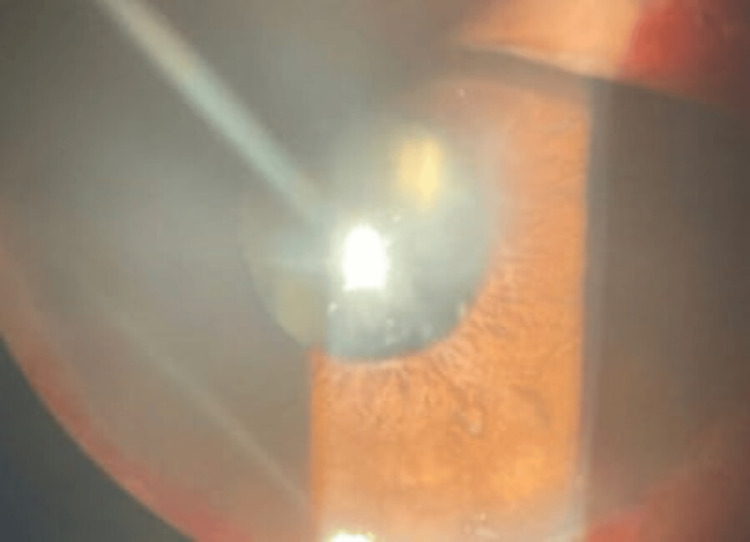 Figure 4
Figure 4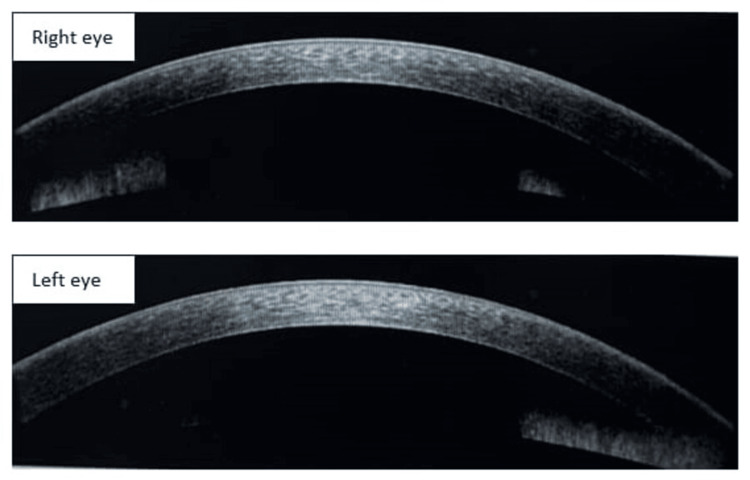 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Venomous Animal Envenomation and Studies · Antimicrobial Resistance in Staphylococcus
Introduction
The corneal endothelium is one of the important factors in maintaining corneal transparency by keeping the cornea in a relatively dehydrated state with the help of an endothelial pump. Any kind of inflammation in the corneal endothelium will lead to endotheliitis which subsequently leads to vision loss. Causes of endotheliitis include viral (most common), fungal, bacterial, drug-related, procedure-related, environmental, toxic, etc. [1]. The exact etiology of corneal edema is not known but it is presumed to be due to a transient depression in the endothelial pump activity which is caused by ethanol [2]. Ethanol and its metabolite acetaldehyde are presumed to cause toxic morphological and biochemical effects to the corneal endothelium and also to the stromal proteins [2].
We report a case of toxic endotheliitis due to ethanol poisoning after an episode of acute alcohol consumption in chronic alcoholic patients.
Case presentation
A 60-year-old alcoholic male came to the ophthalmology outpatient department with complaints of sudden diminution of vision associated with redness in both eyes. The patient gives a history of acute alcohol consumption in large amounts of local liquor approximately 500 to 525 ml one day back. There was no history of trauma or any history of similar attacks in the past. He had no known systemic illness. The patient has been a chronic alcoholic for the past 30 years with daily consumption of 30 to 60 ml of alcohol. The best corrected visual acuity in the right eye was 6\24 and that in the left eye was 1\60.
On examination, both eyes had evidence of diffuse conjunctival congestion. Corneal edema was present with dense stromal haze all over. Descemet membrane folds were present diffusely. The anterior chamber (AC) shows the reaction in both eyes with +3 cells and grade 2 flare. Iris and pupil were hazily seen but appeared within normal limits. The AC angle was wide open in both eyes according to Van Herick's grading (grade 4). Both eyes show grade 1 nuclear sclerosis in the lens (Figure 1). Fundus examination with direct and indirect ophthalmoscopy was tried but the retina was not visualized due to hazy media. On the B scan, the posterior segment was within normal limits with no evident edema of the optic nerve head.
Anterior segment photo of both eyes showing corneal edema and Descemet membrane folds at the time of presentation
On anterior segment optical coherence tomography (AS-OCT), there was increased thickness of the cornea with Descemet membrane folds present in both eyes (Figure 2). The central corneal thickness as measured was 630 microns in the right eye and 640 microns in the left eye.
Anterior segment optical coherence tomography photo of both eyes showing corneal edema with Descemet membrane folds at the time of presentation
The patient was diagnosed with alcohol-induced acute toxic endotheliitis. A differential diagnosis of viral endotheliitis was considered. However, the condition being bilateral and diffuse corneal involvement was against viral etiology. His complete blood cell counts were within normal limits ruling out an infectious etiology. He was started on steroids. Topically, eyedrop prednisolone acetate 1% was given twice hourly with eyedrop homatropine 2% at bedtime in both eyes. He was also started on the tablet Wysolone 60 mg (oral steroids) once a day.
The patient was followed up after two weeks. On slit-lamp examination, conjunctival congestion was markedly reduced. Corneal edema subsided and stromal haze was reduced. Minimal Descemet membrane folds were present. AC reaction subsided with no evidence of cells and flare. The patient’s steroid drop was tapered to six times a day. Tablet Wysolone was tapered to 50 mg and tapering was advised every five days. At the end of four weeks, the cornea was clear with minimal stromal haze present in the left eye and the right eye was within normal limits. Topical steroid drop was tapered four times and tapering was advised every five days. At the end of six weeks, the patient recovered completely with a vision of 6\12 in the right eye and 6\24 in the left eye with a normal anterior segment (Figures 3, 4).
Anterior segment photo of the right eye after six weeks of treatment showing resolved corneal edema
Anterior segment photo of the left eye after six weeks of treatment showing resolved corneal edema
AS-OCT of both eyes was normal with resolved corneal edema (Figure 5). The central corneal thickness as measured was 520 microns in the right eye and 540 microns in the left eye.
Anterior segment optical coherence tomography photo of both eyes showing resolved corneal edema after treatment of six weeks
Discussion
The above case is a rare presentation of bilateral corneal edema following an acute bout of alcohol consumption in chronic alcoholic patients. Toxic endotheliitis following ethanol toxicity is rare. Only a few cases were reported in the past. The mechanism involved is temporary suppression of endothelial pump activity which is supposed to be due to oxidative damage to endothelium stromal proteins by ethanol and aldehydes [2]. In endotheliitis, the patient presents with corneal edema, stromal haze, and Descemet membrane folds. Along with that keratic precipitates on endothelium and AC reaction is present commonly. Limbal ingestion and vascularization may also be present rarely [1].
Vision loss secondary to optic nerve head toxicity due to methanol poisoning is commonly seen in chronic alcoholic patients. Methanol is cheap and readily available. Hence, it is frequently adulterated in alcoholic beverages. Methanol and moreover its metabolite formic acid is responsible for toxic effects [3]. Our case is rare as vision loss is due to endothelial pump suppression due to ethanol toxicity leading to corneal edema.
Shiono et al. first reported corneal edema after intake of alcohol due to toxicity. Before that, alcohol was presumed to cause optic nerve head toxicity only [4]. In Ranjan et al. study of acute toxic endotheliitis following alcohol consumption, they have given IV steroids in addition to topical steroids, while in our study, IV steroid administration was not done [2].
Conclusions
Bilateral toxic endotheliitis following a large amount of alcohol consumption in chronic alcoholics is a rare presentation of endotheliitis. It is a reversible condition as vision loss is transient. Timely diagnosis and prompt treatment are the key. Other causes of sudden vision loss should be ruled out.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A review of corneal Endotheliitis and endotheliopathy: differential diagnosis, evaluation, and treatment Ophthalmol Ther Moshirfar M Murri MS Shah TJ 19521382019 https://pubmed.ncbi.nlm.nih.gov/30859513/3085951310.1007/s 40123-019-0169-7PMC 6514041 · doi ↗ · pubmed ↗
- 2Acute bilateral toxic endotheliitis following alcohol consumption Ocul Immunol Inflamm Ranjan A Murthy SI Rathi VM Sangwan VS 2692722620182749445710.1080/09273948.2016.1201121 · doi ↗ · pubmed ↗
- 3Visual blurring and metabolic acidosis after ingestion of bootlegged alcohol Hemodial Int Rathi M Sakhuja V Jha V 8141020061644182210.1111/j.1542-4758.2006.01169.x · doi ↗ · pubmed ↗
- 4Temporary corneal oedema after acute intake of alcohol Br J Ophthalmol Shiono T Asano Y Hashimoto T Mizuno K 462465711987362042710.1136/bjo.71.6.462PMC 1041200 · doi ↗ · pubmed ↗