Metachondromatosis: A Confusing Disease
Alejandro Blasco, Marta Salom, Francisco Giner, Emilio Baixauli, Francisco Baixauli

TL;DR
Metachondromatosis is a rare genetic disease involving abnormal PTPN11 gene function, causing bone tumors that can be difficult to diagnose and differentiate from other similar conditions.
Contribution
The paper presents a case study of a 5-year-old girl with metachondromatosis, highlighting atypical radiographic features and emphasizing the importance of differential diagnosis.
Findings
Multiple osteochondroma-like lesions grew toward the epiphysis, an atypical feature.
Columnar enchondroma-like lesions were found in multiple skeletal locations.
Some tumors regressed over time, a characteristic not commonly reported in similar diseases.
Abstract
Metachondromatosis is a rare autosomal dominant genetic disease with incomplete penetrance that involves abnormal function of the PTPN11 gene. Differentiation between chondrogenic tumors is a challenge for orthopedists. We report a case of a 5 year-old girl with metachondromatosis, a disease that shares attributes with osteochondromas and enchondromas. We found multiple osteochondroma-like lesions with the atypical characteristic of guiding its growth toward the neighboring joint (epyphisis) instead of moving away from it. Furthermore, columnar enchondroma-like lesions were clearly visible in the right distal radius, in the proximal femoral cervix and in the iliac crests. The patient reported that some other tumor had disappeared or downsized with time. This case was debated between a multidisciplinary skeletal dysplasia group. The aforementioned clinical and radiographic findings…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
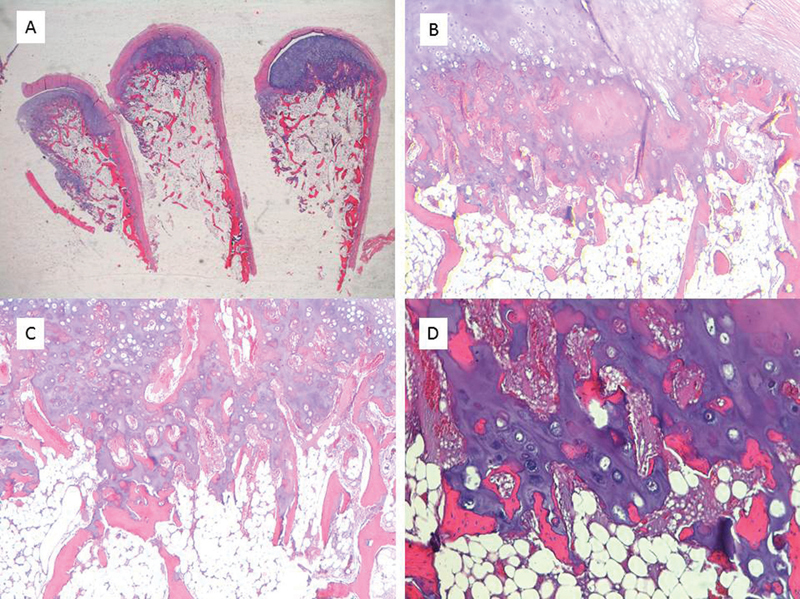 Fig. 1
Fig. 1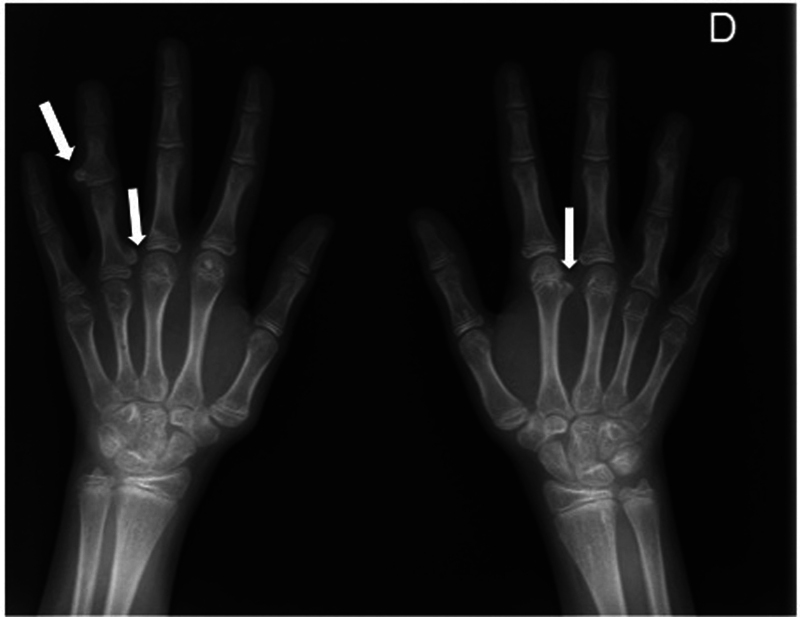 Fig. 2
Fig. 2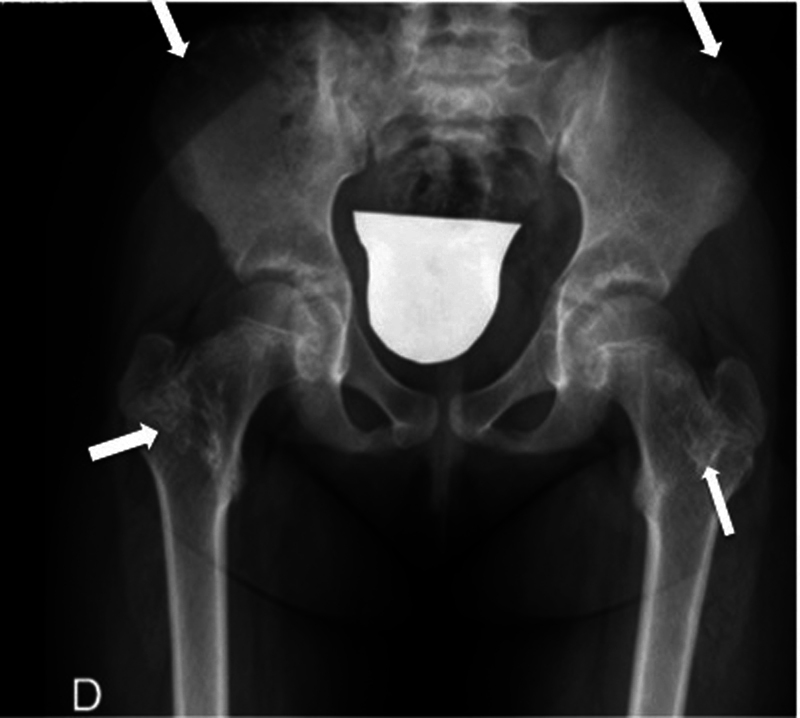 Fig. 3
Fig. 3| Enchondromas | Osteochondromas | Metacondromatosis | |
|---|---|---|---|
| Frequency |
10% of benign osseous tumors.
|
20–50% of all benign bone tumors and 10–15% of all bone tumors.
|
< 1/1,000,000, < 30 cases described.
|
| Location |
Frequently found in the hands more than in the foot and ankle bones, particularly in the phalanges.
|
Proximal humerus, tibia, and distal femur.
| Enchondroma-like lesions: Metaphyseal regions of the long bones and iliac crest |
| Genetics | Does not follow a clear Mendelian transmission pattern |
HMO is an autosomal dominant inherited trait.
|
Autosomal dominant
|
| Radiology |
Formation of hyaline cartilage in the medulla of a bone.
|
Cartilage pedunculated or sessile lumps outside the metaphyseal region of the long bones.
|
Epiphyseal-pointing osteochondroma-like lesions combined with calcified enchondroma-like lesions (
|
| Anatomopathological examination | On gross visual inspection, an enchondroma will appear as a bluish, semitranslucent, hyaline cartilage with a distinctly lobular arrangement. These lobules will vary from a few millimeters to a few centimeters in diameter. | Bony lesion covered with a pearly-white smooth cap |
42% as osteochondromas, 33% as enchondromas, 17% combined.
|
| Natural history | New lesions do not appear after skeletal maturation | New lesions do not appear after skeletal maturation | New lesions do not appear after skeletal maturation |
| Malignization |
5% in solitary enchondromas, >20% multiple enchondromatosis.
|
Between 0.4% and 2% in patients with solitary osteochondroma and between 1 and 4% in patients with HMO.
| No malignization |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Sarcoma Diagnosis and Treatment · Oral and Maxillofacial Pathology
Introduction
Osteochondromas are the most common benign cartilaginous tumor. Osteochondromas are typically metaphyseal tumors of the long bones (proximal humerus, tibia, and distal femur). They usually grow as pedunculated or sessile lesions composed of cortical tissue and with medullary bone tissue covered by a cartilaginous cap. 1
Enchondromas are the second most common benign cartilaginous tumor after osteochondroma. They are commonly found within the medullary cavity of the bones of the appendicular skeleton (more frequent in the hands than in the feet, particularly in the phalanges) and they are characterized by the formation of mature hyaline cartilage in the medullar cavity. 2
Metachondromatosis is a rare autosomal dominant genetic disease with incomplete penetrance that involves abnormal function of the PTPN11 gene. 1
Differentiation between chondrogenic tumors is a challenge for orthopedists. We report the case of a patient with metachondromatosis, a disease that shares attributes with osteochondromas and enchondromas.
Case Report
A 5-year-old girl was referred to our Pediatric Orthopedics Unit asking for evaluation of multiple osteochondromas. Physical examination revealed multiple painful tumor compatible with osteochondromas on radiography. Impairment for proximal interphalangeal (PIP) and distal interphalangeal (DIP) flexion of the fourth finger of the right hand was evidenced, which correlated with a middle phalanx osteochondroma. Previous history of skeletal hereditary diseases could not be confirmed. Surgical excision was performed without complications.
However, an anatomopathological examination showed multiple osseous and cartilaginous pieces compatible with the outer cap of a benign enchondroma. Eight months later, she was also operated for a growing and painful osteochondroma in the third left metacarpal and in the fourth right metacarpal. Paradoxically, in this case, the anatomopathological examination showed a 2.3 × 2 cm osseous lesion covered with a pearly-white smooth cap compatible with benign osteochondroma ( Fig. 1 ).
Images of different histological sections stained with hematoxylin-eosin. A) Sample of the exostotic lesion constituted by a cartilaginous cap with an osteoid central trabecular matrix, 2.5X. B) The chondral matrix shows mature characteristics with endochondral ossification, 4X. C) Transition zone between the peripheral cartilaginous component and trabecular bone resembling a slightly disorganized growth plate, 4X. D) Chondrocytes are arranged in isogenic groups, larger in the central portion, without atypia or atypical mitoses, 10X.
Previous radiographies were examined to find out a reason for this unexpected paradox. What we found was multiple osteochondroma-like lesions with the atypical characteristic of guiding its growth toward the neighboring joint (epiphysis) instead of moving away from it. Furthermore, columnar enchondroma-like lesions were clearly visible in the right distal radius, in the proximal femoral cervix and in the iliac crests ( Figs. 2 and 3 ). The patient reported that some other tumor had disappeared or downsized with time. This case was debated between a multidisciplinary skeletal dysplasia group. The aforementioned clinical and radiographic findings reinforced the hypothetical diagnosis of metachondromatosis.
Anteroposterior view of both hands showing multiple osteochondroma-like lesions with the atypical characteristic of guiding their growth toward the neighboring joint (epyphisis) instead of moving away from it.
Anteroposterior view of the pelvis. In metachondromatosis, enchondromas distribute mainly around the iliac crest and metaphyseal regions of the long bones.
After 8 years of follow-up, the patient is 13 years old, and new lesions in the right ankle, the hip, and the middle phalanx or the fourth left finger have grown, while others have regressed. However, she is asymptomatic, and she leads a normal life.
Discussion
Metachondromatosis combines multiple metaphyseal juxtaepiphyseal exostoses, metaphyseal enchondromas, periarticular calcifications, and frequent unilateral or bilateral Legg-Calvé-Perthes-like changes in the femoral head resembling osteonecrosis. 3 4 5
Classification: Metachondromatosis is a subtype of enchondromatosis without spinal affection, autosomal dominant transmission and osteochondroma-like lesions. 6
Etiology: Metachondromatosis is related with genetic abnormalities. Fisher et al. found 31 cases published. 1 Mutation of the PTPN11 gene (protein tyrosine phosphatase nonreceptor type 11) and lack of production of the tyrosine phosphatase SHP2 is related with the pathogenesis of metachondromatosis, as well as of other developmental diseases (Noonan syndrome, Noonan syndrome with multiple lentigines) and malignant diseases (juvenile myelomonocytic leukemia). 7 Mutation of the PTPN11 gene is inherited in an autosomal dominant pattern with incomplete penetrance and parents must be advised of it. Unlike enchondromatosis, EXT-1 and EXT-2 mutation (exostosin protein) is not observed in metachondromatosis. 1 7
The definitive diagnosis of metachondromatosis requires a combination of clinical, radiographical, and histopathological findings ( Table 1 ). 8
Clinical findings: The combination of multiple enchondromas and osteochondromas raises suspicion of metachondromatosis. 3 4 Metachondromatosis has characteristically epiphyseal-pointing osteochondroma-like lesions that can spontaneously regress, in contrast with conventional osteochondromas. 3 4
Radiographical findings: In metachondromatosis, enchondromas distribute mainly around the iliac crest and the metaphyseal regions of the long bones ( Fig. 3 ). In contrast, osteochondroma-like lesions are mainly distributed in the hands and feet ( Fig. 2 ). 6 In our case, we saw that these lesions can distribute in both the axial skeleton (pelvis, spine, scapula, and hip) and the appendicular skeleton (hands and feet). The hands were the most frequently affected locations in our case, which is in line with Fisher et al. 1 Metachondromatosis is not related with shortening and deformity of the long bones, a common feature of hereditary multiple exostosis. 4 As with osteochondromatosis and enchondromatosis, new lesions do not appear after skeletal maturation. 1
Histopathological findings: Histopathological examination reported first multiple osseous and cartilaginous pieces compatible with the outer cap of a benign enchondroma and, second, a bony lesion covered with a pearly-white smooth cap compatible with benign osteochondroma ( Fig. 1 ). However, sample size and location might determine a different diagnosis from the pathologist because they are difficult to differentiate. The histopathological analysis described by our pathologists is comparable to others that have been published. 1 After a review of the current literature on metachondromatosis, Fisher et al. found that 12 biopsies were studied; 42% (5/12) of the biopsies were diagnosed as osteochondromas, 33% (4/12) as enchondromas, and 17% (3/12) had multiple biopsies, some diagnosed as osteochondromas while some as enchondromas, as in our case. 1
Treatment
Conservative treatment is the treatment of choice, because of the regressive potential and the near absence of malignization. 2 5 Metachondromatosis is an autosomal dominant disorder, so genetic advice must be given to patients. We recommend periodical monitoring of the lesions.
Surgical treatment is reserved for painful lesions: neurovascular compression (for example, equinus secondary to nervus fibularis communis compression in the peroneal head) and avascular necrosis of the femoral head. 1 4 5
Differential diagnosis between enchondromas, osteochondromas and metachondromatosis is vital due to differences in malignization and natural history. When a patient has multiple enchondromas and osteochondromas with regression of some lesions and osteochondroma-like lesions with atypical radiographical characteristics pointing toward the epiphysis, metachondromatosis, a rare disease, must be considered. Risk of malignization is insignificant and genetic advice must be given due it is an autosomal dominant disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fisher T J Williams N Morris L Cundy P J Metachondromatosis: more than just multiple osteochondromas J Child Orthop 201370645546424432109 10.1007/s 11832-013-0526-3PMC 3886349 · doi ↗ · pubmed ↗
- 2Mc Farlane J Knight T Sinha A Cole T Kiely N Freeman R Exostoses, enchondromatosis and metachondromatosis; diagnosis and management Acta Orthop Belg 2016820110210526984661 · pubmed ↗
- 3Wittram C Carty H Metachondromatosis Pediatr Radiol 19952501 S 138S 1398577506 · pubmed ↗
- 4Wenger D R Birch J Rathjen K Tobin R Billman G Metachondromatosis and avascular necrosis of the femoral head: a radiographic and histologic correlation J Pediatr Orthop 199111032943002056076 · pubmed ↗
- 5Mavrogenis A F Skarpidi E Papakonstantinou O Papagelopoulos P J Chondrosarcoma in metachondromatosis: a case report J Bone Joint Surg Am 201092061507151320516327 10.2106/JBJS.I.00693 · doi ↗ · pubmed ↗
- 6Pansuriya T C Kroon H M Bovée J V Enchondromatosis: insights on the different subtypes Int J Clin Exp Pathol 201030655756920661403 PMC 2907117 · pubmed ↗
- 7Bowen M E Boyden E D Holm I A Loss-of-function mutations in PTPN 11 cause metachondromatosis, but not Ollier disease or Maffucci syndrome P Lo S Genet 2011704 e 100205021533187 10.1371/journal.pgen.1002050 PMC 3077396 · doi ↗ · pubmed ↗
- 8Chun K A Stephanie S Choi J Y Nam J H Suh J S Enchondroma of the Foot J Foot Ankle Surg 2015540583683926024560 10.1053/j.jfas.2015.01.002 · doi ↗ · pubmed ↗