Insidious Synovial Sarcoma of Bone in a Patient with Rheumatoid Arthritis
Juan Carlos Reyes Villarreal, Luis Francisco Pineda-Galindo, Olga Vera-Lastra, Elizabeth Natalia Quispe-Susara, Alberto Ordinola Navarro

TL;DR
A rare bone tumor was misdiagnosed as rheumatoid arthritis, leading to a fatal outcome due to delayed detection and complications.
Contribution
Highlights diagnostic challenges of synovial sarcoma when it originates in bone and lacks palpable mass.
Findings
Synovial sarcoma can present as hip pain without a palpable mass, leading to misdiagnosis.
Delayed diagnosis due to symptom overlap with rheumatoid arthritis can result in fatal outcomes.
Small or deep tumors are particularly challenging to detect and diagnose.
Abstract
Synovial sarcoma is a rare malignity of mesenchymal origin; the diagnostic approach usually begins by documenting a soft tissue tumor; however, it results in a challenging diagnosis when it is more profound, of small size, or primary from the bone. The present report describes a patient who presented insidious onset hip pain attributed to rheumatoid arthritis, with a fatal outcome due to baseline disease and surgery complications. The underestimation of hip pain, mainly when there is no palpable mass, may delay the diagnosis. Sarcoma sinovial é uma rara malignidade de origem mesenquimal; a abordagem diagnóstica geralmente começa documentando um tumor de tecido mole; no entanto, resulta em um diagnóstico desafiador quando é mais profundo, de pequeno porte ou primário do osso. O presente relato descreve um paciente que apresentou dor insidiosa no quadril atribuída a artrite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
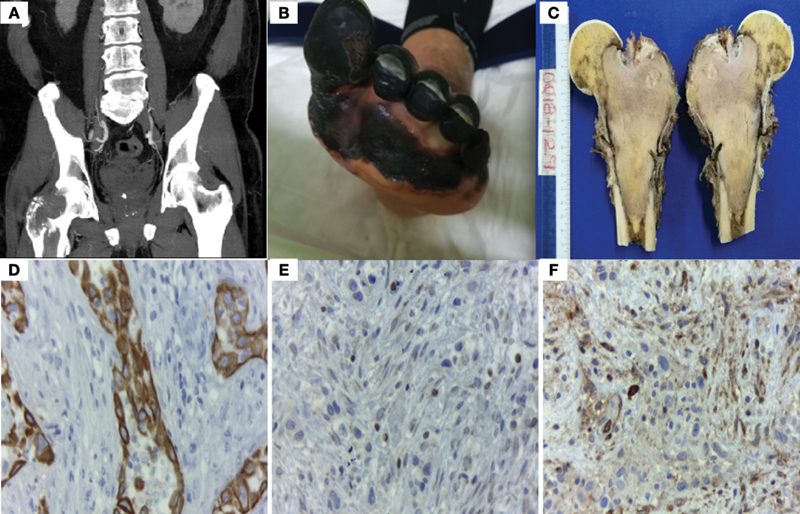 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal synovial abnormalities and treatments · Sarcoma Diagnosis and Treatment · Bone Tumor Diagnosis and Treatments
Introduction
Synovial sarcomas (SSs) are a rare mesenchymal neoplasm with capacities of dual differentiation; a periarticular soft-tissue mass is the most common presentation; however, it can arise from any site. 1 2 The underestimation of hip pain, mainly when there is no palpable mass or a soft-tissue tumor in imaging studies, may delay the diagnosis.
Case Report
A 67-year-old man with a 20-year history of rheumatoid arthritis (RA) started presenting with hip pain; he was evaluated by different departments, and the symptoms were attributed to RA and just symptomatic treatment was indicated.
A year later, he was referred to our hospital due to persistence of pain and edema in the lower limbs. A computed tomography (CT) scan was performed on hospitalization, reporting an osteolytic lesion in the neck and head of the femur ( Fig. 1A ). He developed deep venous thrombosis, which evolved into necrosis of the left toe; significant laboratory tests included positive serum cryoglobulins (polyclonal IgG and monoclonal IgM), elevated rheumatoid factor and hypocomplementaemia ( Fig. 1B ). He went to the operating room, where the right femoral head was resected and a proximal femur megaprosthesis was placed ( Fig. 1C ). During the postoperative period, the patient developed an infection at the surgical site; he was treated with antibiotics, wound cleansing and debridement. The histological diagnosis revealed: epithelial and spindle cells positive for cytokeratin 7, BCL2 and CD99. Molecular studies with translocation t(X;18) (p11.2; q11.2), and SS18-SSX1 fusion proteins expression, corroborated biphasic the diagnosis of SS. However, the patient had complications with cerebrovascular disease and pulmonary thromboembolism and died.
(A) Computed tomography scan showing osteolytic lesion in the neck and head of the femur. (B) Deep venous thrombosis with distal necrosis. (C) Right femoral neck and head showing intraosseous infiltration. (D-F) Immunohistochemistry. The identification of CK7 (D), BCL-2 (E), and CD99 (F) were the key in suspecting the diagnosis of synovial sarcoma.
Discussion
The present report describes a patient who presented insidious onset hip pain attributed to RA, with a fatal outcome due to baseline disease and surgery complications.
Synovial sarcoma is a rare malignity of mesenchymal origin that comprises approximately up to 10% of soft tissue sarcomas. It may present in any anatomic site, but SS arising from soft tissue is the most common presentation. 1 Synovial sarcoma as a primary bone tumor is relatively rare, and it is more frequent in young adult patients. 2
Synovial sarcoma was initially described as a biphasic neoplasm comprising both epithelial and spindle cell components; however, histologic variants such as monophasic, biphasic, and poorly differentiated have been identified. 1 2 According to the reported series, the main symptoms are neuropathic and local pain, motor deficit, and palpable mass; in our patient, the insidious symptomatology and history of rheumatic disease delayed the diagnosis. 3
The diagnostic approach usually begins by documenting a soft tissue tumor; when it is superficial, it is easy to identify it; however, when it is more profound, of small size, or primary from bone, imaging studies showing internal hemorrhage, calcification or osteolytic lesions can help us to guide our diagnostic suspicion. 2 In our patient, a CT scan was performed, in which no tumor was found; however, a right femoral head osteolytic lesion was reported, which led to the suspicion of bone tumor.
Immunohistochemistry is essential in suspecting the diagnosis. In this patient, CK7, CD99 and BCL2 enabled suspecting the diagnosis and classifying the tumor as biphasic, since CK7 is found in epithelial cells and CD99, along with BCL2, are found in spindle cells ( Fig. 1 D-F ). 4
Synovial sarcoma has a pathognomonic translocation between chromosomes X and 18, t (X;18) (p11.2;q11.2), translating into several different expressions of SS18:SSx fusion proteins; with SS18-SSX1 and SS18:SSX2 being the most common. After immunohistochemistry, it was possible to corroborate the diagnosis demonstrating the translocation and fusion proteins expression; the fusion is detectable in > 95% of cases, being a key tool to confirm the diagnosis. 1 4
Metastatic disease is present in 24% of patients at the time of diagnosis; the prognosis for patients without metastasis is favorable. However, metastasis occurs in 50 to 70% of cases, and most develop in the lungs, followed by bone and liver. The standard treatment is surgical resection for localized SSs with consideration of using adjuvant radiation and/or systemic anticancer therapy. However, there is no standard approach for the use of systemic therapy. When prescribed, anthracycline plus ifosfamide are usually the first-line therapy. Nevertheless, future clinical trials would define an appropriate treatment for this disease. 5 The knowledge of the disease can help to guide immunohistochemistry, corroborating the diagnosis and starting an individualized therapy that leads to better outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stacchiotti S Van Tine B A Synovial Sarcoma: Current Concepts and Future Perspectives J Clin Oncol 2018360218018729220290 10.1200/JCO.2017.75.1941 · doi ↗ · pubmed ↗
- 2Caracciolo J T Henderson-Jackson E Binitie O Synovial sarcoma of bone: Sarcoma typically of soft tissues presenting as a primary bone tumor Radiol Case Rep 2018140220420730425775 10.1016/j.radcr.2018.10.026PMC 6231113 · doi ↗ · pubmed ↗
- 3Burks S S Puffer R C Cajigas I Synovial Sarcoma of the Nerve-Clinical and Pathological Features: Case Series and Systematic Review Neurosurgery 20198506 E 975E 99131435657 10.1093/neuros/nyz 321PMC 6891799 · doi ↗ · pubmed ↗
- 4Jones K B Barrott J J Xie M The impact of chromosomal translocation locus and fusion oncogene coding sequence in synovial sarcomagenesis Oncogene 201635385021503226947017 10.1038/onc.2016.38PMC 5014712 · doi ↗ · pubmed ↗
- 5Riedel R F Jones R L Italiano A Systemic Anti-Cancer Therapy in Synovial Sarcoma: A Systematic Review Cancers (Basel)2018101141730388821 10.3390/cancers 10110417 PMC 6267101 · doi ↗ · pubmed ↗