Laparoscopic Treatment of a Symptomatic Young Woman With Median Arcuate Ligament Syndrome
Zoi Nitsa, Prodromos Kanavidis, Natasha Hasemaki, Athanasios Katsargyris, Alexandros Charalabopoulos

TL;DR
A young woman with severe abdominal symptoms was diagnosed with and surgically treated for median arcuate ligament syndrome.
Contribution
This case report presents a rare instance of symptomatic MALS in a young woman successfully treated with laparoscopic surgery.
Findings
A 27-year-old woman experienced postprandial abdominal pain and vomiting due to MALS.
Laparoscopic surgery was performed and provided symptom relief.
MALS should be considered in young patients with unexplained gastrointestinal symptoms.
Abstract
Median arcuate ligament syndrome (MALS), also known as Dunbar syndrome, celiac axis syndrome, or celiac artery compression syndrome, is caused by a band of tissue called the median arcuate ligament that compresses the celiac artery and sometimes the celiac plexus too. MALS does not always cause symptoms, but when symptoms occur, surgery is the treatment of choice. This case report focuses on the case of a 27-year-old woman presenting with postprandial episodes of abdominal pain and vomiting accompanied by loss of weight, which was found to be MALS.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1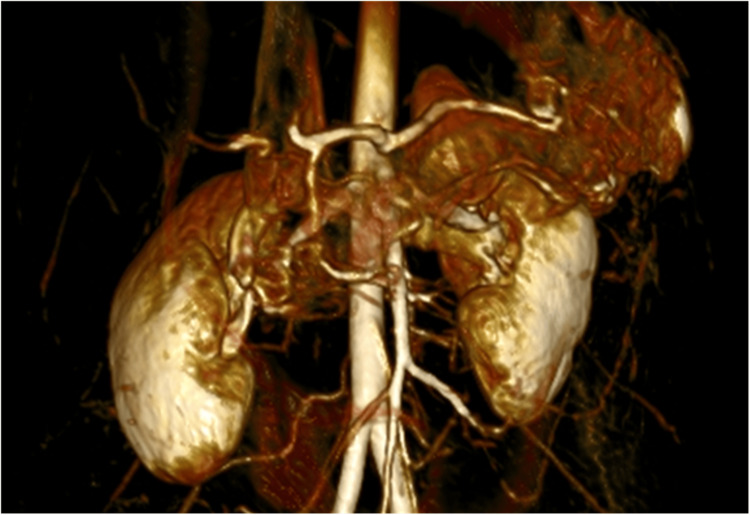 Figure 2
Figure 2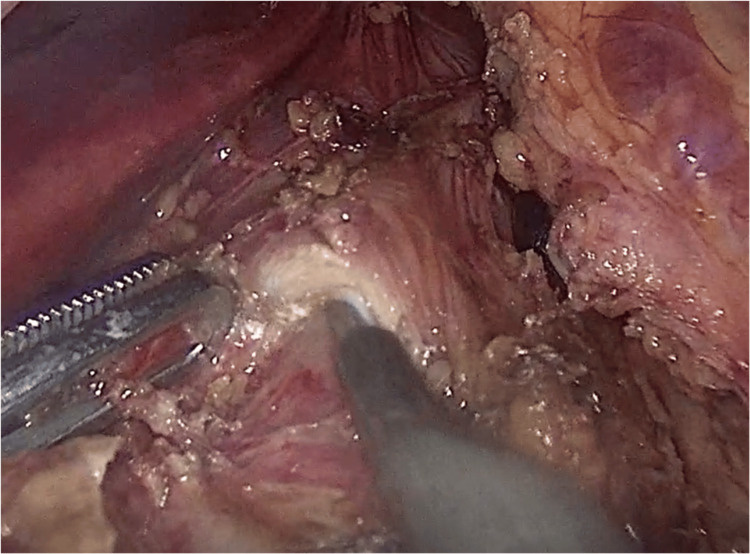 Figure 3
Figure 3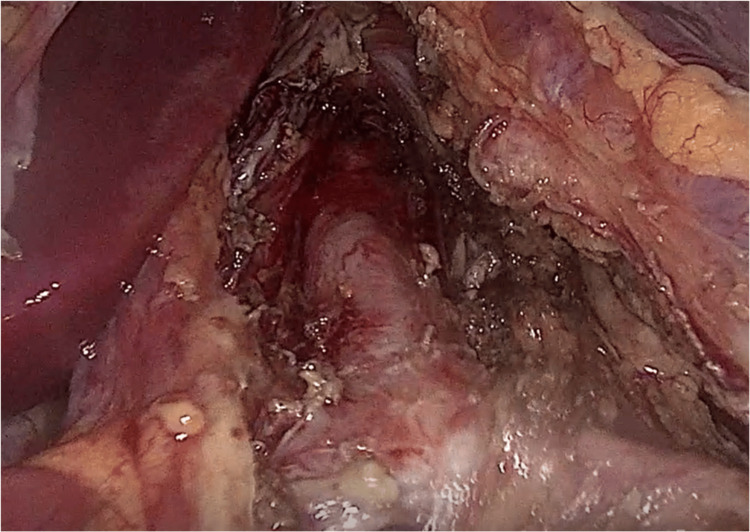 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Vascular anomalies and interventions · Omental and Epiploic Conditions
Introduction
Median arcuate ligament syndrome (MALS) can cause symptoms like abdominal pain, nausea, vomiting after a meal, and diarrhea that can lead to fear of eating and significant weight loss. Surgical treatment consists of decompression of the celiac artery by dissecting the abnormal median arcuate ligament, which passes over the origin of the celiac trunk instead of above it [1]. Surgical treatment does not always lead to symptom resolution, and some of the patients are still having the same symptoms as before [2].
Case presentation
A 27-year-old woman presented with a nine-month history of weight loss, postprandial abdominal pain, and episodes of vomiting and diarrhea. The blood tests, ultrasound study, and endoscopy did not show any abnormalities. The patient underwent CT with intravenous contrast fluid infusion (Figure 1), later MR angiography (MRA) (Figure 2), and a triplex ultrasound study of the aorta and visceral branches, the results of which indicated MALS, with an expiratory peak celiac artery flow of 300 cm/s and almost complete flow obstruction at intense expiration.
CT (sagittal plane) showing a hook-like signCT: computed tomography
MRA 3D reconstruction of the celiac trunkMRA: magnetic resonance angiography, 3D: three dimensional
The patient was treated laparoscopically by surgical release of the celiac artery and plexus from the pressure of the median arcuate ligament and lymphatic tissue (Figures 3-4). The operation lasted 35 minutes, and the blood loss was estimated to be 30 ml. On postoperative day 1, the patient was started on a clear liquid diet without postprandial abdominal pain or vomiting/diarrhea. The patient was discharged three days later, after progressing to a free diet and having an uncomplicated postoperative course.
Release of the celiac trunk from the abnormal median arcuate ligament
Released celiac trunk
The patient remained asymptomatic, tolerated food intake adequately, and gained 4 kg of weight in the first three months. She underwent a triplex study of the aorta and visceral branches with satisfactory results and improvement of the peak expiratory celiac artery flow (255 cm/s).
Discussion
The MAL syndrome includes a set of clinical signs and symptoms resulting from compression of the celiac trunk and plexus by the median arcuate ligament. MALS, however, does not always cause symptoms. This has caused controversy because stenosis in the celiac artery will not always manifest postprandial ischemia in the gastric mucosa due to the development of collateral vasculature that provides sufficient blood flow so as not to cause symptoms and pain. Another possible factor is the compression of the celiac ganglion, which leads to the stimulation of sympathetic pain fibers and fibers of vasoconstriction [3]. The symptoms of MALS may vary, including postprandial abdominal pain, vomiting, diarrhea, and weight loss. Due to the similar symptoms with other more common diseases, the diagnosis of MALS is usually made by exclusion [4]. The diagnosis of MALS is made by duplex ultrasound, which diagnoses the stenosis of the celiac trunk by the expiratory peak systolic flow velocities (sometimes more than 350 cm/s) and deflection angle (>50°). In addition, CT angiography is an important diagnostic tool because it can assess the whole abdominal cavity, and in cases of MALS, it can show a hook-like sign of the celiac trunk that differentiates from atherosclerosis. MRA and digital subtraction angiography are alternative choices [5]. Recent studies have shown that a reverse flow in the gastro-duodenal artery, measured either by ultrasound or MRA, can be a marker of equal or better sensitivity than celiac artery stenosis, with reverse flow being observed from 35% stenosis and greater [3]. This could lead to a better selection of patients, a better correlation with symptoms, and possibly better outcomes. Surgical treatment is currently recommended only for symptomatic patients with 50% stenosis of the celiac artery [6]. The treatment consists of decompression of the celiac trunk, traditionally by an open approach. Recently, however, minimally invasive approaches such as laparoscopic or robotic are more often used, with similar or better results [7,8]. Data from cohorts of laparoscopic MALS decompression seems to show fewer postoperative complications, pain, and a shorter length of stay compared with the open approach [9]. Almost 70% of operated patients experience relief of symptoms [2]. With regards to the patients who continue to have unresolved symptoms, vascular bypass or angioplasty is the next step in treatment, while some patients benefit from celiac ganglion neurolysis or ablation [10].
Conclusions
The MAL syndrome has a direct impact on the patient’s life, while the exact incidence of the disease is unknown. The exact pathophysiologic mechanism is not known; however, due to the low incidence of the disease, there are no guidelines for treatment. The laparoscopic decompression of the celiac artery in specialized centers seems to have promising results, with prompt relief of symptoms as well as immediate recovery and a quick return to daily activities, avoiding the complications of open surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Compression of the celiac trunk and abdominal angina Am J Roentgenol Radium Ther Nucl Med Dunbar JD Molnar W Beman FF Marable SA 73174495196510.2214/ajr.95.3.7315844938 · doi ↗ · pubmed ↗
- 2Systematic review of the efficacy of treatment for median arcuate ligament syndrome Eur J Vasc Endovasc Surg Metz FM Blauw JT Brusse-Keizer M Kolkman JJ Bruno MJ Geelkerken RH 7207326420223607554110.1016/j.ejvs.2022.08.033 · doi ↗ · pubmed ↗
- 3Perioperative microcirculatory changes detected with gastroscopy assisted laser Doppler flowmetry and visible light spectroscopy in patients with median arcuate ligament syndrome Vasc Health Risk Manag Berge ST Safi N Medhus AW Sundhagen JO Hisdal J Kazmi SS 3313411620203298226210.2147/VHRM.S 252192 PMC 7493022 · doi ↗ · pubmed ↗
- 4Median arcuate ligament syndrome Curr Treat Options Cardiovasc Med Duncan AA 1121161020081832531310.1007/s 11936-008-0012-2 · doi ↗ · pubmed ↗
- 5Median arcuate ligament syndrome J Vasc Surg Goodall R Langridge B Onida S Ellis M Lane T Davies AH 217021767120203188231410.1016/j.jvs.2019.11.012 · doi ↗ · pubmed ↗
- 6Robot assisted laparoscopy for median arcuate ligament syndrome relief EJVES Vasc Forum Magnus L ChakféN Lejay A Thaveau F 32365620223603589110.1016/j.ejvsvf.2022.06.002PMC 9399280 · doi ↗ · pubmed ↗
- 7Multimedia article. Laparoscopic management of median arcuate ligament syndrome Surg Endosc Carbonell AM Kercher KW Heniford BT Matthews BD 7291920051596558810.1007/s 00464-004-6010-x · doi ↗ · pubmed ↗
- 8Laparoscopic release of celiac artery compression syndrome facilitated by laparoscopic ultrasound scanning to confirm restoration of flow J Vasc Surg Roayaie S Jossart G Gitlitz D Lamparello P Hollier L Gagner M 8148173220001101304610.1067/mva.2000.107574 · doi ↗ · pubmed ↗