Laparoscopy is non‐inferior to open surgery for rectal cancer: A systematic review and meta‐analysis
Ling Ma, Hai‐jiao Yu, Yu‐bing Zhu, Wen‐xia Li, Kai‐yu Xu, Ai‐min Zhao, Lei Ding, Hong Gao

TL;DR
Laparoscopic surgery for rectal cancer is as effective as open surgery in the long term and offers faster recovery and fewer complications in the short term.
Contribution
This is the largest meta-analysis to date showing laparoscopy is non-inferior to open surgery for rectal cancer.
Findings
Laparoscopic surgery reduced 30-day mortality, complications, and recovery time compared to open surgery.
Laparoscopy showed lower positive circumferential and distal margin rates, with no difference in mesorectal excision completeness.
Laparoscopic surgery improved 3- and 5-year local recurrence, disease-free survival, and overall survival.
Abstract
Laparoscopic surgery has been endorsed by clinical guidelines for colon cancer, but not for rectal cancer on account of unapproved oncologic equivalence with open surgery. We started this largest‐to‐date meta‐analysis to comprehensively evaluate the safety and efficacy of laparoscopy in the treatment of rectal cancer compared with open surgery. Both randomized and nonrandomized controlled trials comparing laparoscopic proctectomy and open surgery between January 1990 and March 2020 were searched in PubMed, Cochrane Library and Embase Databases (PROSPERO registration number CRD42020211718). The data of intraoperative, pathological, postoperative and survival outcomes were compared between two groups. Twenty RCTs and 93 NRCTs including 216,615 patients fulfilled the inclusion criteria, with 48,888 patients received laparoscopic surgery and 167,727 patients underwent open surgery.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
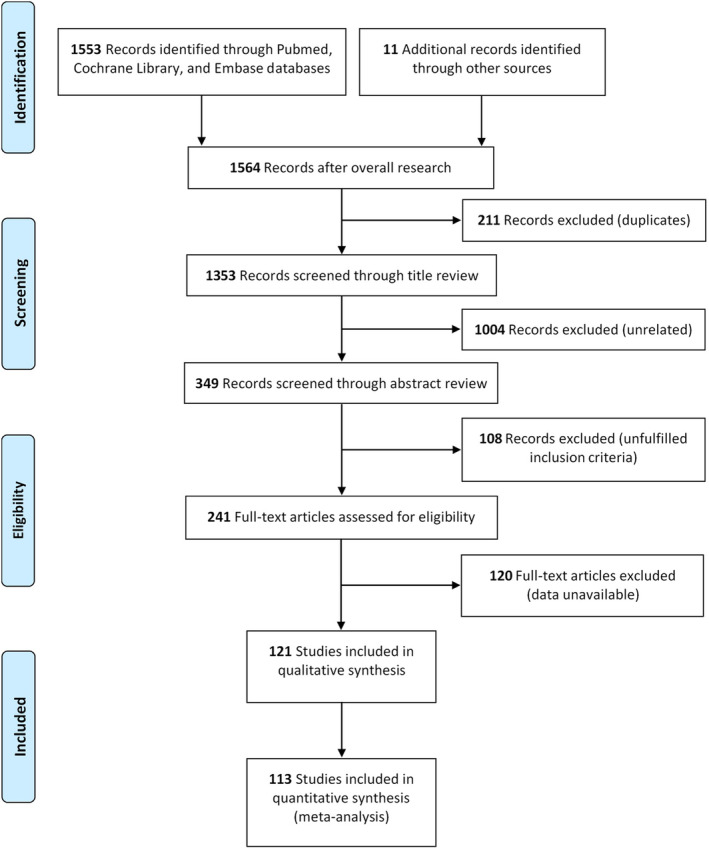 FIGURE 1
FIGURE 1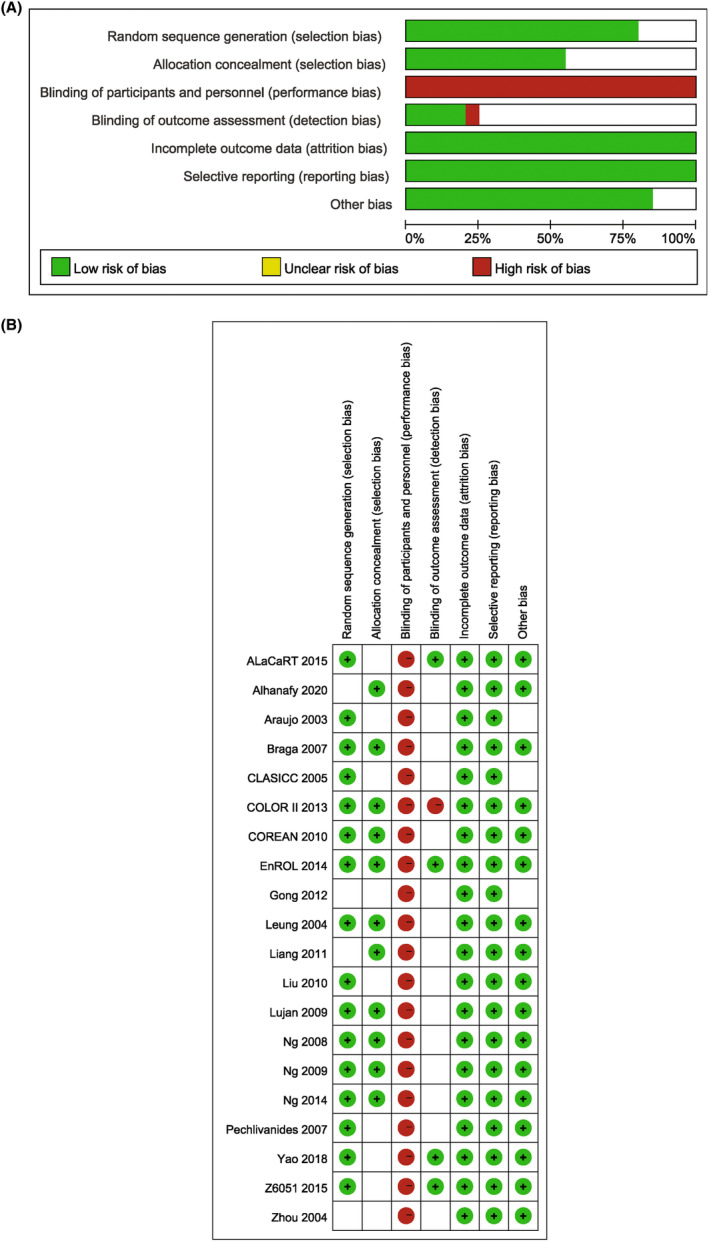 FIGURE 2
FIGURE 2| Reference | Area | Study type | Period | Inclusion criteria | Medical center included | Number of participants | Surgical approach | Conversion rate (%) | Neoadjuvant treatment | Follow up time (month) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lap ( | Open ( | Lap/open | Lap | Open | ||||||||
| Araujo | Brazil | RCT, P | September 1997–September 2000 | Distal rectal cancer with nCRT | Single | 28 | 13 | 15 | 0 | 15/13 | 47.2 | 47.2 |
| Leung | Hong Kong, China | RCT, P | September 1993–October 2002 | Rectosigmoid cancer | Single | 403 | 203 | 200 | 23.2 | 55/77 | 52.7 (38.9) | 49.2 (35.4) |
| Zhou | China | RCT, P | June 2001–September 2002 | Low rectal cancer, within 1.5–8 cm from DL | Single | 171 | 82 | 89 | ND | ND | (1–16) | (1–16) |
| CLASICC | UK | RCT, P | July 1996–July 2002 | Colorectal cancer | 27 | 381 | 253 | 128 | 0 | ND | 62.9 (22.9–92.8) | 62.9 (22.9–92.8) |
| Braga | Italy | RCT, P | ND | Rectal cancer | Single | 168 | 83 | 85 | 7.2 | 14/12 | 53.6 | 53.6 |
| Pechlivanides | Greece | RCT, P | ND | Mid and low rectal cancer, within 12 cm from AV | Single | 73 | 34 | 39 | 3 | 13/17 | ND | ND |
| Ng | Hong Kong, China | RCT, P | July 1994–February 2005 | Low rectal cancer, within 5 cm from AV | Single | 99 | 51 | 48 | 9.8 | 0/0 | 87.2 (22.8–150.0) | 90.1 (27.0–145.5) |
| Lujan | Spain | RCT, P | January 2002–February 2007 | Mid and low rectal cancer | Single | 204 | 101 | 103 | 7.9 | 73/77 | 32.8 (18.9) | 34.1 (20.0) |
| Ng | Hong Kong, China | RCT, P | September 1993–October 2002 | Rectosigmoid junction and upper rectal cancer, within 12–15 cm from AV | Single | 153 | 76 | 77 | 30.3 | 24/46 | 112.5 (71.1–168.3) | 108.8 (69.8–168.7) |
| COREAN | Korea | RCT, P | April 2006–August 2009 | cT3N0–2M0 mid or low rectal cancer, after nCRT | 3 | 340 | 170 | 170 | 1.18 | 170/170 | 47.65 (37–56) | 46.35 (38–57) |
| Liu | China | RCT, P | February 2005–October 2008 | Rectal cancer | Single | 186 | 98 | 88 | 0 | ND | 16.3 | 16.3 |
| Liang | China | RCT, P | May 2004–April 2008 | Nonmetastatic rectal cancer without adjuvant therapy | Single | 343 | 169 | 174 | 0.59 | 0/0 | 44 (1–72) | 44 (1–72) |
| Gong | China | RCT, P | September 2008–July 2011 | Mid and low rectal cancer | Single | 138 | 67 | 71 | 2.99 | ND | 21 (9–56) | 21 (9–56) |
| COLOR II | Belgium et al | RCT, P | January 2004–May 2010 | Rectal cancer, within 15 cm from AV, without evidence of distant metastases | 30 | 1044 | 699 | 345 | 17 | 608/298 | 36 | 36 |
| Enroll | UK | RCT, P | July 2008–April 2012 | Rectal cancer (colorectal cancer) | 12 | 56 | 29 | 27 | 8 | ND | 12 | 12 |
| Ng | Hong Kong, China | RCT, P | August 2001–August 2007 | Mid and low rectal cancer | Single | 80 | 40 | 40 | 7.5 | ND | 75.7 (16.9–115.7) | 76.1 (4.7–126.6) |
| ALaCaRT | Australia | RCT, P | March 2010–November 2014 | T1‐T3 rectal cancer, within 15 cm from AV | 24 | 473 | 238 | 235 | 9 | 119/116 | 38.4 (36–49.2) | 39.6 (36–50.4) |
| Z6051 | USA and Canada | RCT, P | October 2008–September 2013 | Stage II or III rectal cancer within 12 cm from AV | 35 | 462 | 240 | 222 | 11.3 | 240/222 | 47.7 (26.1–59.1) | 48.1 (33.9–59.8) |
| Yao | China | RCT, P | May 2014–February 2016 | Rectal cancer with nCRT | Single | 120 | 60 | 60 | 0 | 60/60 | 1 | 1 |
| Alhanafy | Turkey | RCT, P | February 2017–February 2019 | Rectal cancer | Single | 120 | 60 | 60 | 8.33 | 30/27 | 1 | 1 |
| Schwandner | Germany | NRCT, R, CCS | September 1992–January 1998 | Rectosigmoid or rectal cancer | Single | 64 | 32 | 32 | 0 | ND | 33.1 (24.2) | 31.0 (17.9) |
| Leung | Hong Kong, China | NRCT, R | January 1993–January 1996 | Low rectal cancer | Single | 59 | 25 | 34 | 4 | ND | 30.1 (6.0–52.3) | 28.3 (1.9–55.1) |
| Hartley | UK | NRCT | December 1993–October 1998 | Rectal cancer | Single | 43 | 21 | 22 | 0 | ND | 38 (6–53) | 38 (6–53) |
| Anthuber | Germany | NRCT, R | January 1996–March 2002 | Rectal cancer | Single | 435 | 101 | 334 | 10.9 | 27/116 | 17 | 17 |
| Feliciotti | Italy | NRCT, R | May 1992–April 2002 | Rectal cancer | Single | 124 | 81 | 43 | 12.3 | 75/38 | 43.8 (12–108) | 43.8 (12–108) |
| Wu | China | NRCT, R, CCS | April 2002–May 2003 | Rectal cancer | Single | 36 | 18 | 18 | 0 | 0/0 | 1 | 1 |
| Bretagnol | France | NRCT, R, CCS | September 2000–September 2004 | Mid and low rectal cancer, within 12 cm from AV | 2 | 288 | 144 | 144 | 14 | 120/115 | 18 (1–46) | 18 (1–46) |
| Breukink | Netherlands | NRCT, R, CCS | April 1996–March 2003 | Rectal cancer after nCRT | Single | 82 | 41 | 41 | 10 | 41/41 | 14 (2–31) | 14 (2–31) |
| Morino | Italy | NRCT, P, CCS | April 1994–April 2002 | Mid and low rectal carcinoma, within 12 cm from AV | Single | 191 | 98 | 93 | 18.4 | ND | 46.3 (12–132) | 49.7 (12–132) |
| Sahakitrungruang | Thailand | NRCT, R | June 2004–May 2005 | Rectosigmoid or rectal cancer | Single | 49 | 24 | 25 | 8.3 | ND | 1 | 1 |
| Law | Hong Kong, China | NRCT, R | June 2000–December 2004 | Upper and mid cancer, within 8–20 cm from AV | Single | 265 | 98 | 167 | 12.2 | ND | 21.2 (4.1–56.7) | 21.2 (4.1–56.7) |
| Wong | Hong Kong China | NRCT, P | March 1994–December 2003 | Low rectal and anal canal cancer | Single | 102 | 71 | 31 | 15.5 | 6/0 | 46 (6–100) | 50 (6–123) |
| Lelong | France | NRCT, P, CCS | January 1998–September 2004 | Rectal cancer | Single | 172 | 104 | 68 | 14.5 | ND | 3 | 3 |
| Staudacher | Italy | NRCT | January 1998–September 2005 | Mid and low rectal cancer | Single | 187 | 108 | 79 | 12 | 68/34 | 27.6 (6–82) | 27.6 (6–82) |
| Veenhof | Netherlands | NRCT, R, CCS | February 1999–November 2005 | Rectal cancer | Single | 100 | 50 | 50 | 8 | 26/26 | 17 (6–26) | 22 (10–38) |
| Ströhlein | Germany | NRCT, P | 1998–2005 | Rectal cancer | 2 | 389 | 114 | 275 | 21.9 | 56/174 | 31.1 (2–71) | 32.6 (1–76) |
| Ding | China | NRCT, R, CCS | January 2004–December 2005 | RECTAL cancer | 3 | 335 | 115 | 220 | 11.3 | ND | 20 (11) | 20 (11) |
| González | Mexico | NRCT, P | November 2005–November 2007 | Mid and low rectal cancer | Single | 56 | 28 | 28 | 0 | ND | (9–24) | (9–24) |
| Gouvas | Greece | NRCT, R, CCS | January 1998–March 2007 | Mid and low rectal cancer, within 10 cm from AV | 4 | 88 | 45 | 43 | 9 | 15/11 | 3 | 3 |
| Khaikin | America | NRCT, R | November 2004–July 2006 | Rectal cancer | Single | 82 | 32 | 50 | 12.5 | 18/31 | 10 (1–18) | 10 (1–18) |
| Kim | Korea | NRCT, R | 1994–2004 | Rectal cancer | Single | 407 | 272 | 135 | 4 | ND | 52 (25–129) | 180 (29–263) |
| Koulas | Greece | NRCT, R | October 1998–December 2006 | Rectal cancer | Single | 117 | 57 | 60 | 7.01 | ND | 38 | 78 |
| Laurent | France | NRCT, R | 1994–2006 | Rectal cancer, within 15 cm from AV | Single | 471 | 238 | 233 | 15.1 | 178/149 | 52 (1–151) | 52 (1–151) |
| Law |
Hong Kong China | NRCT, R | June 2000–December 2006 | Rectal cancer | Single | 421 | 111 | 310 | 12.5 | 7/47 | 34 | 34 |
| Biondo | Spain | NRCT, R | May 2006–May 2008 | Rectal cancer | 7 | 604 | 209 | 395 | ND | 138/231 | 1 | 1 |
| Denoya | America | NRCT, R, CCS | 1997–2005 | Mid and low rectal cancer after nCRT | Single | 64 | 32 | 32 | 28 | 32/32 | 1 | 1 |
| Feng | China | NRCT, R | January 2003–May 2005 | Rectal cancer | Single | 173 | 87 | 86 | 0 | 0/0 | 50 (36–65) | 49 (36–64) |
| Fujimoto | Japan | NRCT, R | July 2005–December 2008 | Very low rectal cancer, below 5 cm from dentate line | Single | 54 | 35 | 19 | 3 | 11/6 | 19 (5–42) | 19 (5–42) |
| Baik | America | NRCT, R, CCS | September 2001–September 2009 | Rectal cancer, within 12 cm from AV | Single | 162 | 54 | 108 | 11.1 | 43/89 | 59 | 59 |
| da Luz Moreira | USA | NRCT, R, CCS | 1992–2008 | Rectal cancer | Single | 182 | 91 | 91 | 18.6 | 30/30 | 40 (7–179) | 40 (7–179) |
| Greenblatt | America | NRCT, R | 2005–2009 | Rectal cancer | Multiple | 5420 | 1040 | 4380 | ND | 377/2002 | 1 | 1 |
| June | Korea | NRCT, R | December 2007–July 2009 | Rectal cancer | Single | 211 | 123 | 88 | 0 | 10/9 | 1 | 1 |
| Li | China | NRCT, P | January 2000–June 2005 | Mid and low rectal cancer, within 10 cm from AV | Single | 236 | 113 | 123 | 5.3 | 39/46 | 76 (30.3) | 73.6 (30.5) |
| Park | Japan and Korea | NRCT, R | January 1997–December 2009 | Low rectal cancer | 2 | 210 | 130 | 80 | 0 | 10/1 | 32.5 (16–41.5) | 37 (25–45.2) |
| Yamamoto | Japan | NRCT, P, CCS | July 2002–January 2011 | Low rectal cancer | Single | 44 | 22 | 22 | 0 | 0/0 | 1 | 1 |
| Gunka | Czech Republic | NRCT, P | January 2001–December 2006 | Nonmetastatic rectal cancer | Single | 145 | 75 | 70 | 6.7 | 23/20 | 65 (25–96) | 65 (25–96) |
| Jefferies | UK | NRCT, R | February 2007–June 2010 | Rectal cancer | Single | 41 | 16 | 25 | 12.5 | 7/14 | 23 (6–46) | 23 (6–46) |
| Kellokumpu | Finland | NRCT, P | January 1999–December 2006 | Rectal cancer | Single | 191 | 100 | 91 | 22 | 67/71 | 57.6 | 57.6 |
| Laurent | France | NRCT, R | 1990–2007 | Rectal cancer, below 6 cm from AV | Single | 175 | 110 | 65 | 22 | 103/55 | 53 (1–170) | 53 (1–170) |
| Li | China | NRCT, R | June 2004–June 2010 | Stage I‐III rectal cancer | Single | 657 | 381 | 276 | ND | ND | 51 (13–87) | 51 (13–87) |
| Mckay | Australia | NRCT, R | January 2001–December 2008 | Rectal cancer | Multiple | 545 | 157 | 388 | 8.3 | 77/137 | 1 | 1 |
| Seshadri | India | NRCT, P, CCS | January 2004–January 2010 | Mid and low rectal cancer, clinical stage cT2‐4 or cN1‐2 after nCRT | Single | 144 | 72 | 72 | 4 | 72/72 | 69.5 (1–138) | 69.5 (1–138) |
| Siani | Roma | NRCT, R | January 2004–January 2010 | Stage I‐III mid and low rectal cancer | Single | 60 | 30 | 30 | 3.3 | 30/30 | 38.3 | 37.9 |
| Kuo | Taiwan, China | NRCT, R | January 2006–October 2011 | Very low rectal cancer, within 5 cm from AV | Single | 58 | 28 | 30 | 0 | 28/27 | 1 | 1 |
| Lee | Korea | NRCT, R | June 2001–December 2008 | Stage I rectal cancer | Single | 160 | 80 | 80 | 1.25 | 0/0 | 51 (1–109) | 51 (1–109) |
| Lujan | Spain | NRCT, P | 2006–July 2010 | Rectal cancer | Single | 4405 | 1387 | 3018 | 17.37 | 806/1582 | 23.58 (11.77) | 21.98 (12.39) |
| Park | Korea | NRCT, R, CCS | January 2000–November 2008 | Rectal cancer, within 12 cm from AV | Single | 812 | 406 | 406 | 2 | 43/33 | 55.5 (35.4–77.4) | 55.5 (35.4–77.4) |
| Penninckx | Belgium | NRCT, R | January 2006–October 2011 | Mid or low rectal cancer | Multiple | 2660 | 764 | 1896 | 11.5 | 508/1393 | 36 | 36 |
| Yang | China | NRCT, R | May 2010–May 2012 | Low rectal cancer, within 10 cm from AV | Single | 177 | 87 | 90 | 1.1 | ND | 1 | 1 |
| Ferko | Czech Republic | NRCT, P | January 2010–December 2012 | Mid and lower rectal cancer, within 10 cm from AV | Single | 125 | 53 | 72 | 6.2 | 39/58 | ND | ND |
| Inada | Japan | NRCT, R, CCS | Aug 2004–November 2011 | Low rectal cancer | Single | 28 | 14 | 14 | 0 | ND | 1 | 1 |
| Inomata | Japan | NRCT, R | April 2002–March 2012 | Stage II/III rectal cancer | Single | 65 | 38 | 27 | ND | 5/1 | 1 | 1 |
| Keller | USA | NRCT, R | Aug 2005–May 2011 | Rectal cancer | Single | 81 | 62 | 19 | 14.5 | 40/16 | 25 (0.7–70.3) | 25 (0.7–70.3) |
| Kusano | Japan | NRCT, R | February 2002–November 2012 | Low rectal cancer after nCRT | Single | 33 | 19 | 14 | ND | 19/14 | 35 | 40 |
| Wang | China | NRCT, R | January 2010–January 2012 | Low rectal cancer | Single | 236 | 100 | 136 | 2 | 0/0 | 26 (17–38) | 26 (17–38) |
| Zhou | China | NRCT, R | January 2005– January 2008 | Rectal cancer, within 12 cm from AV | Single | 122 | 57 | 65 | 8.8 | 33/40 | 56.6 (10–84) | 56.6 (10–84) |
| Chi | China | NRCT, R | January 2006–Aug 2013 | Low rectal cancer | Single | 137 | 89 | 48 | 2.25 | 28/18 | 32.3 | 32.3 |
| Guo | China | NRCT, R, CCS | April 2007–December 2013 | Rectal cancer | Single | 382 | 191 | 191 | ND | ND | 42 | 46 |
| Huang | China | NRCT, CCS, R | January 2006–December 2013 | Rectal cancer | Single | 916 | 492 | 424 | 2.44 | ND | 55 | 55 |
| Kim | Korea | NRCT, R | January 2002–December 2011 | Rectal cancer | Single | 307 | 131 | 176 | ND | 14/26 | 40 (11–135) | 51 (8–142) |
| Li | China | NRCT, P | January 2003–December 2008 | Mid and low rectal cancer, within 10 cm from AV | Single | 281 | 129 | 152 | 6.2 | 48/55 | 74.8 (31.2) | 73.9 (31.7) |
| Nussbaum, | USA | NRCT, R, CCS | 2010–2011 | Rectal cancer | Multiple | 12,860 | 6430 | 6430 | ND | 1978/1961 | 1 | 1 |
| Wang, | China | NRCT, R | March 2009–December 2013 | Rectal cancer, within 10 cm from AV | Single | 212 | 106 | 106 | 2.83 | 26/26 | 16 (1–67) | 16 (1–67) |
| Zeng | China | NRCT, R | June 2007–June 2012 | Rectal cancer | Single | 294 | 112 | 182 | 6.3 | 39/61 | 29 (1–73) | 29 (1–74) |
| Zhou | China | NRCT, R | January 2000–December 2009 | Stage II‐III rectal cancer | Single | 406 | 152 | 254 | 4.6 | 13/16 | 63 (28–112) | 65 (32–118) |
| Allaix | Italy | NRCT, R | April 1994–Aug 2005 | Rectal cancer, within 12 cm from AV | Single | 307 | 153 | 154 | 10.5 | 78/85 | 79 (12–231) | 82.5 (12–242) |
| Chen ZX | China | NRCT, CCS, R | 2007–2013 | Rectal cancer, over 75 years old | Single | 74 | 37 | 37 | 0 | 0 | 1 | 1 |
| Chen WP | China | NRCT, R | June 2009–October 2015 | Mid‐low rectal cancer following nCRT | Single | 172 | 75 | 97 | 0 | 75/97 | 1 | 1 |
| Keskin | Turkey | NRCT, R | January 2005–December 2011 | Rectal cancer | Single | 587 | 437 | 150 | 7.78 | 286/81 | 48.5 (24.1) | 48.5 (24.1) |
| Kim | Korea | NRCT, R | July 2010–February 2015 | Rectal cancer | Single | 1581 | 486 | 1095 | 5.1 | 61/553 | 36 | 36 |
| Liu | China | NRCT, P | April 2009–April 2013 | Low or ultra‐low rectal cancer, diameter <2 cm, located at 3–5 cm from AV | Single | 112 | 67 | 45 | 0 | 0 | (26–40) | (24–38) |
| Nonaka | Japan | NRCT, R | January 2008– December 2014 | Advanced mid and low rectal cancer (pStage II‐III), within 10 cm from AV | Single | 78 | 40 | 38 | 0 | 14/13 | 32 (5–53) | 51 (4–66) |
| Odermatt | UK | NRCT, CCS, R | January 2003–June 2013 | Low rectal cancer | Single | 96 | 48 | 48 | 4.17 | 7/8 | 55 (24–72) | 55 (24–72) |
| De'Angelis | France | NRCT, CCS, R | January 2005–December 2015 | pT4 rectal cancer | Four | 104 | 52 | 52 | 21.2 | 35/36 | 34.37 (23.09) | 43.81 (32.54) |
| Matsuhashi | Japan | NRCT, CCS, R | July 2008–April 2013 | Low rectal cancer, ISR | Single | 25 | 19 | 6 | 10.5 | 0 | 54 | 54 |
| Silva‐Velazco | USA | NRCT, P | January 2010–December 2014 | Rectal cancer | Single | 422 | 118 | 304 | 15.4 | 58/124 | 1 | 1 |
| Wu | China | NRCT, R | October 2010–December 2015 | Rectal cancer | Single | 233 | 112 | 121 | 4.46 | 0 | 36 | 36 |
| Andersen | Denmark | NRCT, R | January 2007–December 2013 | Rectal cancer | Multiple | 6189 | 3099 | 3090 | ND | ND | 40.8 (28.8–60) | 54 (27.6–69.6) |
| Aydın | Turkey | NRCT, R | January 2006–January 016 | Rectal cancer | Single | 121 | 71 | 50 | ND | 19/4 | 55.2 | 56.75 |
| Chen | Taiwan, China | NRCT, CCS, R | 2008–2012 | Rectal cancer | Multiple | 108,436 | 5578 | 102,858 | ND | ND | 1 | 1 |
| Draeger | Germany | NRCT, R | January 2004–December 2013 | Rectal cancer | Single | 1507 | 428 | 1079 | ND | 186/398 | 85.2 | 85.2 |
| Garfinkle | Canada | NRCT, R | January 2009–March 2012 | Rectal cancer | 2 | 235 | 34 | 201 | 17 | 7/39 | 1 | 1 |
| Hida | Japan | NRCT, CCS, R | January 2010–2014 | Low rectal cancer, clinical stage II and III | 69 | 964 | 482 | 482 | 5.2 | 169/167 | 39.6 | 39.6 |
| Tayar | Brazil | NRCT, CCS, R | December 2008–December 2012 | Rectal cancer | Single | 100 | 50 | 50 | ND | 43/42 | 1 | 1 |
| Wu | China | NRCT, R | January 2009–December 2013 | Rectal cancer | Single | 891 | 277 | 614 | 1.3 | 57/42 | 65 (46–77) | 65 (46–77) |
| Chen | Taiwan, China | NRCT, R | July 2008–April 2018 | Low rectal cancer, within 7 cm from AV | Single | 87 | 64 | 23 | 1.6 | 31/8 | 37.5 (23.7) | 41.6 (29.1) |
| Davis | USA | NRCT, R | 2005–2016 | Rectal cancer | Multiple | 31,427 | 12,335 | 19,092 | ND | ND | 1 | 1 |
| Manchon‐Walsh | Spain | NRCT, CCS, R | 2011–2012 | Rectal cancer | 5 | 1359 | 842 | 517 | 13.2 | 524/310 | 60 | 60 |
| Schnitzbauer | Germany | NRCT, R | 2007–2016 | Rectal cancer | Multiple | 16,378 | 4540 | 11,838 | ND | 1724/4819 | 56.4 | 56.4 |
| Zhang XB | China | NRCT, CCS, R | January 2010–September 2014 | T4 rectal cancer | Single | 125 | 86 | 39 | 2.3 | 54/23 | 48 | 48 |
| Zhang ZZ | China | NRCT, R | January 2008–December 2011 | Rectal cancer | Single | 228 | 112 | 116 | ND | 35/38 | 67.93 (21.89) | 67.97 (22.19) |
| Zimmermann | Germany | NRCT, CCS, R | January 2006–March 2016 | Rectal cancer | 2 | 496 | 248 | 248 | 0 | 109/94 | 63 | 58 |
| Mar | Spain | NRCT, P | June 2010–December 2012 | Rectal cancer | Multiple | 601 | 400 | 201 | ND | 201/113 | 24 | 24 |
| Reference | Selections | Comparability | Outcome assessment | Score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
| Schwandner, 1999 | * | * | * | * | ‐ | * | * | * | * | 8 |
| Leung | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Hartley | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Anthuber | * | * | * | * | ‐ | ‐ | * | ‐ | * | 6 |
| Feliciotti | * | * | * | * | * | ‐ | * | * | * | 8 |
| Wu | * | * | * | * | * | * | * | ‐ | ‐ | 7 |
| Bretagnol | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Breukink | * | * | * | * | ‐ | ‐ | * | ‐ | * | 6 |
| Morino | * | * | * | * | * | ‐ | * | * | * | 8 |
| Sahakitrungruang | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Law | * | * | * | * | * | ‐ | * | * | * | 8 |
| Wong | * | * | * | * | * | * | * | * | * | 9 |
| Lelong | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Staudacher | * | * | * | * | * | * | * | * | * | 9 |
| Veenhof | * | * | * | * | ‐ | * | * | * | * | 8 |
| Ströhlein | * | * | * | * | ‐ | * | * | * | * | 8 |
| Ding | * | * | * | * | * | ‐ | * | ‐ | * | 7 |
| González | * | * | * | * | ‐ | ‐ | * | ‐ | * | 6 |
| Gouvas | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Khaikin | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Kim | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Koulas | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Laurent | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Law | * | * | * | * | * | ‐ | * | * | * | 8 |
| Biondo | * | * | * | * | * | * | * | ‐ | ‐ | 7 |
| Denoya | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Feng | * | * | * | * | ‐ | * | * | * | * | 8 |
| Fujimoto | * | * | * | * | ‐ | * | * | ‐ | * | 7 |
| Baik | * | * | * | * | * | * | * | * | * | 9 |
| da Luz Moreira | * | * | * | * | * | * | * | ‐ | ‐ | 7 |
| Greenblatt | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| June | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Li | * | * | * | * | * | * | * | * | * | 9 |
| Park | * | * | * | * | * | * | * | * | * | 9 |
| Yamamoto | * | * | * | * | * | * | * | ‐ | ‐ | 7 |
| Gunka | * | * | * | * | * | * | * | * | * | 9 |
| Jefferies | * | * | * | * | * | ‐ | * | * | * | 8 |
| Kellokumpu | * | * | * | * | * | * | * | * | * | 9 |
| Laurent | * | * | * | * | * | * | * | * | * | 9 |
| Li | * | * | * | * | * | ‐ | * | * | * | 8 |
| Mckay | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Seshadri | * | * | * | * | * | * | * | * | * | 9 |
| Siani | * | * | * | * | ‐ | * | * | * | * | 8 |
| Kuo | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Lee | * | * | * | * | * | * | * | * | * | 9 |
| Lujan | * | * | * | * | ‐ | ‐ | * | ‐ | * | 6 |
| Park | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Penninckx | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Yang | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Ferko | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Inada | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Inomata | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Keller | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Kusano | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Wang | * | * | * | * | * | * | * | * | * | 9 |
| Zhou | * | * | * | * | * | * | * | * | * | 9 |
| Chi | * | * | * | * | * | * | * | * | * | 9 |
| Guo | * | * | * | * | * | ‐ | * | * | * | 8 |
| Huang | * | * | * | * | * | ‐ | * | * | * | 8 |
| Kim | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Li | * | * | * | * | * | * | * | * | * | 9 |
| Nussbaum | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Wang | * | * | * | * | * | * | * | ‐ | * | 8 |
| Zeng | * | * | * | * | * | * | * | * | * | 9 |
| Zhou | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Allaix | * | * | * | * | ‐ | * | * | * | * | 8 |
| Chen ZX | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Chen WP | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Keskin | * | * | * | * | * | ‐ | * | * | * | 8 |
| Kim | * | * | * | * | * | ‐ | * | * | * | 8 |
| Liu | * | * | * | * | ‐ | * | * | ‐ | ‐ | 6 |
| Nonaka | * | * | * | * | ‐ | * | * | * | * | 8 |
| Odermatt | * | * | * | * | * | * | * | * | * | 9 |
| De'Angelis | * | * | * | * | * | * | * | * | * | 9 |
| Matsuhashi | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Silva‐Velazco | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Wu | * | * | * | * | * | * | * | * | * | 9 |
| Andersen | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Aydın | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Chen | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Draeger | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Garfinkle | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Hida | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Tayar | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Wu | * | * | * | * | * | ‐ | * | * | * | 8 |
| Chen | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Davis | * | * | * | * | * | ‐ | * | ‐ | ‐ | 6 |
| Manchon‐Walsh | * | * | * | * | * | ‐ | * | * | * | 8 |
| Schnitzbauer | * | * | * | * | ‐ | ‐ | * | * | * | 7 |
| Zhang XB | * | * | * | * | * | ‐ | * | * | * | 8 |
| Zhang ZZ | * | * | * | * | * | ‐ | * | * | ‐ | 7 |
| Zimmermann | * | * | * | * | * | ‐ | * | * | * | 8 |
| Mar | * | ‐ | * | * | * | ‐ | * | * | * | 7 |
| Outcome variables | Studies ( | Patients ( | Analysis model | Total | RCT subgroup | NRCT subgroup | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MD/OR [95%CI] |
|
| MD/OR [95%CI] |
|
| MD/OR [95%CI] |
|
| ||||
| Intraoperative outcomes | ||||||||||||
| Operation time | 82 (17/65) | 24,106/37127 | M | 25.67 [21.02, 30.32] | 97 | <0.0001 | 36.31 [26.49, 46.14] | 97 | <0.0001 | 22.45 [17.10, 27.79] | 97 | <0.0001 |
| Blood loss | 66 (16/50) | 7604/797 | M | −131.42 [−153.61, −109.23] | 99 | <0.0001 | −110.85 [−147.23, −74.47] | 99 | <0.0001 | −138.53 [−166.66, −110.40] | 100 | <0.0001 |
| Incision length | 12 (7/5) | 1945/2244 | M | −12.82 [−12.85, −12.79] | 100 | <0.0001 | −11.77 [−11.87, −11.68] | 100 | <0.0001 | −12.94 [−12.97, −12.91] | 99 | <0.0001 |
| Pathological outcomes | ||||||||||||
| Harvested lymph nodes | 84 (16/68) | 18,459/22609 | M | −0.44 [−0.78, 0.10] | 95 | 0.01 | 0.05 [−0.59, 0.69] | 87 | 0.87 | −0.60 [−1.01, −0.19] | 96 | 0.004 |
| CMR (+) | 43 (10/33) | 14,126/16844 | F | 0.79 [0.72, 0.85] | 40 | <0.0001 | 1.21 [0.91, 1.59] | 0 | 0.19 | 0.76 [0.69, 0.82] | 41 | <0.0001 |
| DMR (+) | 18 (2/16) | 9919/10211 | F | 0.75 [0.66, 0.85] | 0 | <0.0001 | 1.13 [0.35, 3.66] | 0 | 0.84 | 0.74 [0.65, 0.85] | 6 | <0.0001 |
| TME completeness | 20 (6/14) | 4891/7295 | M | 1.02 [0.99, 1.05] | 60 | 0.18 | 0.96 [0.91, 1.01] | 17 | 0.10 | 1.04 [1.01, 1.07] | 58 | 0.02 |
| Postoperative outcomes | ||||||||||||
| First bowel movement | 49 (15/34) | 6593/6878 | M | −0.89 [−1.06, −0.73] | 98 | <0.0001 | −0.83 [−1.06, −0.61] | 98 | <0.0001 | −0.90 [−1.08, −0.73] | 96 | <0.0001 |
| Postoperative analgesic need | 11 (5/6) | 996/1029 | M | −0.88 [−1.38, −0.38] | 97 | 0.0006 | −0.60 [−1.21, 0.02] | 96 | 0.06 | −1.11 [−2.28, 0.06] | 97 | 0.06 |
| Days of ambulation | 12 (6/6) | 1415/1471 | M | −0.89 [−1.09, −0.69] | 72 | <0.0001 | −0.69 [−0.87, −0.51] | 21 | <0.0001 | −1.03 [−1.34, −0.71] | 81 | <0.0001 |
| Length of hospital stay | 92 (16/76) | 38,446/149664 | M | −0.62 [−0.77, −0.47] | 99 | <0.0001 | −0.63 [−0.94, −0.31] | 96 | <0.0001 | −0.62 [−0.78, −0.45] | 99 | <0.0001 |
| Postoperative complications | 86 (16/70) | 19,412/124070 | F | 0.83 [0.81, 0.85] | 7 | <0.0001 | 0.92 [0.84, 1.00] | 14 | 0.06 | 0.82 [0.80, 0.84] | 0 | <0.0001 |
| Hemorrhage | 47 (9/38) | 13,221/116441 | F | 0.74 [0.62, 0.89] | 0 | 0.001 | 0.68 [0.40, 1.17] | 3 | 0.16 | 0.75 [0.62, 0.91] | 0 | 0.003 |
| Wound infection | 75 (14/61) | 26,866/39726 | F | 0.50 [0.47, 0.54] | 13 | <0.00001 | 0.59 [0.46, 0.77] | 28 | 0.0001 | 0.50 [0.47, 0.53] | 7 | <0.00001 |
| Ileus | 70 (15/55) | 15,826/115502 | F | 0.92 [0.87, 0.96] | 0 | 0.0008 | 0.71 [0.53, 0.94] | 0 | 0.02 | 0.92 [0.88, 0.97] | 0 | 0.003 |
| Anastomotic leak | 76 (16/60) | 13,376/16968 | F | 1.01 [0.93, 1.10] | 0 | 0.77 | 0.95 [0.73, 1.23] | 0 | 0.68 | 1.02 [0.93, 1.12] | 0 | 0.65 |
| Abscess | 46 (9/37) | 20,199/32131 | F | 0.94 [0.87, 1.02] | 0 | 0.12 | 1.10 [0.74, 1.63] | 0 | 0.64 | 0.94 [0.87, 1.01] | 0 | 0.09 |
| Reintervention within 30 days | 36 (9/27) | 7733/13167 | F | 0.96 [0.86, 1.07] | 0 | 0.44 | 1.01 [0.80, 1.27] | 0 | 0.96 | 0.94 [0.83, 1.07] | 0 | 0.37 |
| Mortality within 30 days | 48 (8/40) | 34,690/145359 | F | 0.66 [0.59, 0.75] | 0 | <0.0001 | 0.79 [0.44, 1.43] | 0 | 0.44 | 0.66 [0.58, 0.75] | 0 | <0.0001 |
| Survival outcomes | ||||||||||||
| 3‐year LR | 33 (7/26) | 5511/5828 | F | 0.81 [0.69, 0.95] | 0 | 0.008 | 1.04 [0.74, 1.46] | 0 | 0.83 | 0.76 [0.64, 0.90] | 0 | 0.002 |
| 3‐year DR | 21 (5/16) | 3323/3671 | F | 0.91 [0.80, 1.02] | 0 | 0.11 | 1.01 [0.82, 1.26] | 0 | 0.90 | 0.86 [0.75, 1.00] | 9 | 0.05 |
| 3‐year DFS | 26 (6/20) | 3947/4228 | F | 1.03 [1.01, 1.06] | 22 | 0.01 | 1.04 [0.99, 1.09] | 0 | 0.17 | 1.03 [1.00, 1.06] | 32 | 0.03 |
| 3‐year OS | 32 (7/25) | 7022/7989 | F | 1.03 [1.01, 1.05] | 35 | 0.007 | 1.01 [0.98, 1.05] | 10 | 0.54 | 1.03 [1.01,1.06] | 40 | 0.006 |
| 5‐year LR | 23 (4/19) | 3553/4131 | F | 0.66 [0.57, 0.75] | 41 | <0.0001 | 0.99 [0.53, 1.83] | 0 | 0.97 | 0.64 [0.55,0.74] | 44 | <0.0001 |
| 5‐year DR | 19 (5/14) | 2444/2175 | F | 0.89 [0.78, 1.01] | 8 | 0.07 | 0.87 [0.68, 1.11] | 24 | 0.26 | 0.89 [0.77, 1.04] | 8 | 0.16 |
| 5‐year DFS | 22 (5/17) | 7893/15078 | M | 1.06 [1.02, 1.10] | 54 | 0.002 | 1.02 [0.95, 1.09] | 0 | 0.66 | 1.07 [1.02, 1.11] | 62 | 0.002 |
| 5‐year OS | 29 (5/24) | 10,069/17046 | M | 1.05 [1.02, 1.09] | 69 | 0.001 | 1.01 [0.93, 1.10] | 11 | 0.75 | 1.06 [1.02, 1.10] | 73 | 0.001 |
- —Beijing Shijitan Hospital Professionals Training Program (NO.2023LJRCDL)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHistorical Studies of Medieval Iberia
INTRODUCTION
1
Colorectal cancer (CRC) is the third most common cause of cancer death in the United States with an incidence rate of 35.3 and mortality rate of 13.2 per 100,000 population. Approximately one‐third of these cases are rectal cancers.1, 2 The mainstay treatment for rectal cancer remains surgical resection. Considered as a major landmark, laparoscopic colectomy was first performed on 20 patients by Jacobs et al.3 Over the next 30 years, the theory and technique of laparoscopic surgery in the management of rectal cancer have been standardized and improved enormously. Since 2006, the National Comprehensive Cancer Network (NCCN) clinical practice guidelines had recommended laparoscopic‐assisted colectomy to be the priority option for the qualified cases. However, the application of laparoscopy in rectal cancer is still controversial.
Laparoscopic surgery has unbeatable advantages in terms of postoperative recovery. The major controversies over laparoscopy versus open proctectomy are on the oncological outcomes and long‐term survival. The early researches showed doubts on the high incidence of postoperative and peritoneal implantation metastasis after laparoscopic surgery.4 On the contrary, accumulating clinical trials had proved the safety and efficacy of laparoscopic proctectomy compared with open surgery. However, there had been no comprehensive assessment and comparison covering all the aspects of the two procedures in the treatment of rectal cancer, especially the pathological outcomes and long‐term survival. Based on a comprehensively review of literature, we started this largest‐to‐date meta‐analysis to make an overall comparison between the two surgical methods.
METHODS AND METHODS
2
The protocol for this meta‐analysis was available in PROSPERO (CRD42020211718).
Literature search
2.1
We searched literatures involved with randomized controlled trials (RCTs) or nonrandomized controlled trials (NRCTs) on the following online databases: MEDLINE (through PubMed), Cochrane Library and Embase Databases, covering a period from January 1990 to March 2020. The search string was as follows: (rectal cancer or rectal carcinoma or rectal neoplasms) and (treatment or therapy or access or approach or management) and (laparoscopy or laparoscopic surgery) and (open surgery or laparotomy). Manual retrieval of relevant literature reference was available to expand the search and to ensure that no research was omitted. Only full‐text English‐language trials that met the selection criteria were retrieved and reviewed.
Inclusion criteria
2.2
The trials were included based on the following inclusion criteria: (1) RCTs or NRCTs conducted in the period from January 1990 to March 2020; (2) the population of interest were adults diagnosed with rectal cancer by pathology of histology and underwent surgical treatment by means of laparoscopic proctectomy or open surgery; the surgical procedure of protectomy including anterior resection, abdominoperineal resection and intersphincteric resection was made according to the tumor localization above the anal verge, extent of tumor invasion and histologic type; (3) the selected literature must include two sets of data comparison of laparoscopic surgery group and open surgery group in the following aspects: surgical process, pathological results, postoperative recovery and short‐term or long‐term outcomes; and (4) literatures were full‐text papers and published in English.
Exclusion criteria
2.3
The trials were excluded based on the following exclusion criteria: (1) articles were not written in English, or unable to provide full text; (2) review, editorials and commentary articles; (3) literatures were published by the same researcher or research institutes; and (4) data provided by the paper were not clear and valid or could not be obtained via calculation.
Quality assessment
2.4
The quality of trials was assessed independently by two authors (LI and XU) using two methods. All RCTs were assessed by the Cochrane risk of bias criteria,5 whereas the NRCTs were assessed by the Newcastle‐Ottawa Scale (NOS),6 as recommended in the Cochrane Handbook. A score above 6 indicated high quality; otherwise, a lower score indicated poor quality. If controversy existed between the two independent evaluations, all of the authors participated in a discussion to resolve the issue.
Data extraction
2.5
All the information about the participants' characteristics, surgical process, pathological results, postoperative recovery and complications, and short‐term or long‐term outcomes from included studies were extracted independently by three authors (MA, YU, and ZHU). Consensus was reaching after discussion by the three authors or the intervene of the senior authors (DING and GAO).
Statistical analysis
2.6
This meta‐analysis was performed using Review Manager (RevMan‐Version 5.3.). We designed subgroup analysis based on the RCTs and NRCTs. Continuous variables were pooled using the mean difference (MD) with a 95% confidence interval (CI). Discontinuous variables were pooled using the risk ratios (RRs) with a 95% CI. If studies reported the median, range and size of the trial, the means and standard deviations were calculated according to Hozo et al.7 If studies only reported the medians and range, this parameter would be excluded. According to the practice recommendation of the Cochrane Handbook, trials with zero events in both the intervention and the control groups were not included in the meta‐analysis.
All tests were two‐tailed, and p < 0.05 was considered statistically significant. The I ^2^ statistic was used to investigate the heterogeneity among the studies. I ^2^ < 50% indicated a small inconsistency and the fixed effects model was used to pool the data. I ^2^ > 50% indicated a large inconsistency and the random effects model was used to pool the data. Sensitivity analysis was performed by excluding low‐quality studies, trials recruiting participants with particular conditions, or trials with characteristics different from the others.
RESULTS
3
Study Selection
3.1
After the combined search, 1564 articles were identified. Titles and abstracts of these records were screened for inclusion. 1323 articles were rejected and the remaining 241 articles then underwent full‐text evaluation. Finally, 113 articles including 20 RCTs and 93 NRCTs met the inclusion criteria. The PRISMA flowchart for study inclusion and exclusion process was showed in Figure 1.
Flow diagram of literature search and selection process.
Characteristics and methodological quality of eligible studies
3.2
The characteristics of the 113 studies were summarized in Table 1. It included 20 RCTs and 93 NRCTs for a total of 216,615 rectal cancer patients. Of them, 48,888 patients received laparoscopic proctectomy and 167,727 patients underwent open surgery. In the laparoscopic surgery group, patients required a conversion from laparoscopy to open surgery. The conversion cases remained in the laparoscopic surgery group according to the principle of intention‐to‐treat.
Quality assessment of the included articles according to the Cochrane Collaboration's tool for assessing risk of bias for RCTs and to the NOS for prospective NRCTs were shown in Table 2 and Figure 2.
The risk of bias assessment of included RCT studies.
Meta‐analysis results
3.3
The specific data of the results of the meta‐analysis comparing laparoscopic versus open surgery for rectal cancer in the aspects of intraoperative, pathological, postoperative and survival outcomes were listed in Table 3.
Intraoperative outcomes
3.4
Operation time was reported in 17 RCTs and 65 NRCTs. The weighted mean operation time was significantly increased in the laparoscopic group than open surgery group (248.37 vs. 221.96 min, MD = 25.67, 95% CI: 21.02–30.32, I ^2^ = 97%, p < 0.0001) (Figure S1).
Blood loss was reported in 16 RCTs and 50 NRCTs. Significant less blood loss was found in laparoscopic surgery compared with open surgery (151.30 vs. 276.60 mL, MD = −131.42, 95% CI: −153.61 to −109.23, I ^2^ = 99%, p < 0.0001) (Figure S2).
Incision length was reported in 7 RCTs and 5 NRCTs. Significant shorter surgical incision was found in laparoscopic surgery compared with open surgery (5.36 vs. 17.05 cm, MD = −12.82, 95% CI: −12.85 to −12.79, I ^2^ = 100%, p < 0.0001) (Figure S3).
Pathological outcomes
3.5
The number of harvested lymph nodes were reported in 16 RCTs and 68 NRCTs. The weighted mean lymph node retrieved in laparoscopic surgery was significant less than open surgery (14.67 vs. 14.86, MD = −0.44, 95% CI: −0.78 to −0.10, I ^2^ = 95%, p = 0.01). However, the subgroup meta‐analysis showed no significant difference was found in RCT subgroup (MD = 0.05, 95% CI: −0.59 to 0.69, I ^2^ = 87%, p = 0.87) (Figure S4).
CMR positive rate was reported in 10 RCTs and 33 NRCTs. The weighted mean CMR positive rate was significantly reduced in laparoscopic surgery compared with open surgery (6.24% vs. 8.88%, RR = 0.79, 95% CI: 0.72 to 0.85, I ^2^ = 40%, p < 0.0001), but there was no significant difference in RCT subgroup (RR = 1.21, 95% CI: 0.91–1.59, I ^2^ = 0%, p = 0.19) (Figure S5).
DMR positive rate was reported in 2 RCTs and 16 NRCTs. The weighted mean DMR positive rate was significantly reduced in laparoscopic surgery compared with open surgery (3.84% vs. 4.99%, RR = 0.75, 95% CI: 0.66–0.85, I ^2^ = 0%, p < 0.0001), but there was no significant difference in RCT subgroup (RR = 1.13, 95% CI: 0.35–3.66, I ^2^ = 0%, p = 0.84) (Figure S6).
The macroscopic quality of total mesorectal excision (TME) specimen was reported in 6 RCTs and 14 NRCTs. No significant difference of TME completeness was found in laparoscopic surgery compared with open surgery (79.41% vs. 76.07%, RR = 1.02, 95% CI: 0.99–1.05, I ^2^ = 60%, p = 0.18) (Figure S7).
Postoperative outcomes
3.6
Bowel movement recovery was reported in 15 RCTs and 34 NRCTs. The weighted mean time before the first bowel movement or passing the first flatus was significantly shorter in laparoscopic surgery compared with open surgery (2.66 vs. 3.46 days, MD = −0.89, 95% CI: −1.06 to −0.73, I ^2^ = 98%, p < 0.0001) (Figure S8).
The days of postoperative analgesic need were reported in 5 RCTs and 6 NRCTs. The weighted mean time of postoperative analgesic need was significantly decreased in laparoscopic surgery compared with open surgery (3.063 vs. 3.61 days, MD = −0.88, 95% CI: −1.38 to −0.38, I ^2^ = 97%, p = 0.0006) (Figure S9).
The days of ambulation were reported in 6 RCTs and 6 NRCTs. Significant less days of ambulation was found in laparoscopic surgery compared with open surgery (3.28 vs. 4.49 days, MD = −0.89, 95% CI: −1.09 to −0.69, I ^2^ = 72%, p < 0.0001) (Figure S10).
The length of hospital stay was reported in 16 RCTs and 76 NRCTs. The weighted mean time of hospital stay was significantly shorter in laparoscopic surgery compared with open surgery (7.33 vs.7.44 days, MD = −0.62, 95% CI: −0.77 to −0.47, I ^2^ = 99%, p < 0.0001) (Figure S11).
Postoperative complications were reported in 16 RCTs and 70 NRCTs. The weighted mean incidence of overall postoperative complications was significantly decreased in laparoscopic surgery compared with open surgery (28.27% vs. 35.27%, RR = 0.83, 95% CI: 0.81–0.85, I ^2^ = 7%, p < 0.0001), but no significant difference was found in the RCT subgroup (RR = 0.92, 95% CI: 0.84–1.00, I ^2^ = 14%, p = 0.06) (Figure S12). Then we focused on the comparison of five major postoperative complications. The total meta‐analysis revealed significant low rate of hemorrhage (1.25% vs. 5.02%, RR = 0.74, 95% CI: 0.62–0.89, I ^2^ = 0%, p = 0.001) (Figure S13), wound infection (4.84% vs. 10.02%, RR = 0.50, 95% CI: 0.47–0.54, I ^2^ = 13%, p < 0.00001) (Figure S14) and ileus (9.19% vs. 16.81%, RR = 0.92, 95% CI: 0.87–0.96, I ^2^ = 0%, p = 0.0008) (Figure S15) in laparoscopic surgery compared with open surgery. No significant difference of incidence rate of anastomotic leak (7.19% vs. 6.70%, RR = 1.01, 95% CI: 0.93–1.10, I ^2^ = 0%, p = 0.77) (Figure S16) and intra‐abdominal, pelvic or retroperitoneal abscess after surgery (5.03% vs. 5.52%, RR = 0.94, 95% CI: 0.87–1.02, I ^2^ = 0%, p = 0.12) (Figure S17) were found between the two groups.
Reintervention within 30 days after surgery was reported in 9 RCTs and 27 NRCTs. No significant difference of reintervention rate was found in laparoscopic surgery compared with open surgery (7.02% vs. 5.54%, RR = 0.96, 95% CI: 0.86–1.07, I ^2^ = 0%, p = 0.44) (Figure S18).
Mortality within 30 days was reported in 8 RCTs and 40 NRCTs. Significant decreased mortality was significantly decreased in laparoscopic surgery compared with open surgery (0.98% vs. 1.29%, RR = 0.66, 95% CI: 0.59–0.75, I ^2^ = 0%, p < 0.0001), but no significant difference was found in the RCT subgroup (RR = 0.79, 95% CI: 0.44–1.43, I ^2^ = 0%, p = 0.44) (Figure S19).
Survival outcomes
3.7
Thirty‐three studies reported 3‐year local recurrence (LR) and 23 studies reported 5‐year LR. The laparoscopic surgery group showed significantly decreased 3‐year LR (5.12% vs. 6.01%, RR = 0.81, 95% CI: 0.69–0.95, I ^2^ = 0%, p = 0.008) (Figure S20) and 5‐year LR (7.46% vs. 13.73%, RR = 0.66, 95% CI: 0.57–0.75, I ^2^ = 41%, p < 0.0001) (Figure S21) compared with open surgery group. However, there were no significant differences in the RCT subgroup.
Twenty‐one studies reported 3‐year distant recurrence (DR) and 19 studies reported 5‐year DR. There were no significant differences of 3‐year DR (13.36% vs. 14.79%, RR = 0.91, 95% CI: 0.80–1.02, I ^2^ = 0%, p = 0.11) (Figure S22) or 5‐year DR (16.24% vs. 17.01%, RR = 0.89, 95% CI: 0.78–1.01, I ^2^ = 8%, p = 0.07) (Figure S23) between the two groups.
Twenty‐six studies reported 3‐year disease free survival (DFS) and 22 studies reported 5‐year DFS. The laparoscopic surgery group showed significantly increased 3‐year DFS (73.57% vs. 74.55%, RR = 1.03, 95% CI: 1.01–1.06, I ^2^ = 22%, p = 0.01) (Figure S24) and 5‐year DFS (78.41% vs. 73.28%, RR = 1.06, 95% CI: 1.02–1.10, I ^2^ = 54%, p = 0.002) (Figure S25) compared with open surgery group. However, there were no significant differences in the RCT subgroup.
Thirty‐two studies reported 3‐year overall survival (OS) and 29 studies reported 5‐year OS. The laparoscopic surgery group showed significantly increased 3‐year OS (84.88% vs. 82.78%, RR = 1.03, 95% CI: 1.01–1.05, I ^2^ = 35%, p = 0.007) (Figure S26) and 5‐year OS (79.09% vs. 75.52%, RR = 1.05, 95% CI: 1.02–1.09, I ^2^ = 69%, p = 0.001) (Figure S27) compared with open surgery group. However, there were no significant differences in the RCT subgroup.
Only three studies reported 10‐year LR and DR, four studies reported 10‐year DFS and OS. No significant differences were showed based on these 10‐year data of the two groups (data not shown).
DISCUSSION
4
Since laparoscopic surgery were applied to the resection of rectal cancer, numerous studies had been carried out to evaluate the surgical and oncological outcomes of this approach compared with traditional open surgery. Meanwhile, countless meta‐analyses had drawn many conclusions based on the analysis of different types of trials. However, there had been no comprehensive assessment and comparison covering all the aspects of the two procedures in the treatment of rectal cancer, especially the pathological outcomes and long‐term survival. We started this largest‐to‐date meta‐analysis including 113 studies spanning over 30 years to fill the vacuum. In order to include as many patients as possible, not only RCTs but also numerous NRCTs from different medical centers were incorporated into our research, and conditions of inclusion criteria (different locations or stages of rectal cancer, with or without nCRT, different operation styles and studies with small sample size) was relaxed to a certain extent. The 93 NRCTs showed low risk of bias which left these reports convincing. Based on the overall investigation, the genuine effectiveness of laparoscopic proctectomy could be assessed accurately.
The surgical approach for upper rectal cancer was equivalent to the sigmoid cancer, while the standard treatment for mid and low rectal cancer was TME. A successful resection of rectal cancer should meet the conditions of complete TME, a clear circumferential margin (CRM, ≥1 mm) and a clear distal resection margin (DRM, ≥1 mm).29 The standardization of TME improved the prognosis of rectal cancer by reducing the positive margin and local recurrence rates.128 This concept demands the sharp separation of the visceral fascia from the parietal plane. The resected specimen was the whole rectal tumor with an intact coverage including the main lymphatic drainage.129 It was evident that the magnified, illuminated images and pneumoperitoneum provided by laparoscopy facilitated the operation in the narrow pelvic space. In that case, a high‐quality of resected specimen might be more easily to obtain. The results of this meta‐analysis indicated that the 3‐year LR and 5‐year LR were both significantly decreased after the laparoscopic surgery, and eventually lead to longer DFS and OS. Part of that improvement might be attributable to the radical resection of the tumor and mesorectum under direct vision created by laparoscopy. Although there was no significant difference of TME completeness and number of harvested lymph nodes found in laparoscopic surgery compared with open surgery, the positive rate of CMR and DMR were both reduced in the laparoscopy group. These results might contribute to the decreased LR. NCCN guidelines mentioned that some studies had shown that laparoscopy is associated with higher rates of CMR and incomplete TME, which was not supported by our large‐scale meta‐analysis. Moreover, there were no significant differences of 3‐year DR and 5‐year DR between the two groups. It suggested that laparoscopy might reduce the local recurrence without promoting distant metastasis. It should be noted that no significant difference of these survival indexes was found in the RCT subgroup.
The ultimate goal of treatment for cancer was not only an optimal oncological outcome, but also rapid recovery and improved quality of life. Our study revealed that patients could benefit from laparoscopic surgery in the postoperative recovery, including earlier return of bowel function, improved cosmesis and reduced pain owing to small incisions, earlier ambulation, shorter hospital stay and less complications. The total incidence of postoperative complications, morbidity of major complications and mortality within 30 days were all significantly decreased in the laparoscopy group without increased risk of reintervention. The fast recovery after surgery enabled patients to initiate following adjuvant therapy in a shorter period, which was a favorable factor contributing to the improvement of the prognosis.
The pneumoperitoneum created by laparoscopic surgery effectively expanded the activity of abdomen. However, the expansion of pelvic cavity was limited. Accomplishment of anastomosis under laparoscopy without collateral damage required precise manipulation of the surgeons. Only the well‐trained doctors were qualified to perform laparoscopic rectal resection which could provide the equivalent oncologic outcomes and faster postoperative recovery. The COREAN trial was competed by seven highly skilled laparoscopic specialists, it suggested that better short‐term outcome could be achieved in expert hands.20 Several researches recommended effective self‐taught learning curve was about 50–80 laparoscopic rectal resections.130 The rates of conversion to laparotomy, operation time, blood loss and complications were all decreased in the cases performed by senior surgeons. Moreover, the natural orifice specimen extraction surgery and robotic‐assisted laparoscopic surgery have been applied in the surgical treatment of cancer as technology evolved. These kinds of minimal invasive surgery demanding special surgical skills could further decrease the operative trauma and promote postoperative recovery. In that case, the role of surgeons in the surgery and the outcomes of patients was crucial. The experience of surgeons should be taken into consideration in the further strictly controlled trials. The laparoscopic surgery did require longer operative time, but time gap between the two approaches could be closing as the well‐trained surgeons have perfected their surgical techniques.
Drawbacks of laparoscopic protectomy will appear when it comes to specific cases, such as super obese patients or advanced tumor with extensive invasion. The difficulty of laparoscopy will lead to the conversion into open surgery. The range of conversion rate reported in the literatures mentioned in this paper was from 0% to 23.2%, and the average rate was 7.73%. The reasons for conversion might be as follows: too large tumors, low‐located T4 tumors, previously irradiated pelvis, collateral damages of surgical operation and so on. The oncological outcomes of cases converted to open surgery is a controversial issue. Some studies showed similar outcomes, but others revealed worsen short‐term outcomes,131 higher rates of LR and reduced cumulative DFS.132 Most conversion in laparoscopic surgery are actually avoidable with adequate preoperative evaluation based on diagnostic imaging tests and a well‐trained laparoscopic surgical team. The extended laparoscopic instruments also facilitate the operation on the obese patients.
T4 tumor is always the focus of controversy. It was identified as those that invade into other organs and structures and/or perforate the visceral peritoneum. All the guidelines suggest T4 rectal cancer as a contraindication for laparoscopic surgery, because the locally advanced tumor have a high risk of CMR or need en bloc resection of the adjacent infiltrated organs which might increase the convention rates and collateral increasing morbidity. Some studies have assessed the pathologic and oncologic results and suggested that laparoscopic surgery was feasible for T4 colorectal cancer.108, 124 In this study, laparoscopic resection for all the stages of rectal cancer were merged and generally compared with open surgery. In that case, the analysis to some foci of controversy was ignored, such as T4 tumor, resection of primary tumor following nCRT and so on. Further stratified and grouped comparisons were urgently needed to compare the effect of these two surgical approaches in the specific population of rectal patients. Moreover, there were many more aspects in the recovery and prognosis of patients received surgical management deserves to be focused on and compared between the laparoscopy and open surgery, including the gender differences based on different anatomical structure, urinary and sexual dysfunction, incisional hernia, hospitalized cost and postoperative immunological changes. The robot‐assisted laparoscopy has become emerging trend in the treatment of rectal cancer. The surgical outcomes of robotic surgery should also be compared with traditional laparoscopy and open surgery separately.
This article incorporated a large number of NRCTs which lead to a certain degree of bias in case selection and comparability. But they had already been accessed as high quality. Moreover, some NRCTs might have a preference in selection of population for specific purpose, such as elderly patients, T4 tumors, patients received nCRT and so on. These results were all unique and meaningful in the interpretation of the effect of laparoscopic proctectomy. As it should be, more large‐scale RCTs and observational studies with stratified method, multivariable risk adjustment or propensity score analysis were urgently needed to evaluate the surgical outcomes of laparoscopy.
CONCLUSIONS
5
Based on the meta‐analysis of both RCTs and NRCTs, laparoscopic proctectomy was non‐inferior to open surgery in terms of pathological results, postoperative recovery and long‐term survival in the treatment of rectal cancer. It should be recommended as the priority option for the eligible patients in the surgical treatment of rectal cancer.
AUTHOR CONTRIBUTIONS
Ling Ma: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); investigation (equal); methodology (equal); project administration (equal); resources (equal); software (equal); supervision (equal); validation (equal); visualization (equal); writing – original draft (equal); writing – review and editing (equal). Hai‐jiao Yu: Data curation (equal); writing – original draft (equal); writing – review and editing (equal). Yu‐bing Zhu: Data curation (equal); writing – original draft (equal); writing – review and editing (equal). Wen‐xia Li: Formal analysis (equal); software (equal); writing – original draft (equal); writing – review and editing (equal). Kai‐yu Xu: Formal analysis (equal). Ai‐min Zhao: Project administration (equal); resources (equal). Lei Ding: Conceptualization (equal); methodology (equal); supervision (equal); validation (equal); visualization (equal); writing – review and editing (equal). Hong Gao: Conceptualization (equal); methodology (equal); supervision (equal); validation (equal); visualization (equal); writing – review and editing (equal).
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
All authors declare no conflicts of interest.
PRECIS
Laparoscopy is non‐inferior to open surgery for rectal cancer in intraoperative, pathological, postoperative and long‐term outcomes. Laparoscopic surgery provides short‐term advantages, including faster recovery and less complications.
Supporting information
Figure S1.
Data S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL , Giaquinto AN , Jemal A . Caner statistics, 2024. CA Cancer J Clin. 2024;74:12‐49.38230766 10.3322/caac.21820 · doi ↗ · pubmed ↗
- 2Siegel RL , Miller KD , Sauer AG , et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70:145‐164.32133645 10.3322/caac.21601 · doi ↗ · pubmed ↗
- 3Jacobs M , Verdeja JC , Goldstein HS . Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc. 1991;1:144‐150.1688289 · pubmed ↗
- 4Wexner SD , Cohen SM . Port site metastases after laparoscopic colorectal surgery for cure of malignancy. Br J Surg. 1995;82:295‐298.7795990 10.1002/bjs.1800820305 · doi ↗ · pubmed ↗
- 5Higgins JPT , Green S . Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. The Cochrane Collaboration; 2011.
- 6Stang A . Critical evaluation of the newcastle‐ottawa scale for the assessment of the quality of nonrandomized studies in meta‐analyses. Eur J Epidemiol. 2010;25:603‐605.20652370 10.1007/s 10654-010-9491-z · doi ↗ · pubmed ↗
- 7Hozo SP , Djulbegovic B , Hozo I . Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;1:13.10.1186/1471-2288-5-13PMC 109773415840177 · doi ↗ · pubmed ↗
- 8Araujo SE , Da SEAJ , de Campos FG , et al. Conventional approach x laparoscopic abdominoperineal resection for rectal cancer treatment after neoadjuvant chemoradiation: results of a prospective randomized trial. Rev Hosp Clin Fac Med Sao Paulo. 2003;58:133‐140.12894309 10.1590/s 0041-87812003000300002 · doi ↗ · pubmed ↗