A Case Presentation of Well-Differentiated Hepatocellular Carcinoma With No Sign of Liver Disease
Prachi Gedekar, Atul Chavhan, K. M. Hiwale, Shakti Sagar

TL;DR
This paper presents a rare case of liver cancer in an elderly man with no history of liver disease or risk factors.
Contribution
The novelty is the presentation of a well-differentiated HCC case without typical underlying liver disease.
Findings
The patient had no etiological factors for HCC such as alcohol or viral hepatitis.
The cancer showed well-differentiated features with minimal nuclear atypia.
The case highlights the possibility of HCC without traditional risk factors.
Abstract
The type of liver cancer that occurs most frequently is hepatocellular carcinoma (HCC). The majority of cases of HCC are secondary to alcoholic cirrhosis or viral hepatitis. The presence of malignant cells with modest nuclear atypia that resemble normal hepatocytes and the lack of bare nuclei in the smears, which shows the neoplastic hepatocytes' capacity, are characteristics of a well-differentiated HCC plasma membrane to tolerate smearing. We present the case of an 83-year-old male patient with a well-differentiated HCC, who had no etiological factors and no signs of alcohol cirrhotic liver, or any symptoms of liver disease which are the main causes of the HCC.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
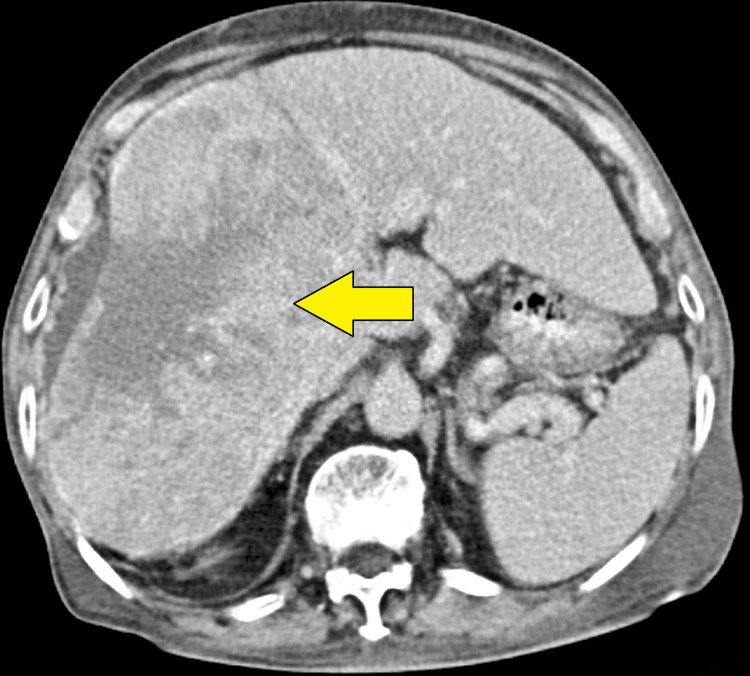 Figure 1
Figure 1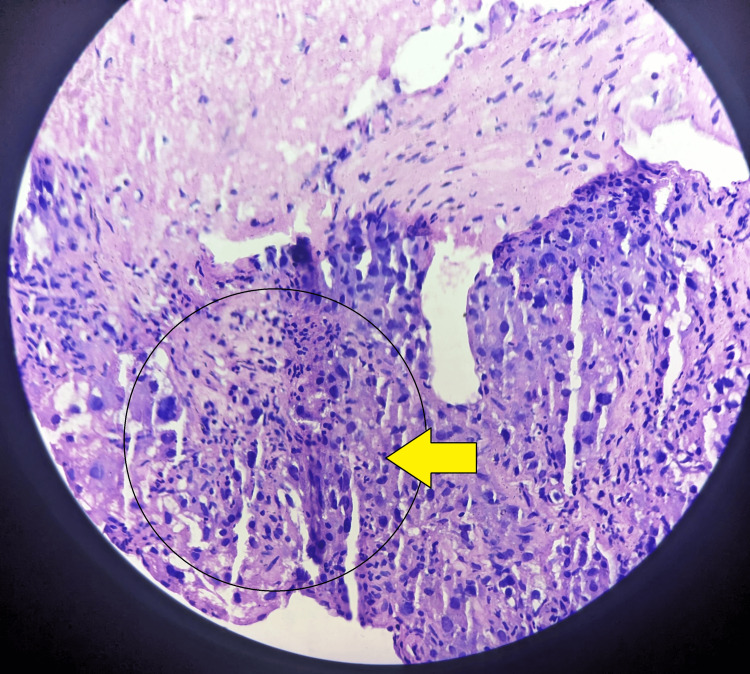 Figure 2
Figure 2| INVESTIGATION | OBSERVED VALUE | UNIT | REFERENCE RANGE |
| Hemoglobin Hb% | 12 | Gm% | Male 13-17; female 12-15 gm% |
| Red blood cell (RBC) count | 3.62 | Millions/cu.mm | Male 4.5-5.5 millions/cu.mm; female 3.8-4.8 millions/cu.mm |
| Whole blood count (WBC) | 7300 | /cu.mm | Male and female 4000-10000 cu.mm |
| Total platelet count | 187000 | 100000/cu.mm | Male and female 150000-410000 Lacs/cu.mm |
| Prothrombin time (PT) | 11 | Second | 10-12 sec |
| Partial thromboplastin time (PTT) | 31 | Second | 25-38 sec |
| Serum alpha-fetoprotein | 13 | Ng/ml | <7.22 IU/ml |
| # | Medicine | Quantity | Doses | Days |
| 1 | Tablet multivitamin | 10 | OD | 10 |
| 2 | Tablet vitamin C | 10 | OD | 10 |
| 3 | Tablet pantoprazole | 10 | OD | 10 |
| 4 | Tablet acetaminophen | 10 | BD | 10 |
| 5 | IV fluid vitamin K in 500 ml NS | 1 | OD | 1 |
| # | Medicine | Quantity | Doses | Days |
| 1 | Tablet multivitamin | 10 | OD | 10 |
| 2 | Tablet vitamin C | 10 | OD | 10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Liver Disease Diagnosis and Treatment · Cancer, Lipids, and Metabolism
Introduction
Globally, liver cancer has the fourth position in cancer-related fatalities and is the fifth most prevalent type of cancer. It is the fourth most common malignancy and the second most common cause of cancer-related death among men worldwide [1]. Compared to women, men are expected to acquire liver cancer [1]. Intrahepatic cholangiocarcinoma (ICC) and hepatocellular carcinoma (HCC) are two common forms of primary liver cancer; angiosarcoma, hemangiosarcoma, and hepatoblastoma are unusual forms [1]. Aristolochic acid and aflatoxins in food, chronic hepatitis B and C, alcoholism, and metabolic liver disease, especially nonalcoholic fatty liver disease are adverse conditions for HCC. Conventionally, histology or cytology has been used to make the diagnosis of HCC [2].
Early-stage HCC is asymptomatic, which causes a considerable delay in receiving a quick diagnosis. Patients with advanced HCC have limited access to effective therapy alternatives, and those with a diagnosis at the final stage of the disease are not eligible for curative surgery. The most popular biomarker for HCC surveillance and diagnosis is alpha-fetoprotein (AFP). It is utilized in conjunction with multiphasic computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound scanning (USS) as the sole phase V biomarker currently available for HCC surveillance [3]. One of the characteristics of cancer is metabolic change. Lipid accumulation is a distinctive pathological characteristic of HCC, occurring frequently in a well-differentiated HCC and infrequently in poorly differentiated HCC. It is common that depending on the grade of differentiation, HCC might alter the pathological characteristics. Of these, a well-differentiated HCC is recognized for being a fat-containing tumor; as the degree of differentiation decreases to moderate or poorly differentiated, the stored fat vanishes. It is believed that inadequate arterial development and reduced portal vein flow are the root causes of this fatty alteration in early-stage HCC [4]. Hepatocellular adenoma in non-cirrhotic liver and high-grade dysplastic nodule in cirrhosis can be mimicked by a well-differentiated HCC [5]. HCCs are thought to expand and become more malignant over time, progressing progressively from a well-differentiated HCC to intermediate HCC and then poorly differentiated HCC. Therefore, well-differentiated HCCs, whose average diameter is less than 20 mm, are an early form of HCCs in hepatocarcinogenesis. The portal vein and hepatic artery supply the HCC and the liver parenchyma. Generally speaking, well-differentiated HCCs develop into moderately differentiated HCCs when the tumor's primary blood supply shifts from the portal tracts to the arteries. Diverse fatty tissue grades are frequently present in HCCs. This fatty transformation is more common in tiny, well-differentiated HCC nodules, particularly those with a diameter of less than 20 mm. A well-differentiated HCC with fatty alteration is quite uncommon to progress to over 30 mm [6].
Case presentation
We present the case of an 83-year-old man who complained of stomach pain and was admitted to the hospital. He also reported low appetite and swelling on his limb. Large heterogeneously enhancing lesions are visible on the CT image of the abdomen and pelvis, and a well-circumscribed soft tissue density mass lesion measuring 14 × 13 cm is observed in the right lobe of the liver (Figure 1). The mass injury is causing capsular retraction with surrounding perihepatic fluid. The examination of the abdomen is completed. Examination of other systems was unremarkable.
Computed tomography revealed a hypoechoic lesion in the right lobe of the liver (indicated by yellow arrow) with ascites
A lab investigation was done. All lab parameters are normal as shown in Table 1.
Multiple core biopsies, collectively measuring 1.0 × 0.2 cm, were received at the histopathology laboratory. The histopathology report revealed that sections show hyperchromatic nuclei tumor cells arranged in a trabecular pattern, resemble large round to polygonal mature hepatocytes, large pleomorphic nuclei, mild nuclear atypia, and clear to eosinophilic cytoplasm well-differentiated HCC as shown in Figure 2.
Microscopy of the liver biopsy shows tumor cells in trabecullar pattern with mature hepatocytes with eosinophilic cytoplasm
Medications given to the patient during hospitalization are shown in Table 2.
After the reports of histopathology, the disease was explained to the patient, and the patient was advised to stay and be treated in the hospital, but the patient wants to be discharged from the hospital and thus has been given discharge upon patient request with prescription shown in Table 3.
Discussion
Thompson et al.'s study demonstrates that compared to weakly differentiated HCC, around 28% of HCC tumors with well and moderate differentiation are more rigid, implying that tumor stiffness as measured by magnetic resonance elastography (MRE) might be a helpful imaging biomarker to distinguish between different HCC tumor grades [7]. It is unclear how highly differentiated HCC differs from poorly differentiated HCC in terms of stiffness. Decreased vascularity and greater necrosis could account for the reduced stiffness in poorly differentiated HCC [7]. However, the part of tumor stiffness only took into account the solid, enhancing portion of the tumor estimate in the current investigation. One theory holds that by definition, highly and moderately differentiated HCCs exhibit an extra-organized tissue architecture trabecular pattern in contrast to weakly differentiated HCCs, which retain their trabecular pattern HCC [7].
As per the study of Hong et al., aberrant reticulin stain, pattern-reduced reticulin stain, or expanded trabeculae are thought to be accurate in identifying a well-differentiated HCC, while odd reticulin stain patterns can occasionally be found. A portion of HCC's maintained reticulin staining represents a variety of tumor reticulin staining patterns reported in this article. In tiny samples like cellblocks or small core biopsies, an intact reticulin staining pattern is uncommon, but it has to be identified when making a diagnosis of a well-differentiated HCC [8].
Kim's study demonstrates that in most well-differentiated HCCs, improved by superparamagnetic iron oxide (SPIO), 85% had hyperintensity; however, these tumors also displayed varied CT density patterns. The majority of hyperintense, well-differentiated HCCs as shown on SPIO-enhanced MRI were influenced by the CT density pattern [9].
Conclusions
An 83-year-old male presented with a massive well-differentiated hepatocyte carcinoma (HCC) in the right lobe of the liver, although there were no distant lesions. Hepatocellular carcinoma typically develops in the context of chronic cirrhosis related to hepatitis B and hepatitis C infections. This case involves an 83-year-old male patient with a well-differentiated HCC in a non-cirrhotic liver, despite the absence of chronic hepatitis or any evident etiological or risk factor for HCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification Adv Cancer Res Chidambaranathan-Reghupaty S Fisher PB Sarkar D 16114920213357942110.1016/bs.acr.2020.10.001PMC 8796122 · doi ↗ · pubmed ↗
- 2A global view of hepatocellular carcinoma: trends, risk, prevention and management Nat Rev Gastroenterol Hepatol Yang JD Hainaut P Gores GJ Amadou A Plymoth A Roberts LR 5896041620193143993710.1038/s 41575-019-0186-y PMC 6813818 · doi ↗ · pubmed ↗
- 3Hepatocellular carcinoma: old friends and new tricks Exp Mol Med Kim E Viatour P 189819075220203326883410.1038/s 12276-020-00527-1PMC 8080814 · doi ↗ · pubmed ↗
- 4Metabolic alteration in hepatocellular carcinoma: mechanism of lipid accumulation in well-differentiated hepatocellular carcinoma Can J Gastroenterol Hepatol Suzuki H Kohjima M Tanaka M 8813410202120213368109110.1155/2021/8813410 PMC 7910064 · doi ↗ · pubmed ↗
- 5Combined use of heat-shock protein 70 and glutamine synthetase is useful in the distinction of typical hepatocellular adenoma from atypical hepatocellular neoplasms and well-differentiated hepatocellular carcinoma Mod Pathol Nguyen TB Roncalli M Di Tommaso L Kakar S 2832922920162676913810.1038/modpathol.2015.162PMC 5292872 · doi ↗ · pubmed ↗
- 6Atypically large well-differentiated hepatocellular carcinoma with extensive fatty metamorphosis: report of a case J Med Invest Ishikawa D Shimada M Utsunomiya T 2672716020132419004610.2152/jmi.60.267 · doi ↗ · pubmed ↗
- 7MR elastography of hepatocellular carcinoma: correlation of tumor stiffness with histopathology features-preliminary findings Magn Reson Imaging Thompson SM Wang J Chandan VS Glaser KJ Roberts LR Ehman RL Venkatesh SK 41453720172784524510.1016/j.mri.2016.11.005PMC 5587120 · doi ↗ · pubmed ↗
- 8SPIO-enhanced MRI findings of well-differentiated hepatocellular carcinomas: correlation with MDCT findings Korean J Radiol Kim SH Lee WJ Lim HK Park CK 1121201020091927085610.3348/kjr.2009.10.2.112PMC 2651447 · doi ↗ · pubmed ↗