Infliximab-Induced Improvement in Dercum's Disease
Cailean E McKay, Ishaan Batish, Shiva Arami

TL;DR
A patient with Dercum's disease showed improvement after treatment with infliximab and methotrexate.
Contribution
This case report presents a potential new treatment approach for Dercum's disease using infliximab.
Findings
A patient with Dercum's disease showed improvement with infliximab and methotrexate.
Current treatment for Dercum's disease is limited to pain management.
Abstract
Dercum’s disease (DD) is a rare and poorly understood disease characterized by obesity and painful lipomas throughout the body. Although the entity is well described in the literature, its etiology, prevalence, and treatment remain unclear. Currently, treatment is focused on pain management. We describe a case of a patient with DD who showed improvement with infliximab and methotrexate.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
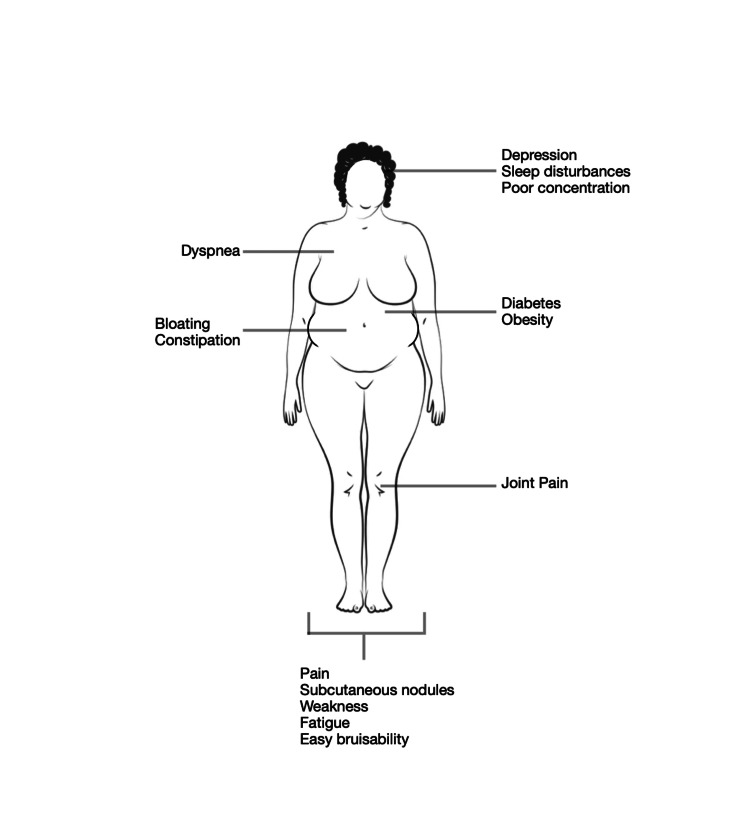 Figure 1
Figure 1| Date | Clinical activity |
| March 2019 | First visit to the clinic |
| April 2019 | First infliximab infusion at 3 mg/kg |
| June–December 2019 | Infliximab infusions every eight weeks; pain improvement noted during clinic visits |
| January 2020 | Improvement in the size of forearm lipomas noted on ultrasound |
| February–May 2020 | No infliximab due to the COVID-19 pandemic |
| May 2020 | Telehealth visit, endorsed worsening pain since stopping infliximab |
| August 2020 | Surgery to resect lipomas, clinic visit |
| September 2020 | Established with pain clinic |
| January 2021 | Clinic visit, decision made to restart infliximab and methotrexate |
| February 2021 | First infliximab infusion at 5 mg/kg |
| May 2021 | Clinic visit with reported improvement in pain |
| July 2021 | Experiencing significant pain, requested to stop infliximab and methotrexate |
| April 2022 | Returned to clinic for refill of pain medication, instructed to follow up with pain clinic |
| Type | Description | |
| I | Generalized diffuse | Diffusely widespread painful adipose tissue without clear lipomas |
| II | Generalized nodular | General pain in adipose tissue and intense pain in and around multiple lipomas |
| III | Localized nodular | Pain in and around multiple lipomas |
| IV | Juxta-articular | Solitary deposits of excess fat, for example at the medial aspect of the knee |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders · Skin Diseases and Diabetes · Nail Diseases and Treatments
Introduction
Dercum’s disease (DD), also called adiposis dolorosa, is a rare entity that is characterized by obesity and chronic pain due to subcutaneous adipose tissue growth, predominantly seen in women aged 35-50 [1]. Often seen additional symptoms include weakness, fatigue, easy bruising, sleep disturbances, dyspnea, joint pain, and neuropsychiatric symptoms, such as emotional instability and depression [2]. The painful adipose tissue can be diffuse or localized to lipoma-like masses. The most commonly affected areas are the extremities, trunk, pelvic area, and buttocks.
DD is a diagnosis of exclusion and is made clinically. On pathology, excised tissue is consistent with fatty connective tissue without signs of inflammation [3]. On examination and imaging, the tender tissue often appears similar to a lipoma, and there are no laboratory tests to distinguish between the two [4].
There is currently no standard treatment for DD, and effective treatment is lacking. Primarily, management has been through pain control, both through medication and surgical excision of painful lesions [5-7]. Patient’s with DD are often prescribed nonsteroidal anti-inflammatory drugs (NSAIDs) and various formulations of lidocaine. There have been various case reports showing the benefit of a variety of different agents [8-11], as well as a single case report showing improvement with infliximab and methotrexate [12].
Case presentation
A 56-year-old female was referred to our clinic in 2019 for further evaluation of DD. She had received a diagnosis two years prior, following a prolonged period of developing painful soft tissue nodules, predominantly in her legs. During this time, she underwent multiple surgeries to remove approximately 30 of these masses.
Past medical history was significant for obesity (body mass index (BMI) > 40), type 2 diabetes mellitus, fibromyalgia, hypertension, and possibly Crohn’s disease. Review of records from her prior rheumatologist showed mildly elevated sedimentation rate, negative rheumatoid factor, and ANA positive at a titer of 1:40. For her DD, she had tried pregabalin, gabapentin, NSAIDs, duloxetine, topiramate, and opiates with little relief or intolerable side effects. Her sleep and activities of daily living (ADLs) were impacted by the level of pain she experienced. She was able to tolerate tramadol, which was prescribed to her by a pain management clinic. Eventually, methotrexate was initiated at 25 mg subcutaneously weekly. She did experience some improvement with the methotrexate, but eventually felt like her pain was worsening again, at which point she was referred to our clinic.
Given her previous improvement with methotrexate, infliximab was initiated at a dose of 3 mg/kg, administered every eight weeks after loading doses. After four infusions, she began to report improvement in her pain. After several months, improvement in size of some of her fatty nodules were noted on in-clinic ultrasound.
Unfortunately, after eight months of infliximab, the patient was unable to return to the clinic for infusions due to the COVID-19 pandemic. In May 2020, approximately six months after her last infusion, she returned to the clinic and reported significantly increased pain. She was unable to restart infliximab until February 2021 due to surgery to remove several fatty nodules. In the interim, she established with a pain clinic and used Norco 10 mg every four hours as needed for pain. Infliximab was restarted and her dose was increased to 5 mg/kg, as well as restarting methotrexate at a dose of 10 mg weekly. She initially felt significant improvement with reinitiation of infliximab. However, by July 2021, the patient no longer felt like she was experiencing improvement, so both infliximab and methotrexate were discontinued. The patient was lost to follow-up until May 2022; in the interim, she had surgery to remove several painful lipomas. At that time, she was discharged from our rheumatology clinic and instructed to follow with pain management.
The patient's timeline with our clinic is summarized in Table 1.
Discussion
DD, also known as adiposis dolorosa, is a rare disorder characterized by painful subcutaneous lipomas most frequently distributed on the extremities, trunk, and buttocks. Associated symptoms include weakness, fatigue, easy bruisability, sleep disturbances, joint pain, and neuropsychiatric complaints, such as depression and poor concentration (Figure 1) [3].
Signs and symptoms of Dercum's diseaseAdapted from Hansson et al [2].This is an Open Access article distributed under the terms of the Creative Commons Attribution License.
It has been proposed that DD be defined as chronic (>3 months) painful adipose tissue in conjunction with obesity. Four distinct subtypes have been proposed: type I, a generalized diffuse form with widespread, painful fatty tissue without any distinct lipomas; type II, a generalized nodular form presenting with widespread pain in and around multiple lipomas throughout the body; type III, a localized nodular form with painful lipomas in limited areas; and type IV, the juxta-articular form that presents with painful fatty tissue near large joints, such as the knee, hip or elbow, as summarized in Table 2 [2]. Most cases of DD appear to occur sporadically, although there have been reports suggesting an autosomal dominant inheritance pattern [13].
The pathogenesis of DD has not been elucidated, although various theories have been proposed. Compression of nerves by adipose tissue and disturbance of subcutaneous blood flow are common theories [14], but this has never been shown on pathology [2-4]. Endocrine dysfunction or alterations in lipid metabolism have also been suggested, given the prevalence of metabolic derangements, such as diabetes in patients with DD [1]. By contrast, it has also been shown that adipocytes secrete pro-inflammatory cytokines, including TNF-alpha and interleukin-6 [15].
Given that the underlying mechanism of DD is not known, there is no standard treatment and therapy has mainly focused on pain relief. Liposuction is a fairly common surgical method used to treat areas of painful fat [3]. Several small studies have shown improvement in pain after these procedures, although the pain relief may diminish over time [16]. However, liposuction is more effective for patients with diffuse disease, rather than a nodular form. Dermolipectomy or lipectomy have also been used for larger, nodular masses [5]. Transcutaneous electrical stimulation has been reported as a safe and effective treatment, and a small study has shown whole body pneumatic compression to be effective [3].
Pharmacologically, treatment in the past has focused mostly on pain relief. Lidocaine has been used in the form of topical application, intralesional injections, and infusions. The latter two forms have been shown to bring relief for multiple months [6,7]. There are mixed reports on corticosteroids; generally, they provide no relief, and one case study showed a link between corticosteroid use developing DD, although conversely, one case report has shown improvement with intralesional injections [3]. Recently, it has been reported that injections of deoxycholic acid into lipomas of patients with DD improved pain [3]. Oral NSAIDs and opiates have been a mainstay for pain relief, and there have been cases showing benefits with metformin [8], pregabalin [9], interferon alpha-2b [10], and d-amphetamine [11].
Previously, there had been one case report showing improvement with methotrexate and infliximab in a patient with DD who also had a history of ankylosing spondylitis [12]. Given the secretion of TNF-alpha and IL-6 by adipocytes [17], there is a reason to believe that anti-TNF therapy would lead to improvement in pain and inflammation. Furthermore, TNF-alpha has been implicated in the release of free fatty acids [15], leading to a decrease in peripheral insulin sensitivity; if fatty acid metabolism plays a role in DD, inhibition of this process could lead to improvement. In our case, the patient did show improvement with her initial course of infliximab, and some improvement with re-initiation. Given the well-known fact that patients can develop antibodies to TNF inhibitors [18], it is possible that her lack of long-term improvement with infliximab was secondary to development of these antibodies, given the intermittent nature of her treatment. TNF-inhibitors, however, do have risk of serious but rare side effects, including invasive fungal infections and tuberculosis [19,20], so they must be used with caution.
Conclusions
DD is a rare condition characterized by painful lipomas, obesity, and nonspecific constitutional symptoms. Patients with DD are difficult to diagnose and manage, given the rarity of its presentation and the lack of standardized treatment. This case report brings further attention to methotrexate and infliximab as a possible treatment for patients with refractory disease. Further research is necessary to help find a definitive method for diagnosing and treatment of DD and to determine etiology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adiposis dolorosa is more than painful fat The Endocrinologist Herbst KL Asare-Bediako S 326334172007
- 2Review of Dercum's disease and proposal of diagnostic criteria, diagnostic methods, classification and management Orphanet J Rare Dis Hansson E Svensson H Brorson H 23720122254624010.1186/1750-1172-7-23PMC 3444313 · doi ↗ · pubmed ↗
- 3Dercum's disease (adiposis dolorosa): a review of clinical presentation and management Reumatologia Kucharz EJ Kopeć-Mędrek M Kramza J Chrzanowska M Kotyla P 2812875720193184434110.5114/reum.2019.89521 PMC 6911249 · doi ↗ · pubmed ↗
- 4Histology of adipose tissue inflammation in Dercum's disease, obesity and normal weight controls: a case control study J Inflamm (Lond) Hansson E Svensson H Stenram U Brorson H 24820112195569610.1186/1476-9255-8-24PMC 3195089 · doi ↗ · pubmed ↗
- 5Juxta-articular adiposis dolorosa (Dercum's disease type IV): report of four cases and treatment by dermolipectomy Wien Med Wochenschr Wollina U Heinig B Langner D Nowak A 37437716520152628959510.1007/s 10354-015-0378-1 · doi ↗ · pubmed ↗
- 6Treatment of pain in Dercum's disease with Lidoderm (lidocaine 5% patch): a case report Pain Med Desai MJ Siriki R Wang D 12241226920081834606710.1111/j.1526-4637.2008.00417.x · doi ↗ · pubmed ↗
- 7Dercum's disease (adiposis dolorosa). Treatment of the severe pain with intravenous lidocaine Pain Petersen P Kastrup J 7780281987382249710.1016/0304-3959(87)91062-1 · doi ↗ · pubmed ↗
- 8A successful case of pain management using metformin in a patient with adiposis dolorosa Int J Clin Pharmacol Ther Łabuzek K Liber S Suchy D OkopieńB 5175245120132361157510.5414/CP 201878 · doi ↗ · pubmed ↗