Hyperosmolar Hyperglycemic State-Induced Hyperviscosity as a Catalyst for Multiple Embolic Strokes
Lorena Escaño, Prarthana Desai

TL;DR
This paper discusses a rare case where a severe hyperglycemic state led to multiple strokes, highlighting the need for better understanding of the associated risks.
Contribution
The paper presents a rare clinical case linking hyperosmolar hyperglycemic state with multiple embolic strokes.
Findings
An 86-year-old male with HHS developed multiple embolic strokes during hospitalization.
The case highlights the prothrombotic state associated with HHS and its potential to cause cerebral infarction.
Clinical vigilance is emphasized for early recognition of stroke in patients with hyperglycemic crises.
Abstract
Hyperosmolar hyperglycemic state (HHS) is the most serious emergency in patients with uncontrolled diabetes mellitus. It has been associated with a prothrombotic state that increases the risk for ischemia in affected patients. Despite the literature on the risk of ischemic stroke in patients with chronic hyperglycemia being vast, there is not enough documentation on the risk of developing a stroke during a hyperglycemic crisis. We present a rare case of an 86-year-old male who was admitted with HHS whose hospital course was further complicated by multiple embolic strokes. Prompt recognition of cerebral infarction when it intertwines with HHS remains a challenging task. This case emphasizes the value of clinical vigilance in patients with this hyperglycemic crisis. Further research is needed to better understand what this prothrombotic state truly entails in these patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
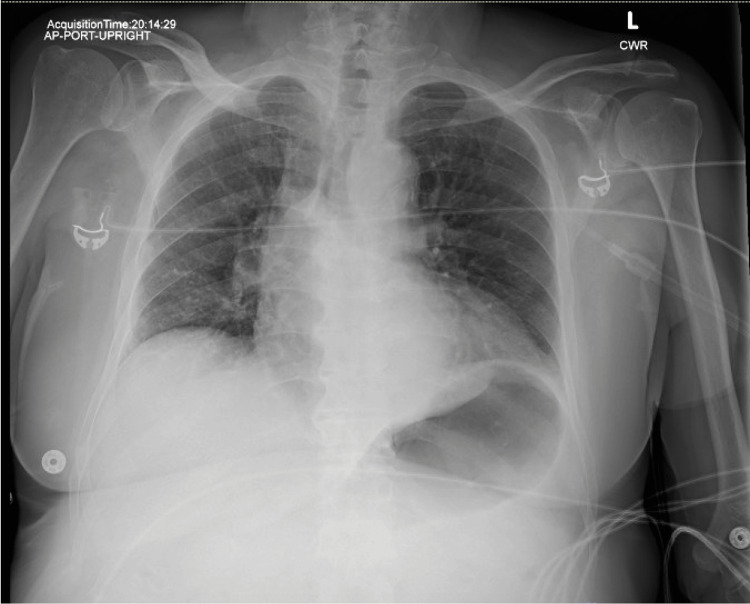 Figure 1
Figure 1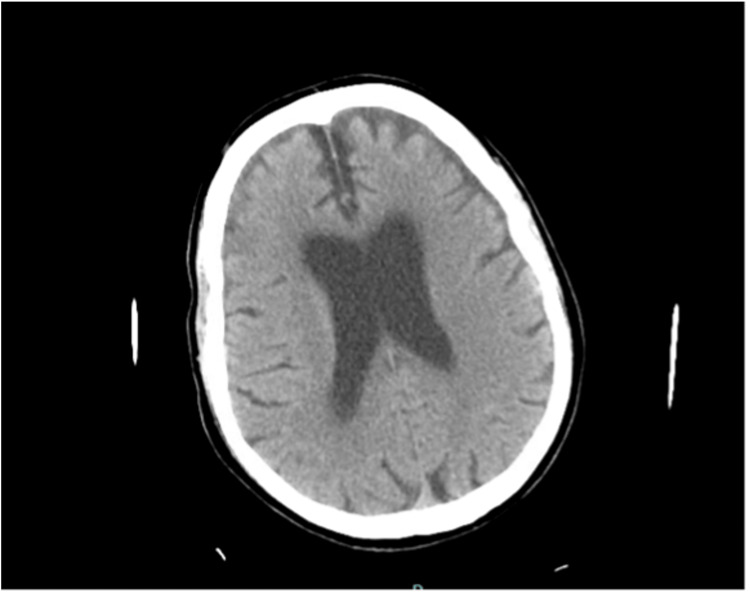 Figure 2
Figure 2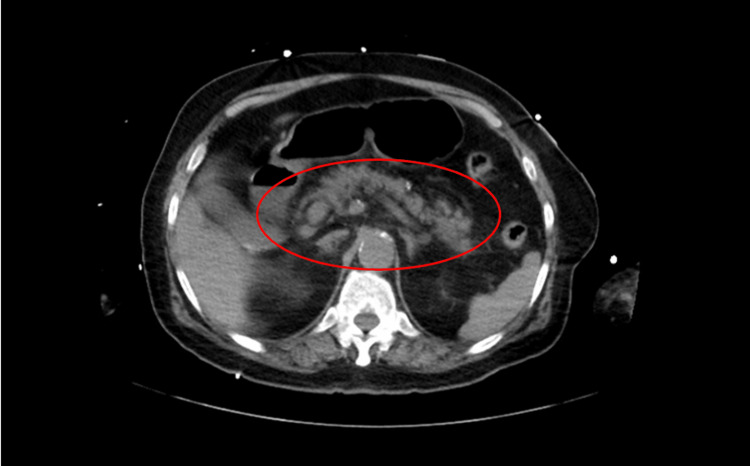 Figure 3
Figure 3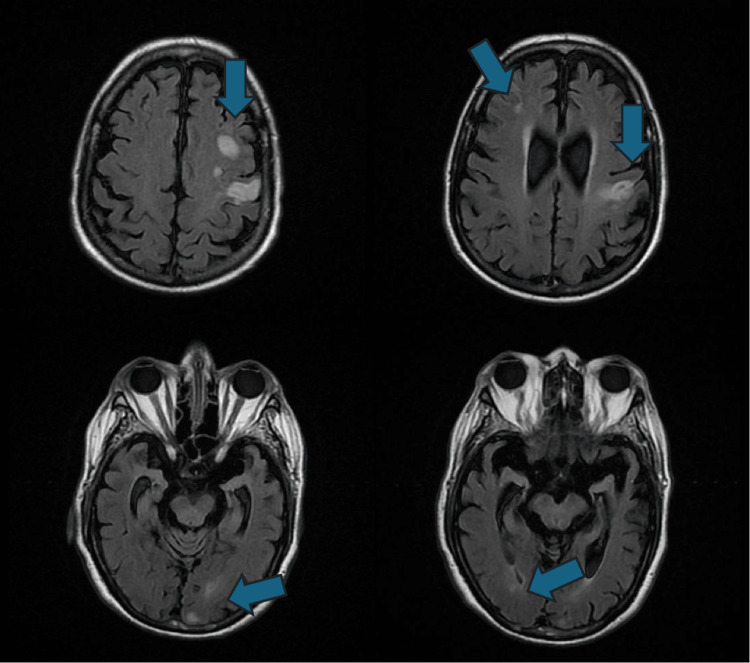 Figure 4
Figure 4| Laboratory test | Laboratory result | Reference value |
| Glucose | >1500 mg/dl | 70 – 99 mg/dl |
| Serum osmolality | 354 mOsm/kg | 275 – 295 mOsm/kg |
| Bicarbonate | 19 mmol/L | 22 – 29 mmol/L |
| Anion gap | 24 mmol/L | 8 – 18 mmol/L |
| Venous pH | 7.23 | 7.32 – 7.43 |
| Beta hydroxybutyrate | 3.9 mmol/L | 0 – 0.4 mmol/L |
| Lactic acid | 3.6 mmol/L | 0.5 – 2.2 mmol/L |
| Lipase | 1,825 U/L | 13 – 60 U/L |
| Triglycerides | 420 mg/dL | 0 – 149 mg/dL |
| Corrected sodium | 153 mmol/L | 135 – 145 mmol/L |
| Potassium | 4.5 mmol/L | 3.5 – 5.3 mmol/L |
| Creatinine | 2.10 mg/dL | 0.67 – 1.23 mg/dL |
| Glomerular filtration rate | 30 mL/min | >60 mL/min |
| White blood cells | 19,100 | 3,500 – 10,000 |
| Platelet count | 334,000 | 150,000 – 400,000 |
| Hemoglobin | 13.9 | 13.5 – 17 |
| Hematocrit | 44.1% | 38 – 50 |
| Hemoglobin A1C | 12.7% | <5.7% |
| INR | 1.12 | 0.91 – 1.40 |
| PT | 14.4 | 12.2 – 14.5 |
| PTT | 32.9 | 25 – 35.8 |
| Glucose level on admission | >1500 mg/dl |
| Glucose level 4 hours post admission | 1210 mg/dl |
| Glucose level 8 hours post admission | 895 mg/dl |
| Glucose level 12 hours post admission | 715 mg/dl |
| Glucose level 16 hours post admission | 468 mg/dl |
| Glucose level 20 hours post admission | 429 mg/dl |
| Glucose level 24 hours post admission | 277 mg/dl |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Acute Ischemic Stroke Management · Diabetes and associated disorders
Introduction
Hyperosmolar hyperglycemic state (HHS) is one of the metabolic emergencies that can arise in decompensated diabetes mellitus. Despite well-developed diagnostic criteria and treatment protocols, it remains an important cause of mortality which approaches 20% in affected patients. Its danger lies in the fact that it typically impacts elderly patients with multiple comorbidities. In addition to this, it has a gradual onset, and the severe dehydration and increased plasma osmolality seen in these patients can ultimately lead to coma and death [1].
Multiple precipitating factors have been described for HHS, inadequate glycemic control and infection being the most common. However, some of the complications that can arise due to this metabolic emergency are less documented in the literature. In particular, the hypercoagulable state seen in affected patients can result in vessel thrombosis with subsequent myocardial infarction, cerebrovascular accident, pulmonary embolism or limb ischemia [2-5].
Case presentation
We present an 86-year-old male brought to the emergency department after being found lying on his bathroom floor, profoundly lethargic and confused. Past medical history was remarkable for hypertension on amlodipine, heart failure with preserved ejection fraction on spironolactone and furosemide, and hyperlipidemia on atorvastatin. There was no known history of diabetes.
The family at bedside reported the patient having a four-day history of decreased appetite with poor oral intake, generalized weakness, and increased urinary frequency. Symptoms continued to progress and the patient became lethargic and confused. EMS was called when the patient was found on his bathroom floor.
Upon arrival to the emergency department, the patient was restless, confused, afebrile, blood pressure 137/65 mmHg, heart rate of 108 b/m, respiratory rate 24 r/m, saturating well on room air. Physical examination was only remarkable for mild epigastric tenderness. No focal neurological deficit was appreciated.
Pertinent laboratory values on admission are presented in Table 1. Urinalysis showed 2+ glucose and trace ketones.
Chest X-ray on admission showed no acute cardiopulmonary process (Figure 1). CT of the head was unremarkable for any acute intracranial abnormality (Figure 2). CT abdomen and pelvis showed peripancreatic fat stranding concerning for acute pancreatitis (Figure 3). Abdominal ultrasound was unremarkable for obstructive biliary disease.
Anteroposterior chest x-ray on admission
Computed tomography of the head on admission
Computed tomography of the abdomen without contrast showing peripancreatic fat stranding on admission
The patient was admitted with a working diagnosis of hyperosmolar hyperglycemic state with a component of diabetic ketoacidosis (DKA) and acute pancreatitis as the likely precipitant.
Given worsening mental status and tachypnea, the patient was intubated and sedated for airway protection. Initial management included IV fluids and insulin drip with subsequent improvement of glycemia. The rate of hyperglycemia correction is illustrated in Table 2. It was corrected at 40-80 mg/dl per hour as per protocol to avoid the development of cerebral edema.
On day two of hospitalization, while weaning the patient off sedation, he was found to have new right-sided hemiparesis prompting further workup. MRI of the brain without contrast revealed multiple small acute infarcts within both frontal lobes, left frontoparietal region and occipital lobe affecting multiple vascular territories (Figure 4). Echocardiogram showed preserved ejection fraction without findings concerning for intracardiac thrombus. Carotid duplex was unremarkable. Cardiac monitoring was without evidence of atrial fibrillation. Neurology was consulted and the patient was started on Aspirin as per protocol. Home atorvastatin dose was increased. Prophylactic heparin which was initially held due to gastrointestinal bleed with dropping hemoglobin was also resumed.
Magnetic resonance imaging of the brain. Axial T2 fluid attenuated inversion recovery (FLAIR) imaging
The patient’s poor mental status and neurological deficits persisted and started to improve very gradually despite correction of severe hyperglycemia. He was ultimately discharged to an acute rehabilitation facility to continue therapy for residual neurological deficits. The acute pancreatitis improved with conservative management without the need for further interventions. The patient was eventually transitioned to a subcutaneous insulin regimen with the plan to continue new-onset diabetes work-up as an outpatient.
Discussion
We have presented here a compelling case involving an 86-year-old male who was initially admitted with a hyperosmolar hyperglycemic state and a component of DKA, likely precipitated by acute pancreatitis, whose hospital course was further complicated by multiple embolic strokes.
Profound dehydration, significant hyperglycemia and hyperosmolarity with some degree of altered mentation, are all well-known features of HHS. However, less discussed in literature is that these metabolic derangements can lead to a prothrombotic state, further increasing the risk of ischemia in these patients. The severe hyperglycemia seen in HHS leads to significant osmotic diuresis which ends up in severe dehydration. This results in the concentration of blood constituents causing increased blood viscosity and stasis. Adding to the pathogenesis, the hyperglycemia and elevated osmolality precipitate endothelial cell dysfunction which promotes vasoconstriction. This cascade of events is further exacerbated by the release of coagulation factors and platelet hyperactivity, as well as stress-induced release of proinflammatory cytokines. Each one of these events results in a prothrombotic state that increases the risk for ischemia as seen in our patient [2].
The current guidelines for the management of HHS advise the use of prophylactic anticoagulation for the entire duration of the hospital stay, unless there are contraindications [4]. Our patient had a prolonged hospital stay that was complicated by an episode gastrointestinal bleed and downtrending hemoglobin, causing pharmacological prophylactic anticoagulation to be deferred. Once his hemoglobin stabilized and the benefits outweighed the risks, prophylactic anticoagulation was resumed.
A few case reports have documented this prothrombotic state seen in HHS presenting as ischemic stroke, venous thrombosis, pulmonary embolism, myocardial infarction and even acute limb ischemia [2,4,5]. However, the occurrence of stroke as a complication of this hypercoagulable state is not that well detailed in the literature as HHS on its own can present as a stroke mimic with neurological deficits and even MRI abnormalities. Despite similar presentation, when HHS presents as a stroke mimic, complete resolution of symptoms is seen once severe hyperglycemia is corrected [3]. In view of this, when both HSS and ischemic stroke coexist, the diagnosis of the latter can be a clinical challenge and can be delayed.
An intriguing aspect of this case was the development of new neurological deficits on day two of hospitalization and lack of resolution of symptoms once the severe hyperglycemia improved. This in addition to the MRI findings reinforce the diagnosis of hyperviscosity-induced multiple embolic strokes in the setting of hyperosmolar hyperglycemic state.
Conclusions
This case emphasizes the importance of recognizing this prothrombotic state with higher risk of ischemia as a potential complication of hyperosmolar hyperglycemic state. In addition to this, it highlights the clinical complexity of HHS and acute stroke when they coexist. This can lead to delayed diagnosis and management of a neurological disease that can lead to deleterious outcomes if left untreated, especially when time-sensitive interventions such as thrombolysis and thrombectomy are warranted.
Further research is needed to gain a deeper understanding of what this hypercoagulable state truly implies in these patients, including its characteristics and overall risk increment of ischemia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hyperglycemic crises: diabetic ketoacidosis and hyperglycemic hyperosmolar state Diabetes Complications, Comorbidities and Related Disorders Umpierrez GE Cham Springer 2020
- 2Hyperglycemic hyperosmolar state causing multiple thrombosis Qatar Med J Ganaw AE Shaikh N Marcus A Soekarman D 7320192019
- 3Hyperosmolar hyperglycaemic state as a stroke cause or stroke mimic: an illustrative case and review of literature Clin Med (Lond) Marren SM Beale A Yiin GS 83862220223507879910.7861/clinmed.2021-0734 PMC 8813015 · doi ↗ · pubmed ↗
- 4Increased risk of ischemic stroke after hyperosmolar hyperglycemic state: a population-based follow-up study P Lo S One Wang JY Wang CY Huang YS 09201410.1371/journal.pone.0094155 PMC 397976224714221 · doi ↗ · pubmed ↗
- 5Triple emergencies: hyperosmolar hyperglycemic state, venous thromboembolism, and huge free-floating right heart thrombus successfully managed with anticoagulation Clin Case Rep Umar H Zagga UM Akintomide FA 09202110.1002/ccr 3.4710 PMC 871084934963797 · doi ↗ · pubmed ↗