Cryobiopsy for Secondary Pulmonary Alveolar Proteinosis
Hiroshi Kobe, Nobuyoshi Hamao, Takashi Niwa, Tadashi Ishida

TL;DR
This paper presents a case where transbronchial lung cryobiopsy successfully diagnosed secondary pulmonary alveolar proteinosis without complications.
Contribution
The paper introduces the first reported use of TBLC for diagnosing SPAP, highlighting its utility and safety.
Findings
TBLC provided sufficient tissue for diagnosing SPAP.
No adverse events occurred during or after the procedure.
TBLC is a viable diagnostic tool for SPAP, which is rarely reported.
Abstract
Secondary pulmonary alveolar proteinosis (SPAP) is one of the diffuse parenchymal lung diseases, and the utility and safety of transbronchial lung cryobiopsy (TBLC) for diagnosing SPAP are unknown. A case of SPAP diagnosed by TBLC is presented. Specimens that were useful for diagnosis were collected, and there was no adverse event following TBLC. The usefulness of TBLC for interstitial lung disease has been widely reported, but there are few reports of SPAP. We present the clinical course of TBLC in the diagnosis of SPAP.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
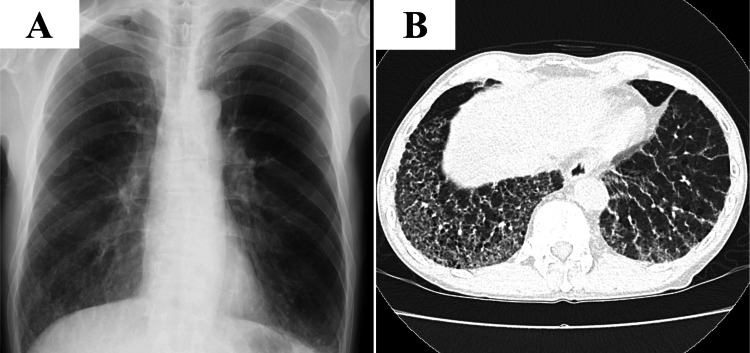 Figure 1
Figure 1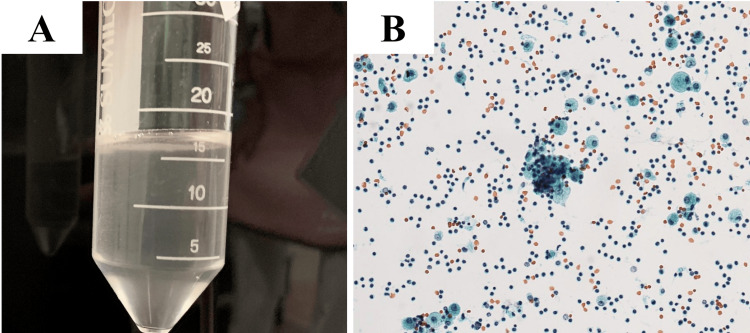 Figure 2
Figure 2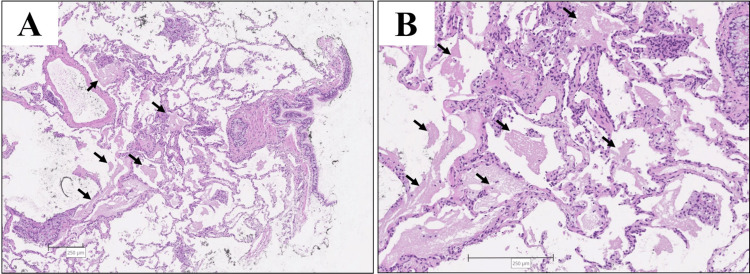 Figure 3
Figure 3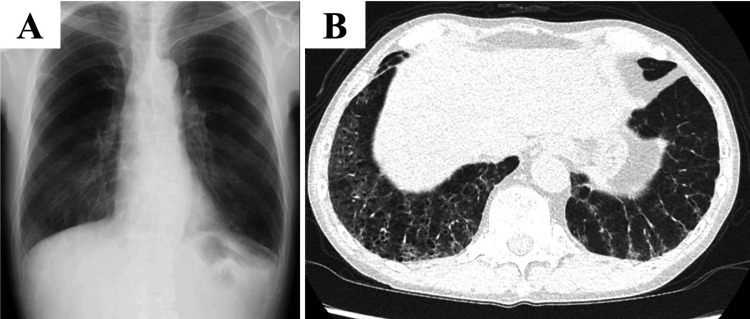 Figure 4
Figure 4| Hematology and biochemistry | Patient's value | Normal value |
| White blood cells (WBC) | 3700 | 3300-8600/μL |
| Neutrophils | 50.2 | 38.0-77.0 % |
| Lymphocytes | 36.9 | 15.0-53.0 % |
| Monocytes | 9.7 | 0-13.0 % |
| Eosinophils | 1.9 | 0-6.0 % |
| Basophils | 1.3 | 0-2.0 % |
| Hemoglobin (HB) | 14.2 | 13.7-16.8 g/dL |
| Platelets (PLT) | 22.7×104 | 16.0-36.0×104 /μL |
| Total protein (TP) | 7.8 | 6.6-8.1 g/dL |
| Albumin (ALB) | 3.5 | 4.1-5.1g/dL |
| Aspartate aminotransferase (AST) | 208 | 13-30U/L |
| Alanine aminotransferase (ALT) | 47 | 10-42U/L |
| Lactate dehydrogenase (LDH) | 334 | 124-222U/L |
| Blood urea nitrogen (BUN) | 7 | 8-20mg/dL |
| Creatinine (CRE) | 0.72 | 0.65-1.07mg/dL |
| Sodium (Na) | 140 | 138-145mmol/L |
| Potassium (K) | 4.3 | 3.6-4.8mmol/L |
| C-reactive protein (CRP) | 0.02 | 0-0.14mg/dL |
| Krebs von den Lungen-6 (KL-6) | 8071 | 105-401U/mL |
| Surfactant protein-D (SP-D) | 2360 | <110ng/mL |
| Antinuclear antibody (ANA) | 80 times | <40 times |
| Anti-neutrophil cytoplasmic antibody (ANCA) | negative | negative |
| anti-cyclic citrullinated peptide (CCP) | <0.5 | <4.5U/mL |
| anti-aminoacyl tRNA synthetase (ARS) | <5.0 | <25.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Neonatal Respiratory Health Research · Congenital Diaphragmatic Hernia Studies
Introduction
Pulmonary alveolar proteinosis (PAP) is one of the diffuse parenchymal lung diseases characterized by the accumulation of lipoproteinaceous material in alveolar regions due to abnormal surfactant homeostasis of alveolar macrophages [1]. Secondary PAP (SPAP) accounts for 5-10% of adult PAP cases caused by hemopoietic disorders, immune dysregulation, infections, inhalation, lysinuric protein intolerance, and drug-induced or iatrogenic. 25-53% of SPAP cases require video-assisted thoracoscopic surgery (VATS) or open lung biopsy because bronchoalveolar lavage (BAL) and transbronchial lung biopsy (TBLB) are not sufficient for a definitive diagnosis [2]. BAL fluid typically displays a characteristic milky appearance. Lung histopathology typically shows diffuse, dense acellular eosinophilic material in the airways. Transbronchial lung cryobiopsy (TBLC) is when compressed gas released at high flow rates expands rapidly to create ultra-low temperatures, allowing large tissue samples to be taken in a freeze-thaw cycle [3]. TBLC is a diagnostic tool that shows high levels of agreement with surgical lung biopsy (SLB) in diagnosing interstitial lung disease (ILD) [4]. The utility and safety of TBLC for ILD other than SPAP are established, but they have been unclear for SPAP. A case of suspected ILD in which TBLC was performed and later diagnosed as SPAP is presented. Following TBLC, no apparent adverse events occurred, and good-quality specimens were obtained that contributed to the diagnosis. TBLC may be an effective biopsy method for patients with SPAP who previously required VATS.
Case presentation
A 66-year-old Japanese man with untreated stable follicular lymphoma was referred from the hematology clinic for investigation of abnormal findings detected incidentally. He smoked for 37 years and quit smoking when he was 57 years old. He worked in a granite mine for about 10 years and had been exposed to dust, granite, and iron. He had no symptoms of breathlessness at all. The chest X-ray showed ground-glass opacity in the lower lung field, and the chest CT showed reticular and ground-gross shadows extending along the bronchovascular bundles and just below the pleura in the lower lobes of both lungs (Figures 1A, 1B).
Chest X-ray and chest high-resolution computed tomography at initial examination.A: Chest X-ray showed ground-glass opacity in the lower lung field. B: Chest high-resolution computed tomography: reticular and ground-gross shadows extend along the bronchovascular bundles and just below the pleura in the lower lobes of both lungs.
Hospitalized for bronchoscopy due to suspected infection or pulmonary infiltration of lymphoma. On admission, his vital signs were a blood pressure of 153/96 mmHg, a temperature of 36.1°C, a pulse rate of 91 beats/min, a respiratory rate of 16 breaths/min, and a peripheral oxygen saturation of 96% in ambient air. Laboratory findings are presented in Table 1.
Arterial blood gas analysis showed that the partial pressure of arterial oxygen was 82.0 mmHg in ambient air (reference range, 80.0-100.0 mmHg). The following results were pulmonary function tests, forced vital capacity (FVC); 4.65 L (predicted value, 3.64 L), %FVC; 126.1%, forced expiratory volume in one second (FEV_1.0_); 3.82L (predicted value, 2.98 L), % FEV1.0; 128.6%, lung carbon monoxide diffusing capacity (DL_CO_); 13.94 mL/min/mmHg (predicted value, 15.93 mL/min/mmHg), and %DL_CO_; 92.9%.
BAL fluid (right lower lobe B_8_) was grossly mildly cloudy (Figure 2A), and cell counts were 1.2 x 10^6^/ml with 1% neutrophil, 85% lymphocyte, and 14% macrophage. Foamy macrophages were seen on cytology (Figure 2B). No significant bacteria were cultured in the BAL fluid.
Bronchoalveolar lavage fluid appearance and cytology.A: Bronchoalveolar lavage fluid appearance: mildly cloudy.B: Cytology of bronchoalveolar lavage fluid: foamy macrophages are observed, x20.
TBLC was performed by a 2.4-mm cryoprobe in the right lower lobe B9, twice times for biopsy, and the freezing time was five seconds each. Balloon occlusion was used for bleeding management, and no other additional procedures were performed for bleeding. Lung tissue, hematoxylin, and eosin stain revealed acidophilic granular structures in the alveolar region (Figure 3).
Lung tissue obtained by transbronchial lung cryobiopsyTransbronchial lung cryobiopsy: hematoxylin and eosin stain. (A) x4, (B) x10. Acidophilic granular structures were seen in the alveolar region (black arrows)
There were no complications associated with TBLC. No findings suggested pulmonary infiltration of lymphoma or infection. Based on the above, PAP was diagnosed. Serum granulocyte-macrophage colony-stimulating factor autoantibody was negative, and he was diagnosed with PAP secondary to lymphoma. Since the severity of SPAP was mild, he continued to be followed up without treatment. One year has now passed since SPAP diagnosis; his lymphoma has not worsened, and SPAP has spontaneously lightened (Figure 4).
Chest X-ray and chest high-resolution computed tomography at a year after diagnosisA: On the chest X-ray, ground-glass opacity was improved. B: Chest high-resolution computed tomography, ground-glass opacity with interlobular septal was improved.
Discussion
SPAP is commonly caused by hemopoietic disorders, immune dysregulation, infections, inhalation, lysinuric protein intolerance, and drug-induced or iatrogenic factors and is usually negative for serum granulocyte-macrophage colony-stimulating factor autoantibody [1,2]. Relying solely on serological tests to establish a diagnosis can be challenging, making it essential to obtain a definitive diagnosis to understand the underlying disease.
H. Ishii et al. reported that, among 40 patients with SPAP, a definitive diagnosis of SPAP was made using BAL in 21 cases, TBLB in nine cases, and VATS in 10 cases [2]. For some patients, BAL and TBLB are not sufficient for a definitive diagnosis of SPAP. Until now, SLB was the only option when BAL and TBLB were inadequate. It has been reported in the field of ILD that TBLC is less invasive than SLB and has a higher diagnostic yield than TBLB [4-6]. It is expected that more PAP cases could be diagnosed by performing TBLC in cases in which SLB cannot be performed.
Bleeding and pneumothorax are the common complications of TBLC [7]. According to a recent systematic review, TBLC for ILD had a higher bleeding risk than TBLB [8]. No reports of elevated bleeding or pneumothorax incidence could be found in patients with SPAP. In addition, a higher risk of infection after TBLC in patients with PAP is a concern because patients with PAP are susceptible to infections due to reduced neutrophil and macrophage function in the alveoli [9]. Inoue Y. et al. reported that 5.7% of patients with PAP in their Japanese cohort developed infections regardless of bronchoscopic procedures [10]. Azuma K. et al. reported that no patients with PAP developed fever after bronchoscopy, though 53.5% of patients with PAP were prophylactically prescribed oral antibiotics after bronchoscopy [11]. As noted earlier, the incidence of infection after TBLB is not high, but there are no such reports regarding TBLC. As neither pneumothorax, severe bleeding, nor infection were observed in the present case, we consider it feasible to perform TBLC in patients with SPAP.
Conclusions
We reported the case of TBLC for SPAP. SPAP is often challenging to diagnose due to the frequent absence of serum granulocyte-macrophage colony-stimulating factor autoantibody, and BAL and TBLB are often not enough to make the diagnosis. TBLC can be a valuable method to improve diagnostic accuracy in suspected cases. Although patients with PAP are known to have a higher risk of respiratory infections, TBLC may be feasible if conducted with adequate precautions. Even when SPAP is definitively diagnosed, treatment may not always be necessary. It is important to carefully monitor the progression of SPAP. Making a definitive diagnosis contributes to determining an appropriate treatment strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pulmonary alveolar proteinosis in adults: pathophysiology and clinical approach Lancet Respir Med Kumar A Abdelmalak B Inoue Y Culver DA 65554201810.1016/S 2213-2600(18)30043-229397349 · doi ↗ · pubmed ↗
- 2Clinical features of secondary pulmonary alveolar proteinosis: pre-mortem cases in Japan Eur Respir J Ishii H Tazawa R Kaneko C 4654683720112128281210.1183/09031936.00092910 · doi ↗ · pubmed ↗
- 3Transbronchial cryobiopsy: a new tool for lung biopsies Respiration Babiak A Hetzel J Krishna G Fritz P Moeller P Balli T Hetzel M 2032087820091924687410.1159/000203987 · doi ↗ · pubmed ↗
- 4Cryobiopsy versus open lung biopsy in the diagnosis of Interstitial lung disease alliance (COLDICE) investigators. Diagnostic accuracy of transbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): a prospective, comparative study Lancet Respir Med Troy LK Grainge C Corte TJ 81171202010.1016/S 2213-2600(19)30342-X 31578168 · doi ↗ · pubmed ↗
- 5Transbronchial cryobiopsies for diagnosing interstitial lung disease: real-life experience from a tertiary referral center for interstitial lung disease Respiration Wälscher J GroßB Eberhardt R 3483549720193055420110.1159/000493428 · doi ↗ · pubmed ↗
- 6Diagnostic yield of transbronchial cryobiopsy in interstitial lung disease: a randomized trial Respirology Pajares V Puzo C Castillo D 9009061920142489012410.1111/resp.12322 · doi ↗ · pubmed ↗
- 7Safety and performance of transbronchial cryobiopsy for parenchymal lung lesions Chest Herth FJ Mayer M Thiboutot J 1512151916020213397114710.1016/j.chest.2021.04.063 · doi ↗ · pubmed ↗
- 8Efficacy and safety of cryobiopsy vs. forceps biopsy for interstitial lung diseases, lung tumors, and peripheral pulmonary lesions: an updated systematic review and meta-analysis Front Med (Lausanne) Giri M Huang G Puri A Zhuang R Li Y Guo S 840702920223537245210.3389/fmed.2022.840702 PMC 8965605 · doi ↗ · pubmed ↗