Hydralazine-Induced Antineutrophilic Cytoplasmic Antibody (ANCA)-Associated Vasculitis Presenting as Crescentic Glomerulonephritis
Yoan E Rodriguez, Hovra Zahoor, Kunal Patel, Christian Castro Ruiz, Neda Shahoori

TL;DR
A patient developed a rare kidney condition linked to an autoimmune reaction after long-term use of hydralazine, a blood pressure medication.
Contribution
This case report highlights hydralazine as a potential cause of ANCA-associated vasculitis leading to crescentic glomerulonephritis.
Findings
Hydralazine therapy was associated with the development of ANCA-associated vasculitis.
The patient presented with crescentic glomerulonephritis as a result of the autoimmune reaction.
This case underscores the need to consider drug-induced vasculitis in patients with unexplained kidney issues.
Abstract
Hydralazine is a vasodilator medication commonly used for treating hypertension. While generally well-tolerated, in rare cases it can induce autoimmune reactions, including anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis. This case report presents a patient who developed ANCA-associated vasculitis resulting in crescentic glomerulonephritis (CrGN) following long-term hydralazine therapy, highlighting the importance of considering this rare adverse effect in patients with unexplained renal decline.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
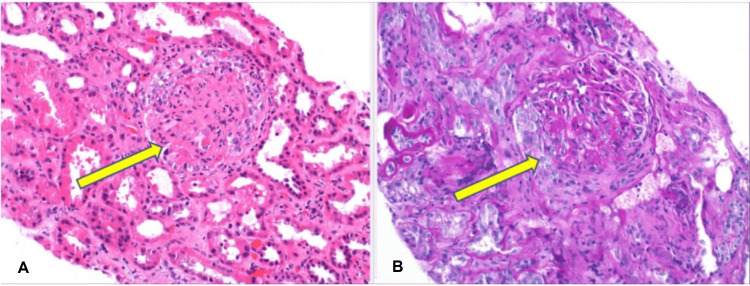 Figure 1
Figure 1| Values | Normal Range | |
| Sodium | 138 | 136-145 mMol/L |
| Potassium | 4.6 | 3.5-5.1 mmol/L |
| Chloride | 107 | 98-107 mMol/L |
| Carbon dioxide | 21.4 | 20.0-31.0 mEq/L |
| Blood urea nitrogen (BUN) | 77 | 9-23 mg/dL |
| Creatinine (Cr) | 5.77 | 0.55-1.02 mg/dL |
| Glucose | 157 | 74-106 mg/dL |
| Value | Normal Range | |
| Urine color | light-orange | yellow |
| Urine appearance | turbid | clear |
| Urine pH | 7.0 | 5.0-7.5 |
| Urine specific gravity | 1.010 | 1.015-1.030 |
| Urine protein | 2+ | negative |
| Urine ketones | negative | negative |
| Urine blood | 3+ | negative |
| Urine nitrite | negative | negative |
| Urine bilirubin | negative | negative |
| Urine urobilinogen | normal | normal |
| Urine leukocyte esterase | negative | negative |
| Urine RBC | >100 | negative |
| Values | Normal Range | |
| White blood cell count (WBC) | 5.5 | 4.0-10.5 x10^3/uL |
| Red blood cell count (RBC) | 2.17 | 3.93-5.22 10^6/uL |
| Hemoglobin (Hgb) | 6.2 | 11.2-15.7 g/dL |
| Hematocrit (Hct) | 20.9 | 34.1-44.9 % |
| Mean cell volume (MCV) | 96.3 | 79.4-94.8 fl |
| Mean cell Hemoglobin (MCH) | 28.6 | 25.6-32.2 pg |
| Mean cell Hemoglobin concentration (MCHC) | 29.7 | 32.2-35.5 g/dL |
| Red cell distribution width (RDW) | 16.1 | 11.7-14.4 % |
| Platelet count (Plt) | 208 | 150-400 10^3/uL |
| Mean platelet volume (MPV) | 10.2 | 9.4-12.3 fL |
| Serology | Values | Normal Range |
| Anti-histone antibodies | 5.8 | 0.0 – 0.9 units |
| Proteinase 3 (PR3) ANCA/c-ANCA antibodies | 1.3 | 0.0 – 0.9 AI |
| Myeloperoxidase (MPO) ANCA/p-ANCA antibodies | 8.0 | 0.0 – 0.9 AI |
| Anti-nuclear antibodies | negative | negative |
| Anti-double-stranded DNA antibodies | 2.0 | 0 – 4.9 iu/mL |
| Anti-glomerular basement membrane antibodies | <0.2 | <1.0 AI |
| Complement C3 | 77 | 90 – 180 mg/dL |
| Complement C4 | 15.8 | 14 – 44 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Renal Diseases and Glomerulopathies · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Hydralazine, a vasodilator used in the treatment of hypertension, is a rare cause of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) with pulmonary and renal involvement [1]. AAV is a pauci-immune inflammatory condition characterized by small vessel necrotizing vasculitis [2]. Crescentic glomerulonephritis (CrGN), is a severe form of glomerulonephritis and a common presentation of AAV, characterized by the destruction of the renal glomeruli often leading to end-stage renal disease (ESRD) [3]. The diagnosis of AAV relies on serologic studies for ANCA antibodies and tissue biopsy showing pauci-immune vasculitis. This case report highlights the importance of considering hydralazine-induced AAV in patients with unexplained renal decline and positive ANCA testing.
Case presentation
An 84-year-old female with a past medical history of type 2 diabetes mellitus, myasthenia gravis, and hypertension on hydralazine 100 mg twice a day for over one year presented with generalized weakness. She reported decreased urination but otherwise denied any other symptoms. The physical examination was unremarkable except for elevated blood pressure of 168/73 mmHg. Labs showed an elevated blood urea nitrogen (BUN) of 77 mg/dL and creatinine (Cr) of 5.77 mg/dL (Table 1), demonstrating an acute kidney injury with a baseline Cr of 1.3 prior to admission. Urinalysis revealed hematuria and proteinuria (Table 2). Complete blood count showed a decreased hemoglobin (6.2 g/dL) as shown in Table 3, which improved to 8.5 g/dL after one unit of packed red blood cells (pRBC) was transfused.
Serology was positive for anti-histone antibodies, proteinase 3 (PR3) ANCA antibodies, and myeloperoxidase (MPO) ANCA antibodies (Table 4). Negative anti-nuclear antibodies (ANA), anti-double-stranded DNA (dsDNA) antibodies, and anti-glomerular basement membrane (GBM) antibodies were noted (Table 4). There was decreased complement C3 while complement C4 was normal.
A renal biopsy was performed, and pathology showed necrosis and cellular/fibro-cellular crescent formation most consistent with ANCA-associated glomerulonephritis resulting in pauci-immune, necrotizing. and crescentic glomerulonephritis as shown in Figure 1.
Renal Biopsy(A) Hematoxylin and eosin (H&E) staining with fibrinoid necrosis and cellular crescent, which is indicated by the yellow arrow; (B) Fibro-cellular crescent, which is indicated by the yellow arrow.
Given the above lab results and hydralazine being the suspected triggering factor along with renal biopsy showing pauci-immune, necrotizing, and crescentic glomerulonephritis characteristic of ANCA-associated glomerulonephritis, a diagnosis of hydralazine-induced AAV was made.
Hydralazine was discontinued and the patient was treated with intravenous methylprednisolone 1 gm for three days followed by oral prednisone 60 mg daily. Rituximab therapy was planned, but the patient and her family, after extensive discussion and consideration of potential risks and benefits, opted to decline rituximab therapy due to concerns about potential side effects. The patient was discharged on maintenance prednisone with continuation of hemodialysis and instructed to follow up with nephrology as an outpatient.
Discussion
Hydralazine-induced AAV is a rare but serious complication of long-term hydralazine therapy [4]. Although the precise mechanism is unknown, it is believed to involve the drug triggering the formation of ANCA, which damages small blood vessels in different organs. Additionally, there is an increase in drug-induced AAV in females, those older than 60, and people who suffer from diabetes, heart failure, or pre-existing renal disease [1,5]. Even though the most likely diagnosis in this case was hydralazine-induced AAV with CrGN, it is crucial to take additional differential diagnoses into account to guarantee an accurate diagnosis and course of therapy. The distinction between anti-glomerular basement disease, idiopathic AAV, hydralazine‐induced lupus nephritis (HILN), and hydralazine‐induced AAV presents a diagnostic challenge for clinicians.
Anti-glomerular basement disease is characterized by the autoimmune development of antibodies towards type IV collagen in the GBM leading to rapidly progressive glomerulonephritis, but there should be evidence of anti-GBM antibodies in serum or histology, which was negative for our patient [6,7]. On the other hand, anti-histone and anti-dsDNA usually are absent in idiopathic AAV [8]. HILN is associated with low levels of C3 and C4 and positive ANA, anti-dsDNA, anti-Smith, and anti-histone antibodies [2,9]. In addition, kidney biopsy in lupus nephritis usually presents with immune complex deposits, endocapillary proliferation, wire loops, and hyaline thrombi [2]. Therefore, a biopsy could help to distinguish between the immunofluorescence patterns of lupus nephritis and hydralazine-induced AAV. Despite the possibility that HILN can present positive ANCA, the diagnosis of AAV was supported by the kidney biopsy's finding of pauci-immune glomerulonephritis rather than immune complex deposits and the absence of ANA, anti-dsDNA, and anti-Smith antibodies.
The initial step in the management of hydralazine-induced AAV should be the discontinuation of hydralazine, which can lead to the resolution of symptoms in mild cases. Treatment of severe cases with renal involvement requires immunosuppressive therapy such as steroids, cyclophosphamide, or rituximab [8]. Even with appropriate medical therapy, patients may still experience differences in their treatment response and progression and/or relapse of kidney disease. However, it is still essential to maintain a high index of suspicion to identify and treat hydralazine-induced AAV as soon as possible.
Conclusions
Early diagnosis and prompt withdrawal of the offending medication followed by immunosuppressive therapy to prevent further organ damage is crucial for hydralazine-induced AAV. While rituximab and/or cyclophosphamide are often recommended for severe AAV cases, respecting patient autonomy and collaboratively reaching a mutually agreeable treatment plan is vital to improve patient outcomes. This case highlights the importance of holding a high index of suspicion for hydralazine-induced ANCA vasculitis to prevent end-organ damage and initiate the therapy at the earliest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anti-neutrophil cytoplasmic antibody-associated glomerulonephritis secondary to hydralazine: a case report Cureus Abdullah A Anwar MS Ijaz M Karim MS Rosen R Bokhari SR 0142022 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 9840876/10.7759/cureus.32603 PMC 984087636654641 · doi ↗ · pubmed ↗
- 2Hydralazine-induced antineutrophil cytoplasmic antibody-associated vasculitis: asymptomatic and renal-restricted presentation Am J Case Rep Tu W Fayman B Ward SC Mamoon Y Bandagi SS 022202110.12659/AJCR.931263 PMC 814133433993184 · doi ↗ · pubmed ↗
- 3Crescentic glomerulonephritis: pathogenesis and therapeutic potential of human amniotic stem cells Front Physiol Al Mushafi A Ooi JD Odobasic D 7241861220213472105910.3389/fphys.2021.724186 PMC 8554237 · doi ↗ · pubmed ↗
- 4Hydralazine-induced vasculitis Cureus Gandhi P Khurana B Munjal RS Sekar A Gandhi RG 015202310.7759/cureus.35306 PMC 1004250236994251 · doi ↗ · pubmed ↗
- 5Hydralazine-induced anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis Cureus Echevarria V Pierre E Quiros J Eftekhari P 015202310.7759/cureus.47656 PMC 1066795538021694 · doi ↗ · pubmed ↗
- 6Anti-glomerular basement membrane disease in children: a brief overview Pediatr Nephrol Dowsett T Oni L 171317193720223476707510.1007/s 00467-021-05333-z PMC 8586640 · doi ↗ · pubmed ↗
- 7Anti-glomerular basement membrane vasculitis Autoimmun Rev Ponticelli C Calatroni M Moroni G 1032122220233625293110.1016/j.autrev.2022.103212 · doi ↗ · pubmed ↗
- 8Hydralazine-induced ANCA associated vasculitis (AAV) presenting with pulmonary-renal syndrome (PRS): a case report with literature review Curr Cardiol Rev Doughem K Battisha A Sheikh O Konduru L Madoukh B Al-Sadawi M Shaikh S 1821871720213241852810.2174/1573403 X 16666200518092814 PMC 8226194 · doi ↗ · pubmed ↗