Multiple Myeloma as a Potential Cause of Low Complements in Patients With Acute Kidney Injury
Kimberly Q Nguyen, Alexander Ting, Lorraine I Chong Tai, Philip Helderlein, Parham Eftekhari

TL;DR
This case report highlights multiple myeloma as a rare but possible cause of low complement levels in patients with acute kidney injury.
Contribution
It presents an atypical case linking multiple myeloma with hypocomplementemia and acute kidney injury.
Findings
A patient with multiple myeloma presented with acute kidney injury and low complement levels.
This case suggests that multiple myeloma should be considered in the differential diagnosis of hypocomplementemia with renal injury.
Such presentations are rare and may require increased clinical suspicion for accurate diagnosis.
Abstract
Multiple myeloma (MM) is a plasma cell malignancy belonging to the class of monoclonal gammopathies that leads to end-organ damage myeloma events that encompass anemia, the presence of lytic bone lesions, hypercalcemia, and renal insufficiency. However, there are very few reported cases of patients with low complements in the context of MM and renal failure. Traditionally, low complements in glomerular disease are associated with conditions such as membranoproliferative glomerulonephritis, cryoglobulinemia, systemic lupus erythematous, and post-infectious glomerulonephritis. Despite its rarity, physicians should maintain a high degree of suspicion and consider MM as a potential cause of low complements in patients with renal injury. In this case report, we present a patient with a history of MM associated with acute kidney injury with hypocomplementemia, an atypical presentation of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
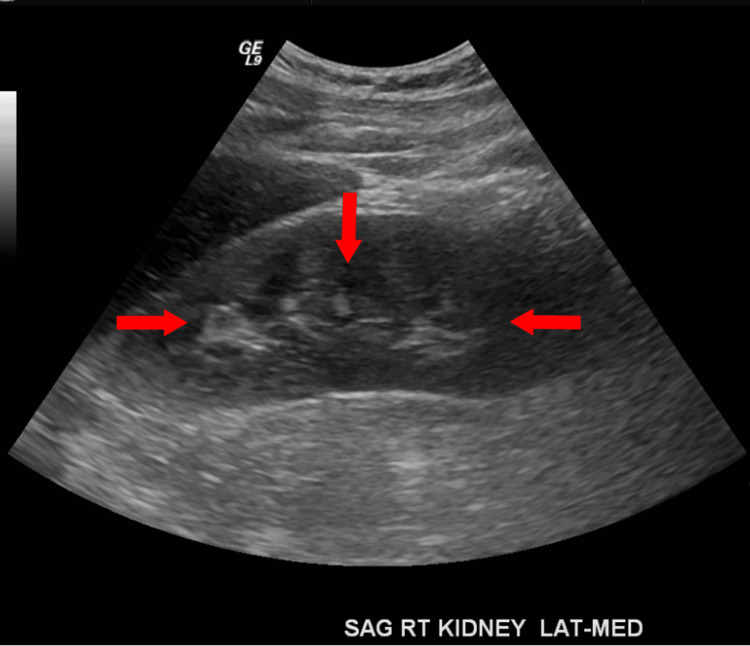 Figure 1
Figure 1| Laboratory results | Patient’s laboratory results | Reference range |
| Serum sodium level | 122 mmol/L | 135–145 mmol/L |
| Serum calcium level | 12.2 mg/dL | 8.5–10.3 mg/dL |
| Blood urea nitrogen | 25 mg/dL | 6–24 mg/dL |
| Creatinine | 2.3 mg/dL | 0.7–1.3 mg/dL for men |
| Hemoglobin level | 7.7 g/dL | 13.8–17.2 g/dL |
| Troponin level | 0.31 ng/mL | 0–0.04 ng/mL |
| Complement 3 level | 10 mg/dL | 88–201 mg/dL |
| Complement 4 level | 9 mg/dL | 13.8–17.2 mg/dL |
| Kappa/Lambda ratio | 71.42 | 0.26–1.65 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Complement system in diseases · Heparin-Induced Thrombocytopenia and Thrombosis
Introduction
Multiple myeloma (MM) is a plasma cell malignancy belonging to the class of monoclonal gammopathies that leads to end-organ damage myeloma events that encompass anemia, the presence of lytic bone lesions, hypercalcemia, and renal insufficiency [1]. End-organ damage events are referred to as myeloma-defining events and encompass anemia, the presence of lytic bone lesions, hypercalcemia, and renal insufficiency. Diagnostic markers include a clonal bone marrow plasma cell percentage greater than or equal to 60%, serum free light-chain ratio ≥100, or more than one focal lesion on MRI [2]. Kidney injury secondary to MM can result from a variety of factors, including cast nephropathy, monoclonal immunoglobulin (Ig) deposition disease, and amyloid light-chain amyloidosis. Less common mechanisms of injury encompass cryoglobulinemia, minimal change disease, thrombotic microangiopathy, and glomerulonephritis [3,4]. At a certain level, light chains can cause renal impairment due to abnormal deposition of complements [5]. The abnormal deposition of complements in the glomeruli can cause an abnormal activation of the alternative pathway of the complement system [6]. However, the association of hypocomplementemia with MM remains poorly understood besides cases of cryoglobulinemia. In this case report, we present a patient with a history of MM associated with acute kidney injury (AKI) with hypocomplementemia.
Case presentation
A 60-year-old male with a history of MM, currently in remission for the past three years, hypertension, asthma, and osteoarthritis initially presented to the emergency department due to an altered mental status that had persisted for one week. The physical examination was largely noncontributory, except for the noted confusion. The neurological examination was otherwise unremarkable. Vital signs on admission revealed a tachycardic patient with a heart rate of 126 beats per minute, a blood pressure of 166/100 mmHg, a respiratory rate of 20 respirations per minute, and an oxygen saturation of 95% on room air. Lab results showed a sodium level of 122 mmol/L, a calcium level of 12.2 mg/dL (corrected calcium level of 13.7 mg/dL), a troponin I level of 0.31, low complements, and a hemoglobin level of 7.7 g/dL (Table 1). Creatinine was 2.3 mg/dL, blood urea nitrogen was 25 mg/dL, and estimated glomerular filtration rate was 38 mL/minute/1.73m². A workup of hypocomplementemia revealed antinuclear antibodies, antineutrophilic cytoplasmic antibodies, anti-myeloperoxidase antibodies, antistreptolysin O, cryoglobulinemia, and anti-proteinase 3 antibodies were negative. The initial urinalysis revealed moderate hematuria consistent with acute nephritic syndrome, with 30 mg/dL of protein in the urine, six red blood cells (RBCs)/high-power field, three hyaline casts/low-power field, and RBC casts. The electrocardiogram was unremarkable, and the chest X-ray revealed stable interstitial infiltrates compared to a prior examination in 2017. Renal ultrasound showed an echogenic kidney consistent with chronic medical renal disease (Figure 1). The patient was transfused with two units of RBCs and received a bolus of normal saline before being admitted to the medicine service.
Renal ultrasound showing an echogenic kidney consistent with chronic medical renal disease (as indicated by arrows).
Nephrology was consulted for hyponatremia and AKI vs. AKI on chronic kidney disease. The patient’s original diagnosis of MM had been confirmed by a CT-guided bone biopsy of the left iliac crest on 05/09/2017. The biopsy demonstrated trabecular bone marrow with hypercellular packed marrow with a solid, atypical, increased plasma cellular infiltrate, comprising approximately 95%, with kappa restriction. Immunohistochemical stains were positive for CD-138 and kappa and negative for lambda. These morphologic and immunostaining patterns, in conjunction with the patient’s clinical history of multiple lytic bone lesions and IgG kappa monoclonal gammopathy, confirmed the diagnosis of MM. The patient’s last hospital admission in May 2017 showed no evidence of any kidney injury.
The impaired renal function was initially suspected to be due to cast nephropathy, prompting orders for kappa/lambda (K/L) ratio and urine-free light chain measurements. Urine protein and electrolytes were also ordered. The K/L ratio was elevated at 71.42, suggesting an element of kappa light chain cast nephropathy; however, the patient’s C4 and C3 complement levels were low at 9 mg/dL and 10 mg/dL on repeat labs, respectively. Blood cultures were negative, and no infection was suspected (Table 1). As the patient had nephritic pattern disease with low complements, we entertained a diagnosis of membranoproliferative glomerulonephritis (MPGN) and cryoglobulin renal disease. Of note, serum cryoglobulin was undetected and the patient refused renal biopsy. This prompted us to investigate medical literature on the significance of hypocomplementemia with MM and nephritic syndrome. Hypocomplementemia classically has been reported to be due to cryoglobulin and MPGN in MM. Despite not being able to perform a renal biopsy, we felt it was important to highlight medical literature and case reports of low C3 and C4 in MM.
The patient refused renal biopsy and thus was unable to set renal pathology. Ultimately, the patient’s clinical condition improved. Hypercreatinemia 1.9 trended downward and he was deemed stable for discharge to home. He was stable for discharge home with follow-up appointments in nephrology, hematology-oncology, and neurology. As the complement laboratory workup was negative for other potential sources of hypocomplements, we thought this was an interesting case.
Discussion
MM is a hematological cancer characterized by the clonal proliferation of malignant plasma cells that produce abnormal monoclonal Ig [1]. This condition results in hypercalcemia, osteolytic lesions, anemia, and renal insufficiency, with renal insufficiency having the most significant impact on overall survival among the four defining myeloma events [5,7].
Patients with MM may present with various glomerular and tubular manifestations. The pathogenesis of myeloma renal injury is due to the nephrotoxic effects stemming from the excessive production of monoclonal Igs and free light chains [8]. The most common renal injury in the context of myeloma is cast nephropathy. Less common renal complications in myeloma include various glomerulopathies, such as light-chain deposition disease and amyloid light-chain amyloidosis.
This case study focuses on a 60-year-old male with MM who had been in remission for three years. He was found to have kidney injury and hypocomplementemia and a bone marrow biopsy confirmed MM. Traditionally, low complements in glomerular disease are associated with conditions such as MPGN, cryoglobulinemia, systemic lupus erythematosus (SLE), and post-infectious glomerulonephritis. However, there are very few reported cases of patients with low complements in the context of MM and renal failure [6,9,10]. Serological workup in our patient was negative for cryoglobulins, SLE, and human immunodeficiency virus, and, unfortunately, the patient did not allow us to perform a renal biopsy. Abnormalities of complement activations in myeloma are not well understood besides conditions in MPGN and cryoglobulins. The defect in C3 activation and deposition, known as C3GN, likely plays a role in myeloma-related kidney injury [6,9,10]. The pathophysiology involves light chains binding to the complement regulator region of factor H, leading to abnormal activation of the alternative pathway of the complement system and subsequent abnormal deposition of complement C3 in the glomeruli, resulting in renal damage [6,9,10].
This case illustrates an atypical presentation of myeloma. Despite its rarity, physicians should maintain a high degree of suspicion and consider MM as a potential cause of low complements in patients with renal injury. Therefore, patients with renal injury in the context of MM and low complements should undergo renal biopsy to determine the type of renal pathology. Given the importance of rapidly reducing the excess serum free light chains for recovery of renal function, an aggressive therapeutic approach is justified in patients with myeloma renal injury [5].
Conclusions
Although the absence of a diagnostic renal biopsy presents a limitation in our ability to conclusively determine the etiology of hypocomplementemia in this patient with renal failure, clinicians should consider the novelty of hypocomplementemia in the setting of MM with AKI, and, if positive, further workup for diagnostic significance with renal biopsy and cryoglobulin levels. We highlight the importance of incorporating complement evaluations into the routine workup for MM-associated renal failure to further investigate causality. Recognizing that the etiology of renal failure associated with MM may extend beyond the common assumption of cast nephropathy, which is the most common manifestation. Clinicians are encouraged to take a proactive approach by challenging the automatic associated with cast nephropathy and broadening the spectrum of potential causative factors. This case report serves as a call to the medical community, emphasizing the need for clinicians to investigate low complements further in MM cases. This signals the need for a comprehensive evaluation and a departure from the conventional assumption of cast nephropathy as the primary manifestation of MM-associated renal failure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multiple myeloma N Engl J Med Palumbo A Anderson K 1046106036420112141037310.1056/NEJ Mra 1011442 · doi ↗ · pubmed ↗
- 2International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma Lancet Oncol Rajkumar SV Dimopoulos MA Palumbo A 04815201410.1016/S 1470-2045(14)70442-525439696 · doi ↗ · pubmed ↗
- 3Kidney disease and multiple myeloma Clin J Am Soc Nephrol Heher EC Rennke HG Laubach JP Richardson PG 20072017820132386889810.2215/CJN.12231212 PMC 3817918 · doi ↗ · pubmed ↗
- 4The spectrum of type I cryoglobulinemia vasculitis: new insights based on 64 cases Medicine (Baltimore) Terrier B Karras A Kahn JE 61689220132342935410.1097/MD.0b 013e 318288925 c PMC 4553985 · doi ↗ · pubmed ↗
- 5Multiple myeloma with acute light chain cast nephropathy Blood Cancer J Leung N Rajkumar SV 46132023 https://doi.org/10.1038/s 41408-023-00806-w 3699099610.1038/s 41408-023-00806-w PMC 10060259 · doi ↗ · pubmed ↗
- 6C 3 glomerulonephritis along with light chain proximal tubulopathy without crystal deposits in multiple myeloma: a case report World J Surg Oncol Xu J Yu X Wang S 24192021 https://doi.org/10.1186/s 12957-021-02135-33348280610.1186/s 12957-021-02135-3PMC 7824921 · doi ↗ · pubmed ↗
- 7Multiple myeloma: 2022 update on diagnosis, risk stratification, and management Am J Hematol Rajkumar SV 108611079720223556006310.1002/ajh.26590 PMC 9387011 · doi ↗ · pubmed ↗
- 8Nephrotoxic potential of Bence Jones proteins N Engl J Med Solomon A Weiss DT Kattine AA 184518513241991190413210.1056/NEJM 199106273242603 · doi ↗ · pubmed ↗