Missing Renal Stone Diagnosis in Dementia Patients With Recurrent Urinary Tract Infections: A Case Report and Literature Review
Sakshi Jain, Rashi Bharat Patel, Lovekumar Vala, SudhaRani Kinthada, Neel Patel, Shikha Jain, Tanzina Khan, Athmananda Nanjundappa, Vaishnavi Sirekulam, Nishthaben Naik, Chandu Siripuram, Harmeet Gill

TL;DR
An elderly dementia patient with recurring UTIs was found to have a kidney stone, highlighting the need for imaging in similar cases.
Contribution
This case report emphasizes the importance of imaging for kidney stones in dementia patients with recurrent UTIs.
Findings
A CT scan revealed an obstructed kidney stone as the cause of recurrent UTIs in a dementia patient.
Dementia patients with recurrent UTIs may require imaging to identify kidney stones.
Dehydration and poor oral intake in dementia patients increase the risk of kidney stones.
Abstract
In older adults, diagnosing, treating, and preventing urinary tract infections (UTIs) can be challenging. This case is of an 82-year-old female of white descent, who was admitted to a post-acute care facility following hospitalization for delirium and a UTI. Hypoactive delirium may be the only clinical manifestation of recurrent UTI. Due to challenges in obtaining a history from this patient with dementia, she had to be admitted multiple times for sepsis. During her final hospitalization, a CT scan of the abdomen and pelvis was ordered, which revealed an obstructed kidney stone as the cause of her recurrent UTIs. Recurrent UTIs especially in patients with dementia should prompt further imaging to look for kidney stones. Factors like dehydration and poor oral intake are risk factors for kidney stones, which patients with dementia are susceptible to.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
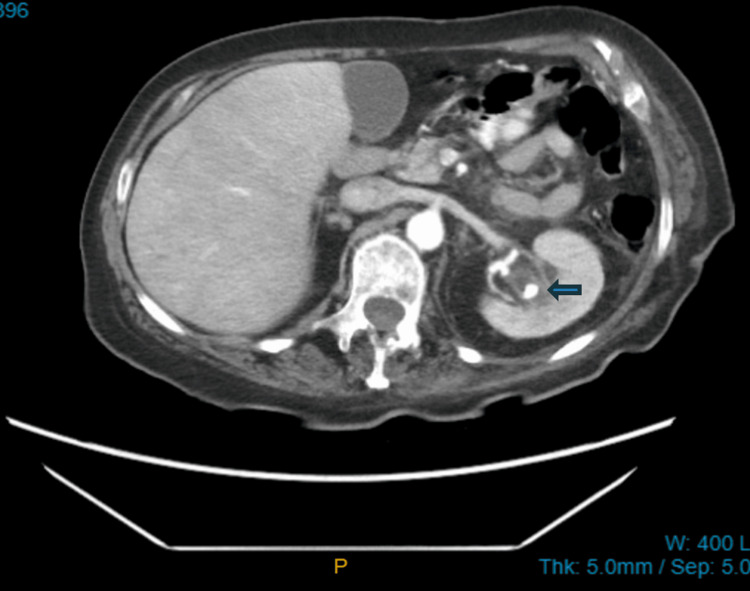 Figure 1
Figure 1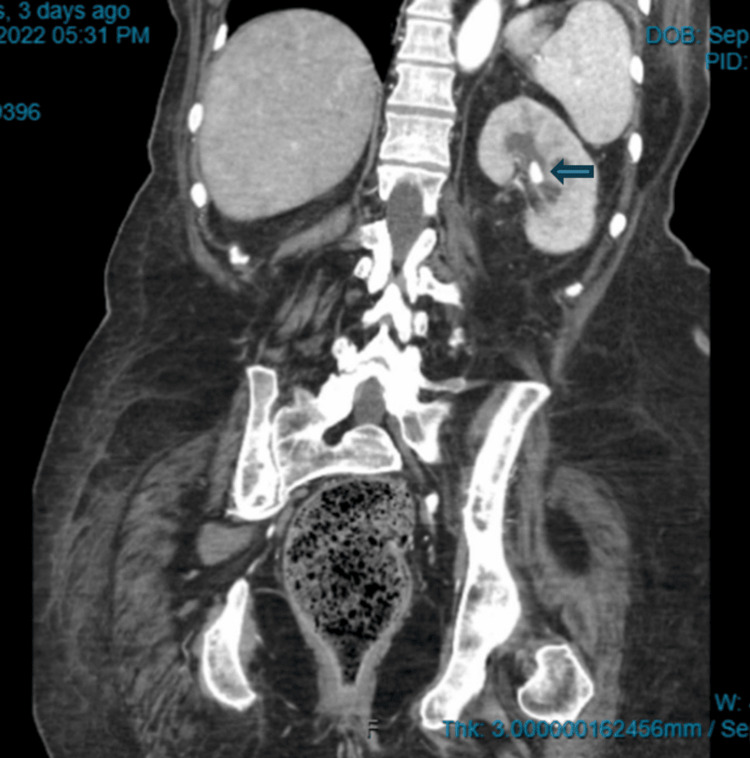 Figure 2
Figure 2| Study name | Demographics | Initial presentation | Diagnostic tests performed | Findings | Management/outcomes |
| Khalid et al., 2022 [ | A 60-year-old woman | A one-week history of fever with dysuria | KUB, HbA1c, CBC, CMP, urinalysis and urine culture, bladder ultrasound | KUB showed no mass or calculus in the bladder. It showed a simple cyst at the lower pole, measuring 1.9 x 1.8 cm. Lab results: serum creatinine = 1.48 mg/dl, HbA1c = 7.98. Ultrasound of the urinary bladder showed no presence of mass or calculus. Urine culture was positive for >100,000 CFU/ml of | Treated for atrophic vaginitis with estrogen cream topically for two weeks and cranberry tablets (475 mg) twice daily for one month. Received intravenous antibiotics piperacillin and tazobactam 4.5 g twice daily for five days. Prescribed fosfomycin 500 mg every eight hours for three months. |
| Nassour et al., 2013 [ | A 71-year-old woman | The patient presented with lethargy. | Urinalysis and urine culture | Urine culture with | Treated with intravenous ciprofloxacin for two days. She was discharged back to the nursing home on hospital day 4 with a prescription to take oral ciprofloxacin for three days. |
| Balouch et al., 2022 [ | A 91-year-old male | The patient presented with dysuria, urinary frequency, and urgency. | Urinalysis and urine culture | Urinalysis was positive for leukocyte esterase. Urine culture grew | He was treated with oral nitrofurantoin and subsequently recommended switching to a seven-day course of oral cephalexin. |
| Mukaya et al., 2016 [ | An 85-year-old man | A patient with dementia presented with a one-day history of agitation and confusion with complaints of urinary frequency, history of fever, and chills. | CBC, CMP, urinalysis, urine culture, CT scan of the abdomen and pelvis | Laboratory results revealed a creatinine level of 13.6 mg/dL, blood urea nitrogen of 245 mg/dL, potassium of 7.5 mEq/L, bicarbonate level of 17 mEq/L, anion gap of 23 mEq/L, and WBC count of 24,770/µL. Urinalysis revealed 100 white blood cells per high-power field and 3+ blood, although the urine culture result was negative. A CT scan of the abdomen and pelvis indicated a 5-mm calculus at the left vesicoureteric junction causing hydronephrosis and calyceal rupture. | Supportive care was provided, including a Foley catheter, intravenous fluids, and the management of electrolyte imbalances, particularly hyperkalemia. |
| Hur et al., 2016 [ | A 60-year-old Korean female | The patient presented with a fever of 38.6 °C accompanied by left-sided flank pain. | CBC, urinalysis, BUN and creatinine, CT scan of the abdomen | WBC was 15.24 × 109/L. Urinalysis showed a pH of 7, absence of nitrates, and 20–29 white blood cells per high-power field. The abdominal CT scan showed a 6-mm obstructive stone in the left renal pelvis, accompanied by left hydroureteronephrosis and thickening of the proximal ureter wall. The urine culture showed methicillin-resistant | The patient received intravenous ciprofloxacin, and the condition showed improvement after a seven-day course of ciprofloxacin. |
| Adhikari et al., 2022 [ | A 62-year-old female | The patient presented with 12 hours of urinary retention. She had a history of hesitancy at urination, increased frequency, interruption of the urinary stream, urgency, and a feeling of incomplete voiding for the last year. She had been complaining of mild, dull lower abdominal pain for the last six months. | CBC, urinalysis, urine culture, KUB, renal ultrasonography | Urinalysis indicated a very high white blood cell count and few red blood cells. Urine culture showed | Open cystolithotomy was performed under spinal anesthesia. She was treated with ciprofloxacin for |
| Elmanar et al., 2022 [ | A 53-year-old male | The patient complained of flank pain and had a history of kidney stones with no abdominal pain or fever. | Urinalysis, KUB, abdominal ultrasound, abdominal CT scan | Urinalysis showed hematuria and pyuria. The KUB showed ground-glass opacity at the left upper lower quadrant of the abdomen. Ultrasonography showed severe obstruction with pelvicalyceal system dilatation and echogenic material, suggesting pyelonephrosis. Abdominal CT showed thick fluid filling the left pelvicalyceal system, suggesting pyelonephrosis. | A percutaneous nephrostomy catheter was inserted, followed by a pus culture, resulting in Group B Streptococcus. The patient showed improvement after the administration of antibiotics. |
| Sandhu et al., 2018 [ | A 55-year-old male | The patient presented with nausea, vomiting, weakness, reduced urine output, and a pre-syncopal episode. | CBC, CMP, CT scan | The abdominal and pelvic CT scans revealed two obstructive stones, measuring 28 and 30 mm, located in the left proximal ureter, along with one obstructive stone measuring 30 mm in the right midureter. | He was diagnosed with acute renal failure from bilateral ureteral obstruction due to uric acid stones. A treatment of percutaneous chemolysis with potassium citrate and 3 amps (ampoule) of bicarbonate in a 20-cc (cubic centimeter) solution every six hours. By the fifth day of hospitalization, the majority of the stones had resolved, and a follow-up CT scan indicated the presence of only punctate, non-obstructing calculi. |
| Magro et al., 2019 [ | A 73-year-old male | The patient came in with a complaint of hematuria. He was seen a week prior for dysuria, urinary urgency, and two episodes of gross hematuria. | CBC, urinalysis, KUB, abdominal ultrasound, CT urogram | Urinalysis showed an acidic pH and the presence of erythrocytes in the urinary sediment, in the absence of nitrites and bacteriuria. The KUB showed bladder distension and several sub and pericentromeric calculi at the level of the medium calyceal group, to the right of the 10 mm stone. | Endoscopic lithotripsy was performed. At two months, it was noted that there were no new episodes of hematuria and improvement in urinary symptoms. |
| Agrawal et al., 2019 [ | A 56-year-old female | The patient presented with lower abdominal pain and dysuria for three days. She reported a history of multiple episodes of dysuria that had been treated with unspecified antibiotics for presumed urinary tract infections in the past six months in Mexico. | CBC, CMP, urinalysis, CT scan of the abdomen and pelvis | Laboratory findings revealed a WBC of 13,100 cells/μL with left shift. Urinalysis had positive leukocyte esterase, and there was no bacterial growth in the final urine culture. Non-contrast CT of the abdomen demonstrated a large calcified stone measuring 11 × 11 × 10.4 cm, nearly occluding the urinary bladder with bilateral hydroureter and hydronephrosis. | She was treated with piperacillin-tazobactam and bilateral percutaneous nephrostomy tube placement. On day 3, she underwent open vesicolithotomy and suprapubic tube placement with the removal of the stone. She was discharged due to improvement of kidney function and treated with a 10-day course of amoxicillin-clavulanate. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Urinary Tract Infections Management · Paleopathology and ancient diseases
Introduction
Recurring urinary tract infection (UTI) poses a considerable health concern, ranking as the second most prevalent infection among residents in nursing homes [1,2]. As per recent evidence, the prevalence of UTI ranges from 0.6% to 21.8%, with an incidence of 0.3 to 0.8 infections per 1000 resident care days [1]. It is estimated that UTIs cost at least US$2-3 billion per year in the United States [3]. The occurrence of UTIs is more prevalent among residents of nursing homes compared to the general population [4]. Recurrent UTIs in this vulnerable population can lead to severe morbidity, increased healthcare utilization, diminished quality of life, low morale, antibiotic resistance, and increased anxiety [5,6]. The diagnosis of UTIs in nursing home patients is challenging because of obstacles in communication, persistent genitourinary symptoms, and the presence of comorbidities. Understanding the causes and factors that lead to recurring UTIs and using effective diagnostic and treatment methods are necessary to improve the health of residents and to reduce the load on healthcare systems [7].
Many studies and guidelines have been developed for diagnosing UTIs in older adults. These include the revised McGreers criteria, which is a well-known protocol used to screen for infections in long-term care settings and help with diagnosis in patients who are cognitively impaired [8]. However, there is a lack of guidance on establishing the etiology of recurrent UTIs, such as kidney stones in patients with cognitive impairment. In high-risk older adults, insufficient oral intake and dehydration are significant factors that can trigger the development of kidney stones. Communication problems and atypical symptoms in this group of patients can make it hard to get a full history, which can cause a missed diagnosis of nephrolithiasis [9]. It is crucial to consistently investigate the root cause of recurrent UTIs, such as obstructive kidney stones, particularly in the presence of relevant risk factors like dehydration.
This case report and literature review provides the clinical course of a nursing home resident with recurrent UTIs, concentrating on key aspects, such as the patient's cognition, clinical presentation, diagnostic evaluation, management, and outcomes. The development of a diagnostic algorithm is suggested to determine the underlying causes of recurrent UTIs, one of them being kidney stones in older adults especially those with dementia.
This article was previously presented as a meeting abstract at the 2023 American Geriatrics Society Scientific Meeting on May 5, 2023.
Case presentation
A post-acute care facility admitted an 82-year-old female of white descent after her hospitalization for delirium and a UTI. Although she underwent rehabilitation, her limited progress in therapy and concurrent dementia necessitated long-term care. The patient consistently denied pain or dysuria during her hypoactive delirium episodes. She seldom spiked a fever and labs always showed mild leukocytosis. Two episodes were treated with antibiotics at the facility. However, the challenges of obtaining a comprehensive history from this patient with dementia, combined with atypical symptoms, also resulted in multiple hospitalizations for sepsis due to delayed diagnoses over a span of six months.
UTI diagnosis was made at each hospital admission with a positive urinalysis (UA), urine culture, and leukocytosis seen in her blood work. Each admission involved intravenous antibiotics, intravenous fluids, and a discharge back to the facility. She was hospitalized three times. Her fourth hospitalization for yet another UTI diagnosed with a UA and urine culture prompted further action leading the nursing home attending provider to contact the hospitalist for computed tomography (CT) of the abdomen and pelvis. The CT scan of the abdomen and pelvis revealed a left-sided kidney stone that was obstructed, as shown in Figure 1 and Figure 2. Urology was consulted, and this was managed through cystoscopy and ureteral stent placement. Urology recommended outpatient nephrostomy tube placement, and the patient returned to the nursing home. Post-hospitalization, the patient remained stable with no UTI recurrence, no delirium, and no further hospitalizations for sepsis.
Axial view CT scan abdomen and pelvis showing left-sided nephrolithiasisThe blue arrow demonstrates a large calcified stone measuring 11 × 11 × 10.4 cm.
Coronal view CT scan of the abdomen and pelvis showing left-sided nephrolithiasisThe blue arrow demonstrates a calcified stone measuring 11 × 11 × 10.4 cm.
Discussion
Older adults can present with atypical symptoms of UTI, but not many studies have looked into how common atypical presentations are and what factors are linked to them [9]. The clinical range of UTIs extends from asymptomatic bacteriuria to symptomatic and recurrent cases. In severe instances, it can lead to sepsis necessitating hospitalization [10]. UTIs rank among the most prevalent infections, impacting nearly 50% of women during their lifetime, and about half of these women encounter a recurrence within six to 12 months [11]. One systematic literature review explored the association between recurrent UTIs and kidney stones and found that they can be mutually coexistent when risk factors are present [12]. This case report showcases the diagnostic challenges in patients with cognitive dysfunction and the importance of imaging investigations in assessing the underlying cause of recurrent UTIs.
Since delirium might be the only presenting symptom in older adults, an unreliable history makes diagnosing kidney stones extremely challenging. They might present with acute functional or cognitive decline. Potential explanations for this atypical presentation include the presence of cognitive impairment, such as dementia or delirium, which hinders obtaining a reliable medical history [13]. A systematic review supports the evidence that patients suffering from kidney stone disease often present with recurrent or concomitant urinary tract infections [14]. Table 1 describes previously published case reports with demographics, initial presentation, diagnostic tests, findings, and management of patients with UTI and some with UTI and kidney stones.
All case reports are of older adults 50 years and above. All patients in the younger age group between ages 50-69 were able to relay a history and presented with typical signs and symptoms of fever, elevated white blood cell count, dysuria, or flank pain. Two patients in the case reports by Nassour et al. [15] and Mukaya et al. [17] above age 70 presented with atypical symptoms of lethargy, confusion, and agitation. Of these two cases, only the 85-year-old patient with dementia had some typical symptoms of urinary frequency, fever, and chills, which prompted a CT abdomen and pelvis showing a kidney stone. The 71-year-old frail nursing home resident who was unable to provide a reliable history did not receive further imaging despite having risk factors for dehydration and poor oral intake.
Recurrent UTIs in older adults with or without cognitive dysfunction having appropriate risk factors of dehydration should prompt a high degree of suspicion for kidney stones even in the absence of typical signs and symptoms. A diagnostic algorithm should be proposed for appropriate diagnosis and management of recurrent UTIs with further imaging in the older population to prevent recurrent admissions, debility, morbidity, and mortality.
Conclusions
Diagnosis of nephrolithiasis is challenging in older adults especially those with dementia due to an asymptomatic or atypical presentation. Patients with dementia are at an increased risk of poor oral intake and dehydration and therefore have a higher risk of developing kidney stones. This case report highlights the importance of further investigation for kidney stones in older adults presenting with recurrent UTIs with risk factors of dehydration who are unable to provide a reliable history and physical exam. The formation of a diagnostic algorithm is necessary to help healthcare providers determine the underlying cause of recurrent UTIs such as kidney stones in older adults with dementia. This will help to prevent morbidity, mortality, and unnecessary hospitalizations in this complex and frail population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Urinary tract infections in older adults residing in long-term care facilities Ann Longterm Care Genao L Buhr GT 3338202012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 3573848/23418402 PMC 3573848 · pubmed ↗
- 2Chapter 32: Urinary tract infections in elderly persons Geriatric Nephrology Curriculum Juthani-Mehta M 14Philadelphia Lippincott 2009 https://www.asn-online.org/education/distancelearning/curricula/geriatrics/Chapter 32.pdf
- 3Urinary tract infections in the elderly: a review of disease characteristics and current treatment options Drugs Context Rodriguez-Mañas L 9202010.7573/dic.2020-4-13PMC 735768232699546 · doi ↗ · pubmed ↗
- 4Antimicrobial use in long-term-care facilities. SHEA Long-Term-Care Committee Infect Control Hosp Epidemiol Nicolle LE Bentley DW Garibaldi R Neuhaus EG Smith PW 5375452120001096872410.1086/501798 · doi ↗ · pubmed ↗
- 5Relationship of lifestyle and clinical factors to lower urinary tract symptoms: results from Boston Area Community Health survey Urology Litman HJ Steers WD Wei JT Kupelian V Link CL Mc Kinlay JB 9169217020071791969310.1016/j.urology.2007.06.1117 PMC 2194647 · doi ↗ · pubmed ↗
- 6Long-term antibiotics for prevention of recurrent urinary tract infection in older adults: systematic review and meta-analysis of randomised trials BMJ Open Ahmed H Davies F Francis N Farewell D Butler C Paranjothy S 07201710.1136/bmjopen-2016-015233 PMC 572998028554926 · doi ↗ · pubmed ↗
- 7Risk factors and predisposing conditions for urinary tract infection Ther Adv Urol Storme O Tirán Saucedo J Garcia-Mora A Dehesa-Dávila M Naber KG 11201910.1177/1756287218814382 PMC 650298131105772 · doi ↗ · pubmed ↗
- 8Surveillance definitions of infections in long-term care facilities: revisiting the Mc Geer criteria Infect Control Hosp Epidemiol Stone ND Ashraf MS Calder J 9659773320122296101410.1086/667743 PMC 3538836 · doi ↗ · pubmed ↗