Fluctuating hypermetropia due to intraocular lens displacement caused by iris pigment epithelial cyst
Kirupakaran Arun, Nizar Din, Miles Stanford, Victoria Cosgrove, Mukhtar Bizrah

TL;DR
A man's vision worsened after lens surgery due to an enlarging eye cyst that shifted his implanted lens, but the issue improved as the cyst shrank over time.
Contribution
This is the first reported case of an iris pigment epithelial cyst growing after intraocular surgery, causing a hyperopic shift.
Findings
An enlarging iris pigment epithelial cyst displaced an intraocular lens, causing a hyperopic shift.
The cyst spontaneously regressed over 30 months, allowing the lens to return to a normal position.
Visual acuity and refraction improved following the cyst's reduction.
Abstract
To report a case of hyperopic shift following lens replacement surgery due to an enlarging iris pigment epithelial (IPE) cyst. A gentleman presented with reduced visual acuity (Snellen unaided 20/25) 12 months followed lens replacement surgery. Examination revealed a retro-pupillary iris lesion that appeared to be displacing the posterior chamber intraocular lens (IOL) and was causing a hyperopic shift (refraction +2.00). Anterior segment optical coherence tomography imaging confirmed this to be an IPE cyst with a posteriorly displaced IOL body. After observation over 30 months, the IPE cyst spontaneously reduced in size and the IOL returned to a more physiological position. Unaided visual acuity improved to Snellen 20/16 and refraction improved to +0.50. To our knowledge, an IPE cyst that shows growth following intraocular surgery has not previously been reported. This growth…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
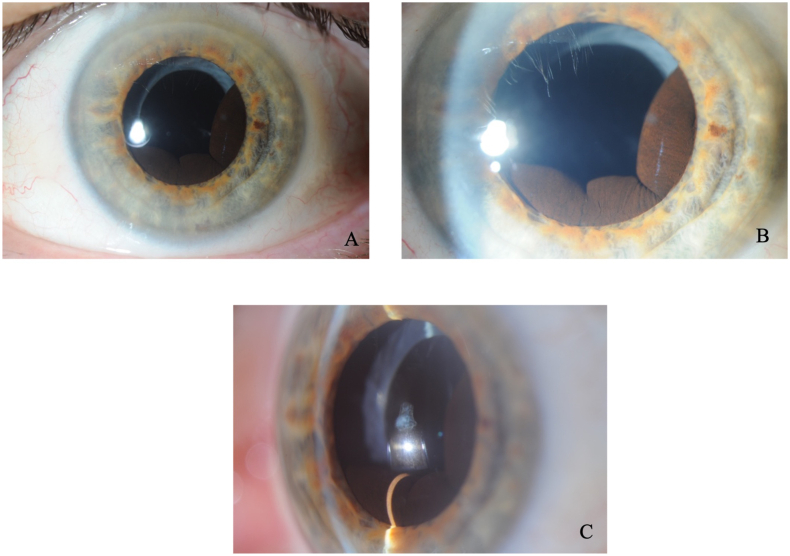 Figure 1
Figure 1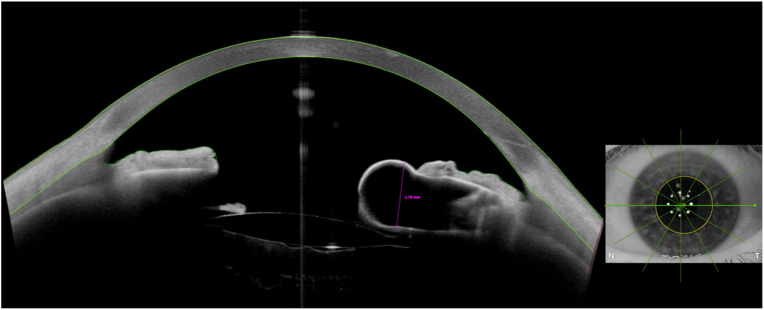 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Oncology and Treatments · Glaucoma and retinal disorders · Retinal and Macular Surgery
Introduction
1
Primary iris pigment epithelial (IPE) cysts commonly are asymptomatic and are stationary or very slow-growing.1 Secondary iris cysts are less common but are more prone to causing complications including reduced vision, glaucoma and uveitis.2 We report a unique case of a gentleman who presented with posterior intraocular lens (IOL) displacement due to a large IPE cyst behind the iris.
Case report
2
A 66-year-old male presented to the outpatient department due to blurred vision in his left eye following lens replacement surgery with a standard monofocal intraocular lens. He had a past ocular history of bilateral LASIK (laser-assisted in situ keratomileusis) for hypermetropia and more recent bilateral lens replacement surgery. On examination, the Snellen unaided visual acuity was 20/20 and 20/40, respectively on the right and left eyes. Left eye vision improved to 20/20 with pinhole. Autorefraction was +0.25/-1.00 × 35 on the right eye and +2.00/0.00 × 180 on the left eye. Intraocular pressures were normal in both eyes. The right eye anterior and posterior examination was unremarkable. However, the left examination revealed a clear cornea, quiet anterior chamber with a retro-pupillary iris mass lesion from 2 to 9 o clock (Fig. 1 A, B and C). Posterior segment examination of the left eye was normal.Fig. 1(A): Slit lamp photograph (low magnification) of the left eye showing a retro-pupillary iris lesion through dilated pupil. (B): Slit lamp photograph (high magnification) of same lesion through dilated pupil (C): Slit lamp photograph showing iris lesion protruding posterior to pupillary plane.Fig. 1
High-resolution anterior segment optical coherent tomography (AS-OCT) imaging of the left eye further demonstrated this lesion. It measured 1.78mm in thickness with internal lucency and was seen protruding from the posterior iris and causing posterior displacement of the posterior chamber IOL (Fig. 2).Fig. 2. Anterior segment optical coherence tomography images of the left eye showing a typical retro-pupillary iris cyst (1.78mm thickness).Fig. 2
A diagnosis of left midzonal IPE cyst was made. This was causing a hyperopic shift from posterior displacement of the posterior chamber IOL. On further questioning, the patient did recollect being told at the time of his left lens replacement surgery that there was a small iris cyst, but this did not affect surgery in any way.
With regards to treatment options, the patient enquired about further laser refractive surgery to correct the hypermetropia. Due to the seemingly sudden increase in size of the iris cysts post lens replacement surgery, we recommended spectacle/contact lens to correct the hypermetropia in the first instance and arranged a further review in the clinic to monitor the cyst.
Four months later, the patient attended for a follow-up appointment. Unaided vision in the left eye had spontaneously improved to Snellen 20/25 and refraction had improved to +1.25/0.00 × 180. On examination, the left iris pigment epithelial cyst had become visibly smaller. As the cyst had become spontaneously smaller and unaided vision and refraction had improved, we decided on surveillance monitoring over any intervention to remove the cyst.
The patient was reviewed again twelve months following the initial presentation. The iris cyst had decreased in size. Vision in the left eye had further improved to Snellen 20/16 unaided and refraction had improved to +0.75/-0.50 × 144.
Humphrey visual fields remained full in both eyes with normal intraocular pressures and healthy optic nerves. Over 2.5 years later following initial presentation, his visual acuity remains Snellen 20/16 unaided with plano refraction.
Discussion
3
Iris cysts are uncommon and can be classified as primary or secondary according to aetiology, and then further divided into subgroups based on their tissue or origin, with primary IPE cysts representing 86 % of all iris cysts.4
Primary IPE cysts are thought to be remnants of the marginal sinus that have not been obliterated and represent developmental anomalies resulting from the cystic expansion of the potential space between the pigmental epithelial layers of the posterior iris.3 Histopathology of primary IPE cysts is composed of nonkeratinized squamous epithelial-lined structures that arise from the posterior iris layer.5
Primary IPE cysts are usually an incidental finding. Primary IPE cysts can be classified based on their location: pupillary, midzone, peripheral and free-floating/dislodged.6 In terms of incidence, peripheral IPE cysts are most common (64 %), followed by midzone (28 %), pupillary (7 %) and dislodged (1 %).7
The clinical course of primary IPE cysts is dependent on their location.1 Peripheral, midzone and dislodged IPE cysts tend to remain stable, regress in size or completely resolve. However, pupillary IPE cysts are more likely to enlarge over time (84 %), with the remainder tending to remain stable in size (8 %) or completely resolve (8 %).7 Interestingly, our patient had a midzone IPE cyst that did show initial enlargement, followed by regression.
Despite this, in the largest primary IPE surveillance study conducted, no complications were detected with pupillary IPE cysts.7 Instead, complications were more seen with midzone and peripheral IPE cysts and these included corneal touch, focal cataract, lens subluxation, iritis and glaucoma.7
Imaging modalities such as ultrasound biomicroscopy and AS-OCT are essential in differentiating iris cysts from ocular tumours. IPE cysts appear as thin-walled and homogeneous lesions with hypoechoic internal content and regular borders on UBM and AS-OCT,8 whilst tumours present with a solid inner structure9 and show increase in lesion size.10 Based on the history, examination and AS-OCT, our patient had a left midzonal primary IPE cyst.
It seems that there was transient enlargement of the IPE cyst in our patient following lens replacement surgery, and this caused the IOL body to displace posteriorly and produce a hyperopic shift (he was emmetropic after his lens extraction). The lack of astigmatism change is somewhat peculiar as the asymmetrical pressure on the IOL body from the transient IPE cyst enlargement would be expected to produce some change in astigmatism. On examination, the IOL was well-centred. There was evidence of posterior displacement, but no evidence of decentration or tilt. This would explain the change in spherical refractive error, but no induction of cylindrical error.
There is clear evidence that trauma,2 inflammation1 and even certain glaucoma medication such as latanoprost11 can stimulate the formation of secondary iris cysts. However, the possible pathogenic mechanism underlying enlargement of primary IPE cysts is still unclear and there are no reports of enlargement/reduction in size of primary IPE cysts being linked to intraocular surgery.12 Furthermore, the two largest IPE surveillance studies7^,^8 did not identify intraocular surgery as a risk factor for cyst enlargement. There are reports of secondary iris cysts (following lens extraction surgery) growing and causing the IOL body to become posteriorly displaced with subsequent hyperopic shift.13, 14, 15
There is very limited literature to show that primary iris cysts have any effect on posterior chamber “in-the-bag” IOLs as our case showed. However, there is some data on how iris cysts affect the position of implantable collamer lenses (ICLs). One study reported a case series of 218 eyes with iris cysts and found no abnormal effects on ICL position, vault or astigmatism over 12 months.16 Another study showed no difference in the ICL position, central vault of ICL and refractive error following ICL implantation between eyes with and without primary iris cysts.17 Similar to what occurred in our case, both these studies found that most cysts regress in size or resolve within 12 months of ICL surgery. In our patient, the IPE cyst spontaneously decreased in size, allowing the IOL to return to a more physiological position, thus reducing the hypermetropic refractive error and improving the unaided distance visual acuity over the 2.5 year period.
Our case report suggests that refractive surgery would not be a suitable option because of the changing iris cyst size. Non-permanent methods such as spectacles or contact lenses may be preferred. If a more permanent treatment is sought, then treatment of the IPE cyst rather than refractive surgery may be advisable.
Conclusion
4
We report a case of a patient who developed a hyperopic shift following lens replacement surgery due to an IPE cyst. The IPE cyst caused a hyperopic shift due to a substantial increase in size (following lens replacement surgery) that led to displacement of the IOL posteriorly. Over the following months and years, the iris cyst shrunk spontaneously and the unaided visual acuity and refraction improved without any intervention.
Patient consent
Consent to publish the care report was obtained. This report does not contain any personal information that could lead to the identification of the patient.
Acknowledgments and disclosures
No funding or grant support.
The following authors have no financial disclosures: KA, ND, VC, MB.
All authors attest that they meet the current ICMJE criteria for Authorship.
CRediT authorship contribution statement
Kirupakaran Arun: Writing – original draft. Nizar Din: Writing – review & editing, Supervision. Miles Stanford: Writing – review & editing. Victoria Cosgrove: Data curation. Mukhtar Bizrah: Conceptualization, Data curation, Supervision, Writing – review & editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Georgalas I.Petrou P.Papaconstantinou D.Brouzas D.Koutsandrea C.Kanakis M.Iris cysts: a comprehensive review on Diagnosis and treatment Surv Ophthalmol 633201834736410.1016/j.survophthal.2017.08.00928882598 · doi ↗ · pubmed ↗
- 2Hildreth T.Maino J.Hartong T.Primary and secondary iris cysts J Am Optom Assoc 6281991 Aug 5885921813566 · pubmed ↗
- 3Shields J.A.Primary cysts of the iris Trans Am Ophthalmol Soc 7919817718097342411 PMC 1312203 · pubmed ↗
- 4Shields C.L.Kancherla S.Patel J.Clinical survey of 3680 iris tumors based on patient age at presentation Ophthalmology 11922012 Feb 40741410.1016/j.ophtha.2011.07.059Epub 2011 Oct 2722035581 · doi ↗ · pubmed ↗
- 5Dubey Suneeta 1Pegu Julie 1Jain Kanika 2Iris cysts: varied presentations and review of literature Saudi Journal of Ophthalmology 354Oct–Dec 202134134610.4103/sjopt.sjopt_228_2135814992 PMC 9266481 · doi ↗ · pubmed ↗
- 6Shields J.A.Kline M.W.Augsburger J.J.Primary Iris cysts: a review of the literature and report of 62 cases Br J Ophthalmol 683198415216610.1136/bjo.68.3.1526696869 PMC 1040279 · doi ↗ · pubmed ↗
- 7Lois N.Shields C.L.Shields J.A.Mercado G.Primary cysts of the iris pigment epithelium. Clinical features and natural course in 234 patients Ophthalmology 105101998 Oct 1879188510.1016/S 0161-6420(98)91034-X 9787358 · doi ↗ · pubmed ↗
- 8Köse H.C.Gündüz K.Hoşal M.B.Iris cysts: clinical features, imaging findings, and treatment results Turk J Ophthalmol 5012020 Mar 5313610.4274/tjo.galenos.2019.20633 PMID: 32167261; PMCID:32167261 PMC 7086092 · doi ↗ · pubmed ↗