A Case of Recurrent Sputum-Positive Pulmonary Tuberculosis Presenting With Pulmonary Mycetoma
Adinath Gaikwad, Pankaj Wagh, Souvik Sarkar, Mansi Khare

TL;DR
This case study presents a rare instance of a tuberculosis patient who also developed pulmonary mycetoma, highlighting the importance of accurate diagnosis to avoid severe health outcomes.
Contribution
The paper highlights a rare co-infection of tuberculosis and mycetoma, emphasizing the need for differential diagnosis to prevent mismanagement.
Findings
The patient's failure to continue anti-tubercular medication led to disease recurrence.
Combination therapy with anti-tubercular drugs and itraconazole was initiated.
Surgical excision is recommended over pharmacotherapy for mycetoma in tuberculosis patients.
Abstract
Pulmonary tuberculosis is a notorious disease as it can cause severe morbidity and mortality. In this case, we discuss a 75-year-old male tuberculosis patient from a rural area with no underlying comorbidities who failed to continue anti-tubercular medication after two months. The case discusses the diagnostic modalities confirming the diagnosis, sputum culture for Mycobacterium tuberculosis, imaging studies, including X-ray and CT of the chest, and laboratory parameters for identifying pulmonary mycetoma. The patient is now on anti-tubercular therapy (isoniazid, rifampicin, pyrazinamide, and ethambutol combination) and the anti-fungal drug itraconazole. Though pharmacotherapy for the treatment of mycetoma in patients with tuberculosis has a minimal role, the more appropriate treatment is surgical excision via lobectomy. As the occurrence of tuberculosis and mycetoma is a rare…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
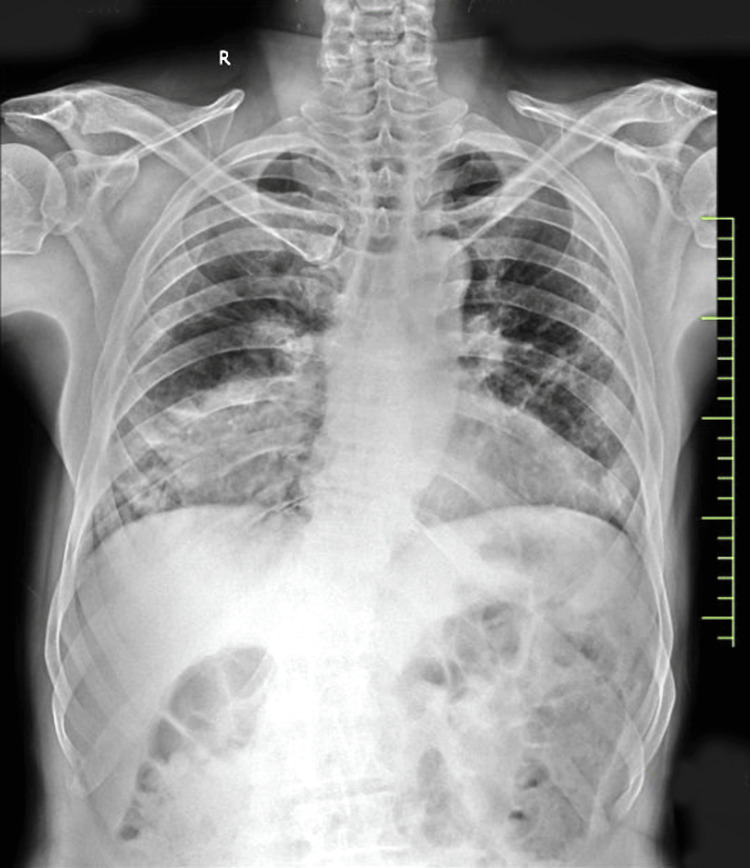 Figure 1
Figure 1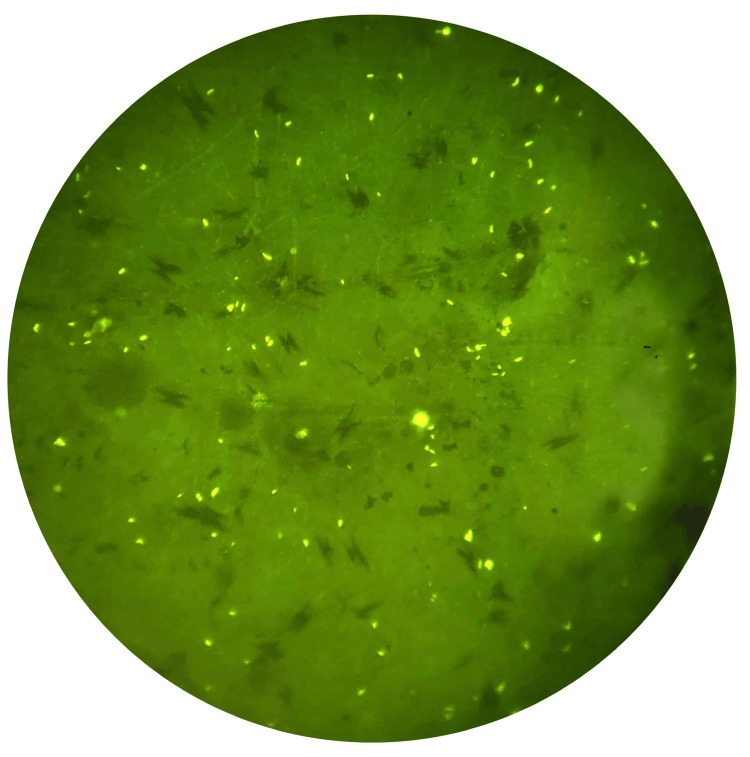 Figure 2
Figure 2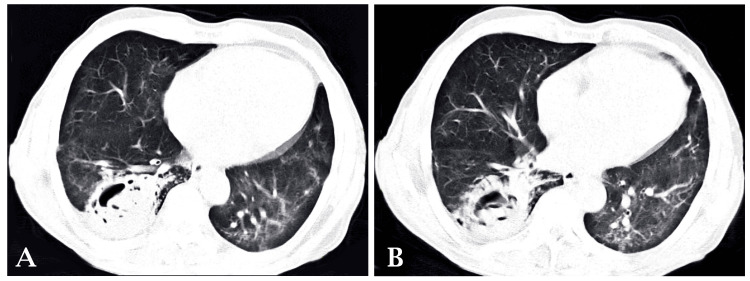 Figure 3
Figure 3| Lab variables | Results | Reference range |
| Hemoglobin (g/dL) | 9.3 | 12–16 |
| MCHC (g/dL) | 31.7 | 31–35 |
| MCV (fL) | 75.9 | 76–100 |
| MCH (pg/cell) | 24.1 | 25–32 |
| Total RBC count (million cells/mm3) | 3.88 | 0–1.070 |
| Total WBC count | 7,900 | 3,500–9,000 |
| Total platelet count (× 105) | 3.99 | 1.5–4.5 |
| Hematocrit (%) | 29.5% | 42–53 |
| Granulocytes ((× 109) | 5.5 | 1.5–8.5 |
| Lymphocytes (%) | 40 | 25–45 |
| RDW (%) | 18.1 | 11.5–14.5 |
| Monocytes (%) | 04 | 3–7 |
| Eosinophils (%) | 01 | 1–3 |
| Basophils (%) | 00 | 0–0.75 |
| Lab variables | Results | Reference range |
| Liver function test | ||
| Alkaline phosphatase (U/L) | 100 | 53–128 |
| SGPT (U/L) | 11 | 7–56 |
| SGOT (U/L) | 20 | 8–33 |
| Total protein (g/dL) | 8.3 | 6.0–8.3 |
| Albumin (g/dL) | 3.2 | 3.4–5.4 |
| Globulin (g/dL) | 5.1 | 2.0–3.5 |
| A/G ratio serum | 0.62 | 1.3–2 |
| Total bilirubin (mg/dL) | 0.5 | 0.1–1.0 |
| Conjugated bilirubin (mg/dL) | 0.2 | 0–0.3 |
| Unconjugated bilirubin (mg/dL) | 0.3 | 0.2–0.8 |
| Kidney function test | ||
| Urea (mg/dL) | 28 | 6–24 |
| Creatinine (mg/dL) | 1.1 | 0.5–1.5 |
| Sodium (Na+) serum (mEq/L) | 139 | 135–145 |
| Potassium (K+) serum (mEq/L) | 4.5 | 3.5–5.0 |
| Other relevant tests | ||
| Calcium serum (mg/dL) | 8.4 | 8.4–10.2 |
| Magnesium (mg/dL) | 1.7 | 1.5–2.0 |
| Phosphorus serum (mg/dL) | 5.0 | 2.8–4.5 |
| Anti-HCV (rapid) | Non-reactive | - |
| HbsAg (rapid) | Non-reactive | - |
| HIV (rapid) | Non-reactive | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and treatment of tuberculosis · Actinomycetales infections and treatment · Sarcoidosis and Beryllium Toxicity Research
Introduction
The co-infection of pulmonary tuberculosis and aspergillosis is rare [1]. Pulmonary aspergillosis has various presentations, including allergic bronchopulmonary aspergillosis, mycetoma, necrotizing *Aspergillus *pneumonia, and invasive aspergillosis [2]. When a patient presents with tuberculosis, it is sometimes possible to miss an *Aspergillus *infection as the clinical symptoms are similar (hemoptysis, weight loss, fever, and night sweats). Furthermore, a misdiagnosis could be made due to a lack of clinical suspicion, and, most crucially, the infection is chronic enough to be confused with pulmonary tuberculosis [3].
Case presentation
A 75-year-old male patient from a rural area with no underlying comorbidities was diagnosed with pulmonary tuberculosis two years ago, for which he had taken anti-tubercular therapy (ATT) for two months only and then stopped the medication. He presented to us with the chief complaints of cough with mucoid expectoration for four months. Coughing was associated with chest pain in the right inframammary region. The cough was also associated with mild hemoptysis and was not relieved by a cough suppressant. The patient also complained of breathlessness for four months, progressing from grade 1 to grade 3 mMRC, which was aggravated by exertion and relieved by rest. The patient complained of intermittent low-grade fever for four months. He gave a history of exposure to biomass of plant origin. The patient also complained of weight loss with no change in appetite. The patient had a history of paroxysmal nocturnal dyspnea, which was relieved by sitting in a flexed posture. The patient was sleep-deprived due to cough and breathlessness. On examination, blood pressure was 108/72 mmHg, pulse rate was 69 beats/minute, respiratory rate was 18 breaths/minute, and oxygen saturation was 96% in room air. Upon physical examination, respiratory sounds in the right lower lobe were decreased. A chest X-ray in an erect position in the posteroanterior view revealed homogenous rounded consolidation in the right lower zone of the lung (Figure 1).
Chest radiograph of the patient on presentation.Homogenous rounded consolidation in the right lower zone of the lung.
Subsequent sputum examination showed positive results for auramine-rhodamine fluorescent stain for Mycobacterium tuberculosis (Figure 2). Rifampicin resistance was not detected. Blood investigations showed hemoglobin of 9.3 g/dL (reference range = 12-16 g/dL). Serum IgE levels were 1,127 ng/mL. Serum IgG specific for Aspergillus fumigatus was positive. The remaining pertinent laboratory results are shown in Table 1 and Table 2.
Mycobacterium bacilli stained with fluorescent auramine-rhodamine stain.
After an X-ray and laboratory examination, a further radiological examination with high-resolution computed tomography (HRCT) was done (Figure 3). HRCT of the lungs revealed a cavitary lesion measuring approximately 4 × 6 × 5.1 cm in the posterobasal segment of the right lower lobe with adjacent areas of ground-glass opacities and soft tissue opacification within the cavity, evidence of crescent-shaped lucency around the soft tissue strongly supporting mycetoma. Multiple areas of centrilobular nodules arranged in linear branching patterns showed bud appearance in the right lower lobe due to active infective etiology.
Computed Tomography Scan of the Chest of the Patient at Presentation(A) evidence of crescent-shaped lucency around the soft tissue and (B) Posterobasal segment of the right lower lobe with adjacent areas of ground glass opacities and soft tissue opacification within the cavity.
Initially, the patient was started on broad-spectrum antibiotics (ceftriaxone), antipyretics, and cough suppressants. Cough suppressants showed minimal effectiveness. For mild hemoptysis, the patient was prescribed etamsylate, tranexamic acid, and vitamin K, which immediately decreased the episodes of hemoptysis. After confirming the diagnosis of tuberculosis, the patient started ATT, which included a combination of isoniazid, rifampicin, pyrazinamide, and ethambutol. After the patient was confirmed to have mycetoma (aspergilloma), he was started on oral Itraconazole. The patient showed good symptomatic improvement and was discharged and asked to follow up after one month.
Discussion
Pulmonary tuberculosis can cause remodeling of the lung parenchyma through various processes, including pulmonary cavitation, pulmonary fibrosis, bronchiectasis, airflow obstruction, restrictive ventilatory defects, and impaired gas exchange. Patients with pulmonary tuberculosis, especially those with secondary tuberculosis, develop cavitary lesions susceptible to *Aspergillus *infection [4,5]. Depending on the changes in the lung, parenchyma aspergillosis can manifest as saprophytic aspergilloma (mycetoma), allergic bronchopulmonary aspergillosis, and invasive aspergillosis [6]. This type of change leads to dead space in the lung parenchyma, devoid of the blood supply, providing a suitable environment for fungal infections such as aspergillosis in the form of mycetoma can also be called aspergilloma or fungal ball [7]. Chest CT shows a cavitary lesion in the posterobasal segment of the right lower lobe with adjacent areas of ground-glass opacities and soft tissue opacification within the cavity [8]. Multiple areas of centrilobular nodules arranged in linear branching patterns show a tree-in-bud appearance in the right lower lobe due to active *Aspergillus *infection [9]. The patient started taking broad-spectrum antibiotics, antipyretics, and cough suppressants for symptomatic relief. After confirmation of pulmonary tuberculosis, the patient started taking ATT while continuing the earlier prescription for symptomatic relief. After confirmation of mycetoma, the patient was started on oral itraconazole. Treatment proved to be effective and symptomatic relief was seen in the patient. Taking into account the symptomatic improvement, the patient was discharged and asked to follow up after one month.
Conclusions
Notably, the simultaneous isolation of *Aspergillus *species and Mycobacterium tuberculosis from respiratory samples is challenging and needs careful consideration to prevent adverse outcomes. Along with the treatment for symptomatic relief of tuberculosis, the patient was started with an ATT regimen. As for mycetoma, pharmacotherapy with itraconazole has a minimal role because the lungs are already damaged. Moreover, mycetoma cannot be removed as the infected part does not have enough blood supply for the effective action of pharmacotherapy provided by drugs. Taking into account these factors, mycetoma must be removed surgically by right lower lobectomy for complete eradication of the infected part. Clinical regression and symptom improvement were observed in the patient. Accurate diagnosis and treatment with a multidisciplinary team within limited time and resources can be the difference between morbidity and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Concomitant presence of Aspergillus species and Mycobacterium species in the respiratory tract of patients: underestimated co-occurrence?Front Microbiol Dellière S Angebault C Fihman V 29801020193199826710.3389/fmicb.2019.02980 PMC 6967598 · doi ↗ · pubmed ↗
- 2Aspergillus in the lung: diverse and coincident forms Eur Radiol Buckingham SJ Hansell DM 178618001320031278317410.1007/s 00330-002-1813-4 · doi ↗ · pubmed ↗
- 3Chronic pulmonary aspergillosis as a cause of smear-negative TB and/or TB treatment failure in Nigerians Int J Tuberc Lung Dis Oladele RO Irurhe NK Foden P 105610612120172882645610.5588/ijtld.17.0060 · doi ↗ · pubmed ↗
- 4Pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: incidence, risk factors, and outcome Clin Microbiol Infect Guinea J Torres-Narbona M Gijón P 8708771620101990627510.1111/j.1469-0691.2009.03015.x · doi ↗ · pubmed ↗
- 5Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: case series, proposed nomenclature change, and review Clin Infect Dis Denning DW Riniotis K Dobrashian R Sambatakou H 08037 Suppl 3200310.1086/37652612975754 · doi ↗ · pubmed ↗
- 6Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings Radiographics Franquet T Müller NL Giménez A Guembe P de La Torre J BaguéS 8258372120011145205610.1148/radiographics.21.4.g 01jl 03825 · doi ↗ · pubmed ↗
- 7Tuberculosis and lung damage: from epidemiology to pathophysiology Eur Respir Rev Ravimohan S Kornfeld H Weissman D Bisson GP 1700772720182949103410.1183/16000617.0077-2017 PMC 6019552 · doi ↗ · pubmed ↗
- 8Imaging findings in acute invasive pulmonary aspergillosis: clinical significance of the halo sign Clin Infect Dis Greene RE Schlamm HT Oestmann JW 3733794420071720544310.1086/509917 · doi ↗ · pubmed ↗