Unraveling the Complexity: Ehrlichiosis-Induced Septic Shock and Acute Respiratory Distress Syndrome
Anshu Kataria, Anne M Arcidiacono, Minhaz Murshad, Shuvendu Sen, Ahmad A Homoud

TL;DR
A 67-year-old man developed severe ehrlichiosis leading to septic shock and ARDS, but recovered after doxycycline treatment.
Contribution
This case highlights the rare severity of ehrlichiosis and effective management strategies using doxycycline.
Findings
Prompt treatment with doxycycline led to full recovery from severe ehrlichiosis.
Ehrlichia chaffeensis infection was identified as the cause of septic shock and ARDS in an immunocompetent patient.
Abstract
Human monocytic ehrlichiosis typically presents with nonspecific cold-like symptoms and a history of recent tick exposure, often responding well to early treatment. Here, we present the case of a 67-year-old immunocompetent male who initially presented with fevers, chills, dysuria, and hematuria, leading to admission to the intensive care unit with septic shock and acute respiratory distress syndrome (ARDS), which was later attributed to Ehrlichia chaffeensis infection. Prompt treatment with doxycycline resulted in a full clinical recovery. This case highlights the rare occurrence of severe ehrlichiosis and provides insights into its effective management based on updated literature.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
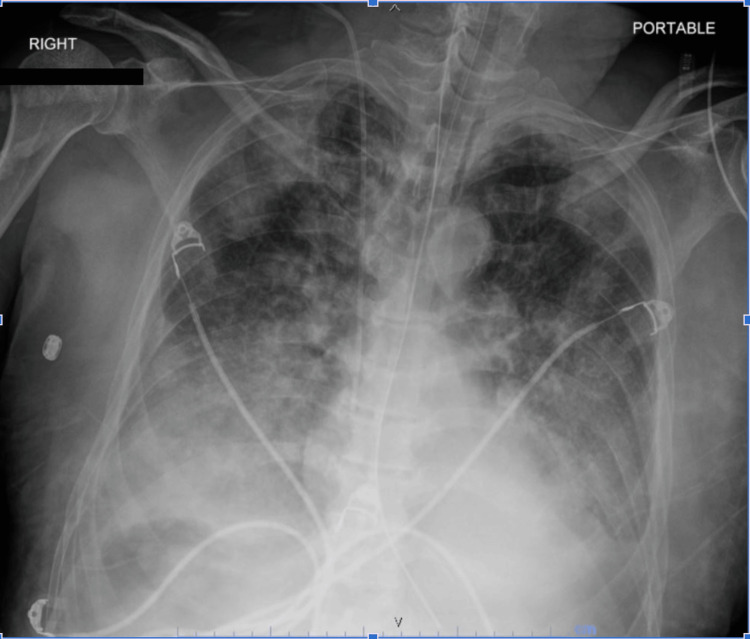 Figure 1
Figure 1| Lab values | Initial labs | At the time of the development of septic shock | Reference values |
| Prothrombin time | - | 14.7 (H) | 11-13.5 seconds |
| International normalized ratio | - | 1.26 (H) | 0.9-1.1 |
| Partial thromboplastin time | - | 46 (H) | 25-35 seconds |
| Fibrinogen | - | 505 | 200-400 |
| WBCs | 4.6 | 10.8 | 4.5-11.0 x 103/uL |
| Hemoglobin | 13.3 | 11.1 (L) | 13.5-17.5 g/dL |
| Hematocrit | 39.6 | 33.0 (L) | 41.0-53.0% |
| Platelet count | 37 | 25 (L) | 150-450 x 103/uL |
| Lymphocytes, % | 4.4 (L) | 2.6 (L) | 20-40% |
| Monocytes, % | 5.3 | 1.8 | 2-10% |
| Eosinophils, % | 0.0 | 0.0 | 1-6% |
| Neutrophils, absolute | 4.0 | 9.0 (H) | 2-7 x 103/uL |
| Lymphocytes, absolute | 0.3 (L) | 0.4 (L) | 1-4 x 103/uL |
| Monocytes, absolute | 0.2 | 0.2 | 0.2-0.8 x 103/uL |
| Eosinophils, absolute | 0.0 | 0.0 | 0.04-0.4 x 103/uL |
| Segmented neutrophils, % | 76.3 (H) | 26.3 (L) | 40-75% |
| Bands, % | 10.5 | 57.0 (H) | 0-5% |
| Metamyelocytes | 0.9 (H) | 11.4 (H) | 0.0% |
| Metamyelocytes, absolute | 0.0 | 1.2 (H) | 0.0 x 103/uL |
| Anisocytosis | 1+ (Slight) | 1+ (Slight) | Normal |
| Macrocytes | 1+ (Slight) | 1+ (Slight) | Normal |
| RBC morphology | Abnormal | Abnormal | Normal |
| Glucose | 149 (H) | 65 (L) | 70-100 mg/dL |
| Blood urea nitrogen | 12 | 12 | 7-20 mg/dL |
| Creatinine | 1.14 | 1.07 | 0.6-1.2 mg/dL |
| Estimated glomerular filtration rate | ≥60 | ≥60 | >60 mL/min/1.73 m2 |
| Sodium | 133 (L) | 140 | 135-145 mmol/L |
| Chloride | 101 | 108 (H) | 98-107 mmol/L |
| Anion gap | 7 | 9 | 5-15 mmol/L |
| Calcium | 8.8 | 7.7 (L) | 8.7-10.4 mmol/L |
| Bicarbonate | 25 | 23 | 20-31 mmol/L |
| Alkaline phosphatase | 179 (H) | 133 (H) | 46-116 U/L |
| Protein total | 6.8 | 4.9 (L) | 6.0-8.3 g/dL |
| Albumin | 3.3 (L) | 2.0 (L) | 3.4-5.0 g/dL |
| Bilirubin total | 1.0 | 1.3 | 0.2-1.3 mg/dL |
| Aspartate aminotransferase | 153 (H) | 345 (H) | 0-34 U/L |
| Alanine transaminase | 174 (H) | 258 (H) | 10-49 U/L |
| Brain natriuretic peptide | - | 155 (H) | <100 pg/mL |
| Lactic acid | 1.7 | 2.7 (H) | 0.5-2.2 mmol/L |
| Procalcitonin | 1.02 (H) | 7.32 (H) | <0.50 ng/mL |
| Lactate dehydrogenase | - | 516 (H) | 120-246 U/L |
| Ferritin | - | 1502.2 (H) | 10.5-307.3 ng/mL |
| Haptoglobin | - | 106 | 40-280 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Insect and Pesticide Research · Dermatological diseases and infestations
Introduction
Ehrlichiosis is a disease transmitted by tick-borne vectors, specifically the lone star and blacklegged ticks found primarily in the northeast and southeast regions of the USA [1, 2]. Cases of ehrlichiosis have been steadily rising since the year 2000 in the USA, with concern that it may be linked to warmer climate change [3]. Onset typically occurs five to 14 days after the initial tick bite, with early illness presenting with mild nonspecific symptoms, i.e., fevers/chills, headache, malaise, myalgias, and rash (mostly in children). According to the Centers for Disease Control and Prevention (CDC), late illness is typified by severe manifestations of CNS involvement (20%), acute respiratory distress syndrome (ARDS), septic shock, toxic shock-like syndromes, renal/hepatic failure, and coagulopathies. The CDC also states that risk factors for these severe manifestations include delayed treatment, age extremes, and immunocompromising conditions [4]. The treatment for ehrlichiosis is typically doxycycline for seven to 10 days with favorable outcomes and a rare progression into late/severe illness.
Case presentation
Investigation
We report the case of a 67-year-old male patient with a medical history of hyperlipidemia, nonobstructive coronary artery disease, and benign prostatic hyperplasia who presented with a high-grade fever, hematuria, dysuria, lethargy, and increased urinary frequency, initially suspected to be prostatitis-related sepsis. The patient had recently traveled to Niagara Falls and Toronto and had been prescribed nitrofurantoin without symptom improvement. Notably, the only other medication the patient was prescribed was tamsulosin for benign prostatic hyperplasia, which he had not started taking.
Upon arrival at the ED, the patient's temperature was 100.6°F, and he displayed tachycardia at 104 beats per minute with a blood pressure of 119/78 mmHg. During his ED stay, his temperature spiked to 104.3°F, and he became hypotensive at 86/48 mmHg. Physical examination revealed rigors, sinus tachycardia, and diaphoresis.
Diagnosis
Initial laboratory findings included thrombocytopenia (platelet count of 37), an elevated segmented neutrophil percentage (76.3%), and transaminitis, with elevated levels of aspartate aminotransferase (153 U/L), alanine transaminase (174 U/L), and alkaline phosphatase (179 U/L), as shown in Table 1. Urinalysis showed numerous RBCs and proteins without WBCs. CT abdomen and pelvis showed an enlarged prostate. Given the transaminitis, a right upper quadrant ultrasound and hepatobiliary iminodiacetic acid scan were performed, both of which ruled out cholecystitis.
With the patient's clinical presentation and laboratory findings, sepsis treatment was initiated, focusing on the prostate as the source (suspected prostatitis). IV vancomycin and IV piperacillin/tazobactam were administered, and the patient was transferred to the intensive care unit (ICU) due to concern for septic shock. During the ICU stay, the patient's condition deteriorated, with increasing pressor requirements, rising lactic acidosis, intermittent temperature spikes, and the development of ARDS requiring intubation. Infectious disease specialists recommended broadening antibiotic coverage for better prostate penetration, resulting in the addition of IV levofloxacin. On the fourth day of admission, a positive Ehrlichia chaffeensis PCR confirmed the diagnosis (Figure 1).
Chest X-ray demonstrating ARDS in our patient.ARDS: acute respiratory distress syndrome.
Treatment
The patient received prompt IV doxycycline (100 mg twice daily for one week) and prior antibiotics were discontinued, leading to decreased pressor requirements and an improved overall condition.
Follow-up and outcomes
Eleven days after recovering from ARDS, the patient was successfully extubated. During his hospitalization, he experienced speech and swallowing difficulties necessitating G-tube placement. Otherwise, his hospital course was unremarkable, and he was discharged to subacute rehabilitation with a full recovery.
Discussion
Human monocytic ehrlichiosis (HME), as seen in our patient, is caused by E. chaffeensis, a Gram-negative intracellular bacterium transmitted by blacklegged and lone star ticks [5]. This bacterium has been increasingly detected in the northeastern and southeastern USA. Ehrlichia chaffeensis invades phagocytes through endocytosis, suppressing apoptosis and inhibiting innate immune responses, primarily affecting peripheral blood cells [5]. Though not tried in our case, interferon (IFN)-gamma is key to clearing E. chaffeensis infection, and iron chelation therapy with deferoxamine can inhibit its propagation [6].
Ehrlichiosis symptoms vary widely, with most clinical manifestations resulting from the host's inflammatory response rather than the bacterium itself. It is often likened to a "toxic shock-like syndrome" due to the robust immune response despite low bacterial loads. Common initial symptoms include fever, chills, severe headache, myalgias, nausea, vomiting, diarrhea, loss of appetite, and confusion, with laboratory findings such as leukopenia, thrombocytopenia, and transaminitis. Approximately one-third of patients may develop a rash, typically appearing around five days after fever onset [7].
Early detection and treatment are critical for preventing the progression to severe disease. Given the nonspecific symptoms and frequent lack of tick bite recollection [8], diagnosis often relies on PCR, as Ehrlichia morulae are rarely seen in peripheral smears. Doxycycline is the primary treatment, with few reports of success with rifampin and only in in vitro studies [9,10]. Patients typically respond to doxycycline within 48-72 hours.
Prevention is essential, focusing on avoiding tick bites. Post-tick bite prophylaxis and testing patient-retrieved ticks for infection are not recommended [11]. The CDC outlines guidelines for tick-borne disease prevention, including avoiding tick-infested areas, wearing protective clothing, applying permethrin spray, using Environmental Protection Agency-registered insect repellents, and conducting thorough skin checks after outdoor activities [12].
Conclusions
The number of ehrlichiosis cases has been steadily rising, necessitating consideration of this diagnosis in endemic areas. While the case fatality rate remains low, the risk of progression to severe disease underscores the importance of early recognition and treatment. Our case emphasizes the need for a broad differential diagnosis when dealing with a fever of unknown origin or when conventional sepsis treatment is ineffective. Further research is warranted to develop more rapid testing and detection methods.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Approximate distribution of the lone star tick 10 2023 2011 https://www.cdc.gov/ticks/maps/lone_star_tick.html
- 2General distribution of blacklegged ticks (Ixodes scapularis) 10 2023 2018 https://www.cdc.gov/ticks/maps/blacklegged_tick.pdf
- 3Increased risk of tick-borne diseases with climate and environmental changes Can Commun Dis Rep Bouchard C Dibernardo A Koffi J Wood H Leighton PA Lindsay LR 8389452019 https://pubmed.ncbi.nlm.nih.gov/31285697/3128569710.14745/ccdr.v 45i 04a 02PMC 6587693 · doi ↗ · pubmed ↗
- 4Centers for Disease Control and Prevention. Ehrlichiosis 10 2023 2022 http://www.cdc.gov/Ehrlichiosis/
- 5Molecular and cellular pathobiology of Ehrlichia infection: targets for new therapeutics and immunomodulation strategies Expert Rev Mol Med 10 2023 Mc Bride JW Walker DH 013201110.1017/S 1462399410001730 PMC 376746721276277 · doi ↗ · pubmed ↗
- 6Abrogation of gamma interferon-induced inhibition of Ehrlichia chaffeensis infection in human monocytes with iron-transferrin Infect Immun 10 2023 Barnewall RE Rikihisa Y 48044810621994 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 303190/pdf/iai 00011-0120.pdf 792775810.1128/iai.62.11.4804-4810.1994 PMC 303190 · doi ↗ · pubmed ↗
- 7Ehrlichiosis: signs and symptoms 10 2023 2019 https://www.cdc.gov/ehrlichiosis/symptoms/index.html
- 8RMSF: deadly, but preventable 10 2023 2019 https://www.cdc.gov/ncezid/dvbd/media/rmsf.html