A Rare Case of Renal Vein Thrombosis Secondary to Oral Contraceptive Pills
Lavneet Chawla, Amitoj S Sachdeva

TL;DR
A 29-year-old woman developed kidney vein blood clots likely due to birth control pills, highlighting the need to consider this risk factor.
Contribution
This case report highlights the rare but important link between oral contraceptive use and renal vein thrombosis.
Findings
A 29-year-old female with oral contraceptive use developed unilateral renal vein thrombosis.
Discontinuation of oral contraceptives and anticoagulation therapy led to symptom improvement.
The case emphasizes oral contraceptives as a risk factor for venous thromboembolism.
Abstract
Renal vein thrombosis (RVT) is a common complication of nephrotic syndrome and renal malignancy. However, its association with oral contraceptive use has rarely been reported. We report a case of a 29-year-old female with a history of oral contraceptive use, presenting with acute flank pain. On further investigation, she was found to have unilateral RVT. Oral contraception was discontinued, and she was started on therapeutic anticoagulation, initially with low-molecular-weight heparin, and then switched to apixaban. Her symptoms improved, and she is currently doing well. This case signifies the importance of proper history-taking and how oral contraception should be considered a significant risk factor for venous thromboembolism.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
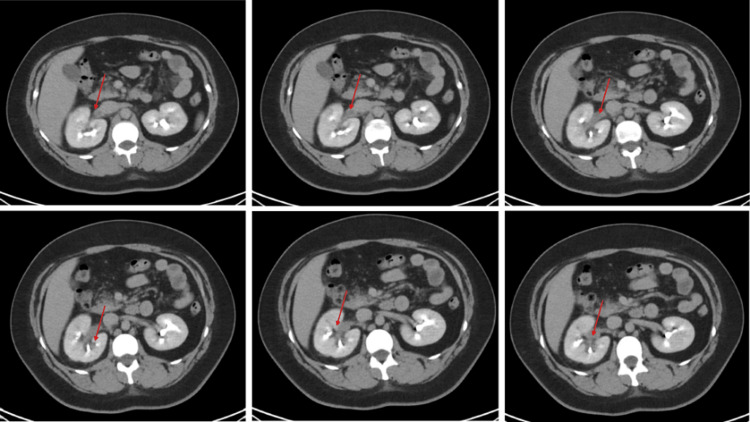 Figure 1
Figure 1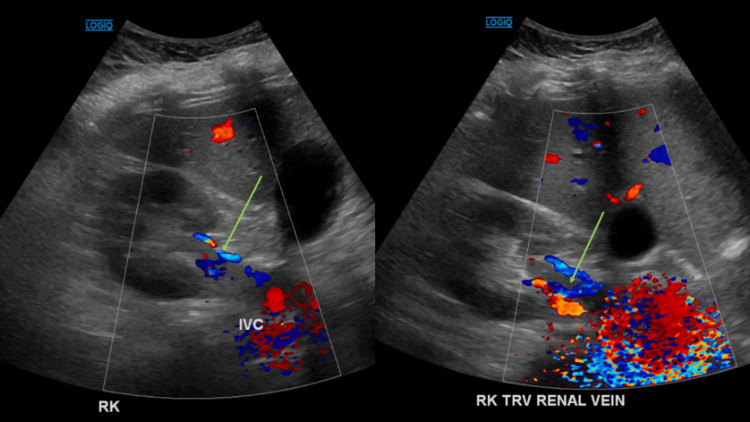 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Renal and Vascular Pathologies · Pharmaceutical industry and healthcare
Introduction
Renal vein thrombosis (RVT) is a relatively rare condition characterized by thrombus formation in the renal veins or their branches. It is commonly seen in patients with nephrotic syndrome, renal malignancy, or in infants with inherited thrombophilia [1]. Previous studies have reported an increased incidence of venous thromboembolism with oral contraceptive pills (OCPs), but solitary RVT has rarely been reported. Here, we present a case of unilateral RVT in a patient taking OCPs for polycystic ovarian syndrome (PCOS) and an unremarkable inherited thrombophilia workup.
Case presentation
A 29-year-old Caucasian female with a previous medical history of iron deficiency anemia (IDA) and long-term estrogen-based OCP use for PCOS presented with sharp right flank pain for two days, radiating down to her right groin. She had associated non-bloody, non-bilious vomiting and suprapubic discomfort. She denied fevers, chills, dysuria, gross hematuria, heavy weightlifting, or trauma to her back. She denied any history of smoking. Her vitals and physical examination were unremarkable. The patient's BMI was 42 kg/m^2^. The complete blood count showed a white blood cell count of 15,350/mcL and a hemoglobin level of 7.8 g/dL. The complete metabolic panel was unremarkable. The urinalysis showed 3+ protein, 11-20 WBC/hpf (high power field), and a moderate amount of bacteria. The D-dimer level was 2.87 mcg/mL (normal <0.50 mcg/mL), and SARS-CoV-2 was negative. A computed tomography (CT) scan of the abdomen and pelvis with contrast showed no renal or ureteral stones. However, it showed mild right perinephric stranding and a filling defect in the right renal vein, concerning a thrombus (Figure 1). The renal Doppler ultrasound showed an area of hyperechogenicity within the right renal vein with elevated venous flow, consistent with thrombosis (Figure 2). OCP was discontinued, and she was started on therapeutic (1 mg/kg every 12 hours) low-molecular-weight heparin (LMWH) for RVT and ceftriaxone for concurrent pyelonephritis. The patient underwent a thrombophilia workup that was unremarkable, including antithrombin III, homocysteine levels, factor V Leiden, factor II prothrombin gene, lupus anticoagulant, and proteins C and S. The patient’s renal function remained stable, and her symptoms improved. She was transitioned to apixaban and referred to gynecology for PCOS management with the recommendation of avoiding estrogen-based therapy and completing a 24-hour urine protein study.
CT of the abdomen and pelvis with an IV contrast series demonstrating mild right perinephric fat stranding and filling defect in the right renal vein (red arrow).
Hyperechogenicity within the right renal vein with elevated venous flow (green arrow) on renal Doppler ultrasound.RK: right kidney; IVC: inferior vena cava; TRV: traverse
Discussion
Apart from OCPs, other risk factors for RVT include infection, trauma, extrarenal compression of the renal vein, and, most recently, SARS-CoV-2 [2]. OCPs affect blood clotting by increasing plasma fibrinogen levels and increasing the activity of factors VII and X. The antithrombin activity is decreased. RVT primarily affects the left side and is more common in women than men. The symptoms of acute RVT may include flank pain, back pain, or hematuria, and if bilateral, patients can have renal dysfunction. Diagnosing RVT requires clinical suspicion and can be confirmed with CT angiography or magnetic resonance (MR) venography. Ultrasonography with Doppler has low sensitivity [3].
In our case, the patient presented with acute flank pain and had a right RVT with no evidence of nephrotic syndrome or malignancy on abdominal imaging, and her thrombophilia workup was unremarkable. OCP use appeared to be her unique underlying risk factor, although underlying pyelonephritis as a risk factor could not be completely ruled out. There have been a few cases of RVT reported previously with OCP use [4-11]. Miyahara et al. reported a case of left RVT in a patient using OCPs. Their patient also had smoking as an additional contributing risk factor, which was not seen in our patient [4]. Sasaki et al. reported a case of left RVT in a Japanese female patient, who also had smoking as an additional contributing risk factor [5].
Local thrombolytic therapy with or without catheter-directed thrombolysis is recommended for patients with renal dysfunction to restore renal venous flow and renal function. In contrast, therapeutic anticoagulation is recommended for patients with chronic RVT or acute RVT without renal dysfunction. The efficacy of warfarin as a direct oral anticoagulant (DOAC) has not been well studied. However, patients should receive unfractionated heparin or LMWH prior to transitioning to warfarin. A few studies have reported the role of DOACs in RVT. Zhang et al. performed a small study on 16 patients and observed similar efficacy with rivaroxaban compared to LMWH [12]. Matta et al. successfully treated a 44-year-old patient with rivaroxaban who presented with isolated right RVT and bilateral pulmonary embolism [13]. In our case, OCP discontinuation and underlying menorrhagia added further complexity as anticoagulation increased the patient's bleeding risk. After a multidisciplinary discussion with the hematologist and the patient, apixaban was used with plans of repeating imaging in three months to monitor thrombus status.
Conclusions
We highlight the importance of having RVT on the differential diagnosis when a patient presents with acute flank pain, especially with a history of OCP use. This case also demonstrates a therapeutic dilemma due to the limited evidence to support the use of DOACs in RVT, and more studies are needed to establish their use in the treatment of RVT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A patient with spontaneous bilateral renal vein thrombosis but no risk factors Int J Surg Case Rep Pradhan J Han S Girishkumar H 10796310420233688915610.1016/j.ijscr.2023.107963 PMC 10015233 · doi ↗ · pubmed ↗
- 2Renal vein thrombosis treated with apixaban in a patient with COVID-19: a case report Cureus Kakhktsyan T Mousa A Arshad H Chepenko K Fatima T 015202310.7759/cureus.39296 PMC 1028147737346224 · doi ↗ · pubmed ↗
- 3Intrarenal arterial Doppler sonography in the detection of renal vein thrombosis of the native kidney AJR Am J Roentgenol Platt JF Ellis JH Rubin JM 136713701621994819200110.2214/ajr.162.6.8192001 · doi ↗ · pubmed ↗
- 4Renal vein thrombosis occurring in association with oral contraceptives: a case report Ann Vasc Dis Miyahara T Nishino Y Ozaki M Ogiwara M 1311341620233735910010.3400/avd.cr.22-00129 PMC 10288121 · doi ↗ · pubmed ↗
- 5Renal vein thrombosis associated with oral contraception and smoking: a case report from Japan, with literature review CEN Case Rep Sasaki Y Shimabukuro A Isegawa T Tamori Y Koshiishi T Yonaha H 100105320142850925210.1007/s 13730-013-0095-9PMC 5413680 · doi ↗ · pubmed ↗
- 6Acute renal vein thrombosis, oral contraceptive use, and hyperhomocysteinemia Mayo Clin Proc Chan HH Douketis JD Nowaczyk MJ 2122147620011121331210.4065/76.2.212 · doi ↗ · pubmed ↗
- 7Mild unilateral proteinuria and renal vein thrombosis associated with oral contraceptive usage Am J Kidney Dis Goldman RS Kettwich DL Woodside JR 47147321983682396310.1016/s 0272-6386(83)80080-8 · doi ↗ · pubmed ↗
- 8Hypertension, renal vein thrombosis and renal failure (occurring in a patient on an oral contraceptive agent)Clin Nephrol Slick GL Schnetzler DE Kaloyanides GJ 707431975 https://pubmed.ncbi.nlm.nih.gov/1122661/1122661 · pubmed ↗