Complex Cardiovascular Morbidities in Prader-Willi Syndrome: A Multidisciplinary Approach
Raul Alba, Soroush Omidvarnia, Jared J Bies, Tim Carlson, Qusay Alfaori, Thwe Htay

TL;DR
This paper highlights the complex cardiovascular issues in Prader-Willi Syndrome and the importance of a multidisciplinary treatment approach.
Contribution
The paper presents a case study emphasizing the need for interdisciplinary care in managing cardiovascular complications in PWS.
Findings
PWS patients can have multiple coexisting cardiovascular and metabolic conditions.
A collaborative approach involving various specialists is essential for effective management.
Current treatments focus on symptom management, but genetic research may offer future improvements.
Abstract
This case emphasizes the complexity of Prader-Willi syndrome (PWS), the need for a collaborative approach from specialists, and a closer look at the various cardiovascular complexities associated with this syndrome. While current treatments focus on managing symptoms, ongoing genetic research offers hope for more favorable outcomes. Further studies are crucial to gauge the effectiveness of these treatments for PWS patients. We detail a patient with a complex medical history of PWS, further complicated by congenital heart disease with Eisenmenger’s syndrome, diabetes mellitus, pulmonary hypertension, venous insufficiency, hypothyroidism, and hyperlipidemia. Reported in this study is a compilation of clinical data as well as suggestions from several medical specialists in applying a multifaceted approach to treatment, significantly emphasizing the need for interdisciplinary care and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
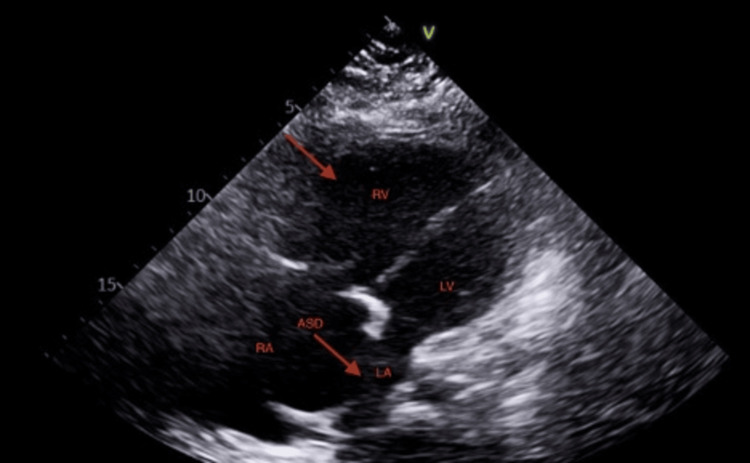 Figure 1
Figure 1| Lab | Patient value | Reference ranges |
| White blood cell count (WBC) | 9.87 x 103/UL | 4.50-11.03 x 103/UL |
| Reb blood cell count (RBC) | 5.91 x x 106/UL High | 3.50-5.50 x 106/UL |
| Hemoglobin | 17.1 g/dL High | 12.0-15.0 g/dL |
| Hematocrit | 58.2% High | 40-50% (male), 36-46% (female) |
| Platelets | 174 x 103/µL | 150-450 x 103/µL |
| Sodium, serum | 136 mmol/L | 135-145 mmol/L |
| Potassium, serum | 4.8 mmol/L | 3.5-5.0 mmol/L |
| Chloride, serum | 104 mmol/L | 98-108 mmol/L |
| Blood urea nitrogen, serum | 27 mg/dL High | 7-20 mg/dL |
| Creatinine | 0.9 mg/dL | 0.6-1.3 mg/dL |
| Calcium, serum | 8.1 mg/dL Low | 8.5-10.5 mg/dL |
| Magnesium, serum | 1.6 mg/dL | 1.7-2.2 mg/dL |
| Albumin, serum | 3 g/dL Low | 3.5-5.0 g/dL |
| N-terminal pro-BNP (NT-proBN) | 5,290 pg/mL | <300 pg/mL |
| Cholesterol, serum | 187 mg/dL | <200 mg/dL |
| Triglycerides, serum | 150 mg/dL | <150 mg/dL |
| HDL Cholesterol, serum | 25 mg/dL Low | 40 (men), >50 (women) mg/dL |
| LDL Calculated | 132 mg/dL High | <100 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic Syndromes and Imprinting · Apelin-related biomedical research · Congenital heart defects research
Introduction
We present a case report of a 20-year-old female with Prader-Willi Syndrome (PWS), a rare and complex genetic disorder that is the leading genetic cause of life-threatening obesity in humans [1]. PWS results from the loss of expression of paternally derived genes in the PWS critical region on chromosome 15q11-q13, which can occur due to a paternal deletion, maternal uniparental disomy 15, or an imprinting defect [2,3].
Although cardiovascular abnormalities are known to be associated with PWS, such as congenital heart defects and myocardial dysfunction [4], our patient had an unusual combination of multiple medical conditions, including Eisenmenger’s syndrome, congestive heart failure, diabetes mellitus, pulmonary hypertension, venous insufficiency, hypothyroidism, and hyperlipidemia. This case illustrates the necessity for a multidisciplinary approach in managing PWS patients with complex and co-existing medical problems and delves into the various cardiovascular complications associated with PWS.
Case presentation
A 20-year-old female with a past medical history of PWS, secundum ASD and multiple fenestrations with predominantly right to left shunt (Eisenmenger’s syndrome), congestive heart failure, diabetes mellitus, severe pulmonary hypertension, venous insufficiency, hypothyroidism, and hyperlipidemia presented to the emergency department for worsening anasarca and respiratory distress. The patient had multiple similar presentations as a result of her worsening clinical status.
The patient’s previous medication regimen included macitentan, riociguat, and sildenafil and discontinued them due to intolerable side effects. The patient’s medications upon presentation consisted of furosemide 40 mg daily, Insulin glargine 20 units twice daily, and levothyroxine 100 mcg daily. The patient used 3L nasal cannula oxygen at a baseline. Her family history was significant for diabetes mellitus in her father, and she denied the use of tobacco, alcohol, or illicit drugs.
On physical examination, the patient presented with a temperature of 36.7 °C, a heart rate of 83 (peripheral), and an oxygen saturation of 90% with 3L of nasal canular O2. The patient was vitally stable, alert, oriented, and well-nourished. Lung bases were decreased on auscultation bilaterally, non-labored respiration was present, and 3+ pitting edema in her lower extremities. An 8-cm-wide venous stasis ulcer on the left lower limb was present. Initial laboratory findings showed a WBC count of 9.87 × 10^3^/UL, hemoglobin of 17.1 g/dL, and hematocrit of 58.2% (Table 1).
Hospital course
Respiratory Support
High-flow nasal canula was utilized to sustain adequate oxygen levels upon admission. Our patient underwent a trial of pulmonary vasodilators including sildenafil and macitentan but was unable to tolerate these treatments. Oxygenation via high-flow nasal canula was continued and gradually weaned to a nasal canula as tolerated.
Cardiovascular Management
Cardiovascular management involved conducting comprehensive imaging studies. A transthoracic cardiac echocardiogram showed the right atrium and right ventricle (RV) severely dilated with depressed RV systolic function. Small LV size with flattened interventricular septum consistent with RV pressure/volume overload (Figure 1). Right heart catheterization further confirmed the presence of severe right heart failure.
Transthoracic echocardiogramRight ventricle and atrial septal defect marked by red arrows.
Renal and Metabolic Stabilization
Our patient underwent renal ultrafiltration to address pulmonary hypertension but was unable to complete the full treatment due to intolerance. Nephrotoxic medications were strictly avoided to preserve renal function, and strategies for maintaining hydration were implemented. The patient continued diuresis with IV furosemide, with closed monitoring of oxygenation, strict intake/output, electrolyte balance, daily weights, and kidney function. Hypoglycemia was managed by discontinuing her home insulin regimen and initiating insulin sliding scale for optimizing blood glucose levels.
Wound care management
The wound identified on left anterior tibia, diagnosed as a venous stasis ulcer, required specialized wound care and a multidisciplinary team approach. Patient received meticulous dressing changes, regular wound assessments, and specific wound care to expedite healing and infection prevention.
Throughout her hospitalization, our patient underwent an intricate treatment regimen comprising respiratory support, attempted vasodilator therapy, vigilant cardiovascular management, renal function preservation, glucose regulation, and specialized wound care. Our patient’s cardiovascular and respiratory status returned to baseline with 2-3L nasal cannula oxygen, and her acute kidney injury (AKI) resolved, returning to within normal limits. The patient’s wound was last assessed with no signs or symptoms of infection noted. The patient was discharged home with oral daily furosemide and continuous oxygenation, along with scheduled outpatient follow-up and wound care.
Discussion
This case highlights the multifaceted considerations necessary for managing a patient with PWS and multiple co-occurring conditions that result from severe pulmonary hypertension and right heart failure. Particularly, a need for multi-specialty collaboration and careful monitoring to improve the patient’s overall health and well-being. The care of our patient is orchestrated by a multidisciplinary team including specialists in cardiology, pulmonology, nephrologists, internal medicine, endocrinology, nutrition, respiratory care, therapy (occupational, speech, physical), and wound care. Together, they collaboratively delivering comprehensive treatment.
PWS is a condition involving a complicated mixture of genetic factors and cardiovascular comorbidities. Numerous cases consistently showed how young adults with PWS often suffer from cardiovascular risk factors such as high cholesterol, diabetes, and high blood pressure, demonstrating cardiovascular vulnerability within the young adult demographic [5]. In particular, higher levels of C-reactive protein, which are linked to underlying inflammation, exacerbate the intricate cardiovascular risks in patients with PWS [6].
One case report detailed a 27-year-old man with PWS and multiple underlying comorbidities such as obesity, hypertension, diabetes mellitus, and dyslipidemia, which led to three-vessel coronary artery disease (CAD) [7]. These findings emphasize how patients with PWS are at greater risk of early-onset heart disease, stressing the urgent need for more specific strategies to manage cardiovascular risks.
Another study showcased a 10-year-old boy with PWS who was experiencing sinus pauses, calling attention to the importance of careful heart rate monitoring in younger individuals who suffer from PWS [8]. This patient’s subsequent need for a pacemaker status-post syncope indicates potential arrhythmia risks, further supporting the notion of ongoing heart rhythm studies for children with PWS, aiding in the prevention of serious complications in the future. Additionally, the literature explains the broader effects of obesity, both idiopathic and syndromic, on cardiovascular health [9, 10]. While idiopathic obesity and cardiovascular consequences are extensively studied, these studies accentuate the shortage of data on syndromic obesity in conditions like PWS, characterized by heterogeneous phenotypes and premature mortality, placing emphasis on the crucial need for more research to understand more specific cardiovascular risks linked to syndromic obesity in individuals with PWS [11,12].
PWS is a rare genetic disorder that affects multiple body systems and causes various clinical features throughout the patient’s life span [13]. The diagnosis of PWS is based on clinical criteria and confirmed by genetic testing [2]. The management of PWS involves addressing various health issues as they arise, such as growth hormone deficiency, hypogonadism, obesity, diabetes mellitus, sleep apnea, behavioral problems, and cardiovascular complications [14,15]. There is no cure for PWS, and the current treatments are mainly symptomatic and supportive [16]. However, recent advances in understanding the genetic mechanisms underlying PWS have opened new avenues for potential genetic and epigenetic therapies that could restore the expression of the silenced genes or modulate their downstream effects [17,18]. Further research is needed to explore the safety and efficacy of these novel approaches in PWS patients.
Conclusions
The intricacies presented in this case highlight the complexities faced by individuals with PWS and underscore the importance of a multidisciplinary approach when managing such patients. Illustrated in this report are the dedications and resilience held by a multidisciplinary team, demonstrating how these efforts help in delivering quality healthcare. Further need for research and investigation into various treatment modalities for PWS is crucial for improving long-term outcomes, particularly in the fields of genetics and epigenetic therapies. We present this to stimulate further interest and investigation into this syndrome, ultimately leading to enhanced quality healthcare delivery for these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prader-Willi syndrome: a review of clinical, genetic, and endocrine findings J Endocrinol Invest Angulo MA Butler MG Cataletto ME 124912633820152606251710.1007/s 40618-015-0312-9PMC 4630255 · doi ↗ · pubmed ↗
- 2Prader-Willi syndrome - clinical genetics, diagnosis and treatment approaches: an update Curr Pediatr Rev Butler MG Miller JL Forster JL 2072441520193133312910.2174/1573396315666190716120925 PMC 7040524 · doi ↗ · pubmed ↗
- 3Prader-Willi syndrome: Molecular mechanism and epigenetic therapy Curr Gene Ther Mian-Ling Z Yun-Qi C Chao-Chun Z 36432020203232968510.2174/1566523220666200424085336 · doi ↗ · pubmed ↗
- 4Cardiac evaluation in children with Prader-Willi syndrome Acta Paediatr Marcus KA van Alfen-van der Velden JA Otten BJ Weijers G Yntema HG de Korte CL Kapusta L 031101201210.1111/j.1651-2227.2011.02570.x 22181352 · doi ↗ · pubmed ↗
- 5Subtle cardiovascular abnormalities in Prader-Willi syndrome might begin in young adulthood Internal Med Kobayashi S Murakami N Oto Y 337733846020213471962410.2169/internalmedicine.7073-21PMC 8627814 · doi ↗ · pubmed ↗
- 6CD 16(+) monocytes are involved in the hyper-inflammatory state of Prader-Willi syndrome by single-cell transcriptomic analysis Front Immunol Xu Y Hou X Guo H 11537301420233725138010.3389/fimmu.2023.1153730 PMC 10213932 · doi ↗ · pubmed ↗
- 7Prader-Willi syndrome: a nest for premature coronary artery disease?BMJ Case Rep Brás DR Semedo P Piçarra BC Fernandes R 02018201810.1136/bcr-2017-222828 PMC 583664129437709 · doi ↗ · pubmed ↗
- 8Vagal asystoles in a boy with Prader-Willi syndrome Pediatrics Thomas C Mandilaras G Rabenhorst D Oberhoffer FS Fischer M Haas NA Rodriguez SF 58216152202310.1542/peds.2022-05821637539482 · doi ↗ · pubmed ↗