Left Upper Extremity Pain, Right Coronary Artery Culprit: A Puzzling Path to Aneurysm Discovery
Moath Said Alfawara, Vivek Modi, Min-Fang Chao, Malek Nayfeh, Fares Alahdab, Mahmoud Alrifai, Mouaz Al-Mallah

TL;DR
This paper presents a rare case of a giant coronary artery aneurysm in an adult, highlighting its unusual presentation and potential complications.
Contribution
The novelty lies in reporting a rare adult case of GCA with a focus on its clinical presentation and management.
Findings
Giant coronary artery aneurysm (GCA) is rare and often asymptomatic.
GCAs can lead to severe complications like myocardial infarction or sudden death.
The case involved a GCA in the right coronary artery in an adult patient.
Abstract
Giant coronary artery aneurysm (GCA) is a rare disease afflicting 0.2% of the population. It is primarily attributed to atherosclerosis in adults and Kawasaki disease in children. Other uncommon etiologies include Takayasu arteritis and post-percutaneous coronary intervention.1,2 GCA lacks a universally accepted definition, with proposed criteria including a diameter exceeding 2 cm, 5 cm, or four times the normal vessel size.3 While the majority of GCAs are asymptomatic, a subset of patients present with angina, myocardial infarction from embolization or compression, heart failure due to fistula formation, or even sudden death.1 We report a case of an adult harboring a GCA involving the right coronary artery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
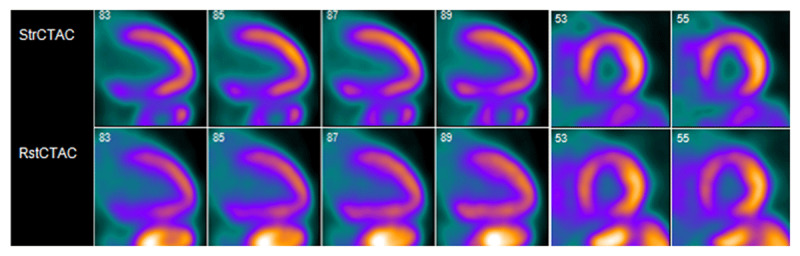 Figure 1
Figure 1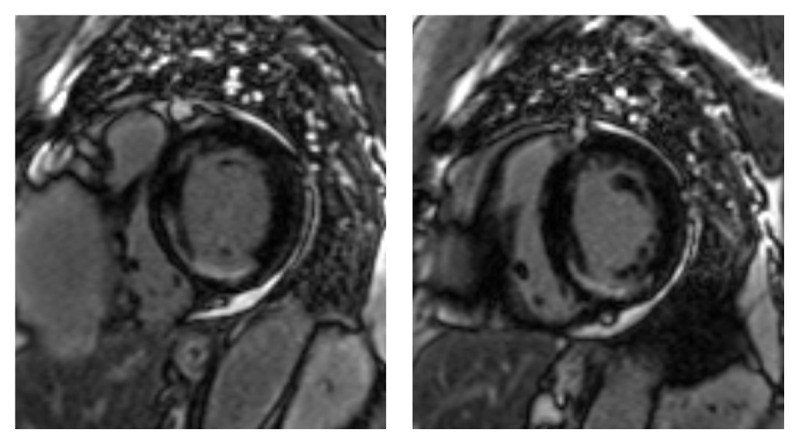 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
Case Presentation
A 71-year-old male with a medical history of hypertension, hyperlipidemia, and obstructive sleep apnea presented to the emergency department (ED) on multiple occasions with left upper extremity pain. The patient has a family history of premature coronary artery disease, with his father having undergone coronary artery bypass grafting in his 50s. The patient’s pain was initially persistent but later became intermittent. He described it as a pressure-like sensation radiating to the lower left arm, exacerbated by exertion and alleviated by rest. The pain was not accompanied by any other cardiac or respiratory symptoms. Electrocardiogram did not show any ischemic changes. Serial high-sensitivity troponins remained normal. Echocardiography revealed a hypokinetic inferior wall with a rounded structure adjacent to and slightly compressing the right atrium (Video 1).
Subcostal echocardiography view showing a rounded structure measuring 6.8 cm in diameter adjacent to and slightly compressing the right atrium; see also at https://youtube.com/shorts/k97OoTMpAbo.
Subsequently, positron emission tomography pharmacological stress testing demonstrated an infarct with peri-infarct ischemia in basal to mid inferior and inferoseptal walls (Figure 1). The patient underwent cardiac catheterization, which revealed an aneurysmal left coronary system. There was an unusual posterior takeoff of an ectatic right coronary artery (RCA) that could not be completely opacified (Video 2).
Cardiac positron emission tomography showing a medium-sized, moderate-severity, partially reversible defect in the proximal and mid inferior and inferoseptal segments.
Coronary angiogram showing an ectatic left coronary system and an incompletely opacified ectatic proximal right coronary artery; see also at https://youtube.com/shorts/0ssjghqx5sM.
Cardiac computed tomography revealed a giant aneurysm of the RCA measuring 9 × 11 cm that originated from the posterior aspect of the right-coronary cusp closer to the non-coronary cusp. The proximal RCA was patent, with a small jet of contrast extending into the cephalad portion of the aneurysm sac posteriorly. The aneurysm was compressing the right atrium (Video 3). Cardiac magnetic resonance imaging confirmed an aneurysmal RCA and revealed subendocardial late gadolinium enhancement in the basal and mid-inferior segments, indicating partial viability of RCA territory (Figure 2).
Cardiac computed tomography angiography sagittal view showing a giant retrosternal right coronary artery aneurysm extending from the proximal to distal segment, compressing the right atrium; see also at https://youtu.be/HMw3lXG_90c.
Late gadolinium enhancement cardiac magnetic resonance imaging showing left ventricular subendocardial scar in the basal and mid inferior and inferoseptal walls consistent with right coronary artery related myocardial infarction.
Due to recurrent anginal symptoms requiring multiple ED visits, a multidisciplinary decision was made for resection of the aneurysm and bypass of RCA. Intraoperatively, an ectatic proximal RCA was seen feeding into the aneurysmal sac, and a rather small RCA was seen exiting the aneurysmal sac. The patient underwent surgical excision of the aneurysm, and the distal RCA was dissected and ligated. The posterior descending artery was opened and grafted end-to-side with a saphenous vein. The resected aneurysm was sent for pathology, which revealed a myxoid degeneration of the media. The patient successfully underwent cardiac rehabilitation with no recurrence of anginal symptoms at the 6-month follow-up.
Discussion
While giant coronary artery aneurysms (GCAs) can manifest in any coronary artery, a propensity for the RCA, especially proximally, has been documented.^4,5^ Due to the rarity of GCAs, there are no large, randomized studies to guide management decisions. Surgical techniques such as ligation with bypass, isolated bypass, and plication are preferred for large aneurysms that present with mass effect or pose a high risk of rupture or distal thromboembolism.^1,3^ Successful short-term conservative management with warfarin and antianginals has been reported in asymptomatic patients.^6^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cohen P, O’Gara PT. Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev. 2008 Nov-Dec;16(6):301-4. doi: 18923233 10.1097/CRD.0b 013e 3181852659 · doi ↗ · pubmed ↗
- 2Falsetti HL, Carroll RJ. Coronary artery aneurysm: A review of the literature with a report of 11 new cases. Chest. 1976 May;69(5):630-6. doi: 1083790 10.1378/chest.69.5.630 · doi ↗ · pubmed ↗
- 3Jha NK, Ouda HZ, Khan JA, Eising GP, Augustin N. Giant right coronary artery aneurysm- case report and literature review. J Cardiothorac Surg. 2009 May 1;4:18. doi: 19405985 10.1186/1749-8090-4-18PMC 2688487 · doi ↗ · pubmed ↗
- 4Keyser A, Hilker MK, Husser O, Diez C, Schmid C. Giant coronary aneurysms exceeding 5 cm in size. Interact Cardiovasc Thorac Surg. 2012 Jul;15(1):33-6. doi: 22505591 10.1093/icvts/ivs 111PMC 3380987 · doi ↗ · pubmed ↗
- 5Manginas A, Cokkinos DV. Coronary artery ectasias: imaging, functional assessment and clinical implications. Eur Heart J. 2006 May;27(9):1026-31. doi: 16415301 10.1093/eurheartj/ehi 725 · doi ↗ · pubmed ↗
- 6Wessly P, Soherwardi S, Allen N. Nonsurgical Management of a Giant Coronary Artery Aneurysm. Cureus. 2017 Jul 16;9(7):e 1478. doi: 28944117 10.7759/cureus.1478 PMC 5602375 · doi ↗ · pubmed ↗