Acute Mesenteric Ischemia Secondary to Candida Endocarditis: A Case Report
Tatsuya Ochi, Shota Kikuta, Takeshi Nishimura, Satoshi Ishihara

TL;DR
A 36-year-old man developed acute bowel and organ damage from a rare fungal infection of the heart, which was successfully treated with surgery and antifungal drugs.
Contribution
This is the first reported case of acute mesenteric ischemia caused by Candida endocarditis.
Findings
Acute mesenteric ischemia was caused by a fungal infection of the heart valve (Candida tropicalis).
The patient recovered after surgical valve replacement and antifungal therapy.
Clinicians should consider infective endocarditis as a cause of mesenteric ischemia in patients without traditional risk factors.
Abstract
A 36-year-old man presented with abdominal pain, vomiting, and diarrhea. On arrival, his vital signs were remarkable for fever (39.3 °C) and tachycardia (127 beats/min, regular). His abdomen was distended, and a blood test showed elevations of inflammatory markers. Contrast-enhanced computed tomography revealed a superior mesenteric artery thrombus, ischemic colitis, ascites, and infarctions in the spleen and right kidney. He was diagnosed with bowel necrosis due to acute mesenteric ischemia (AMI). An emergent laparotomy was performed. The following day, Candida tropicalis was identified in the blood culture. In addition, transthoracic echocardiography revealed vegetation on the mitral valve leaflet. These findings were suggestive of infective endocarditis (IE) caused by C. tropicalis (Candida endocarditis); thus, the patient underwent surgical mitral valve replacement with the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
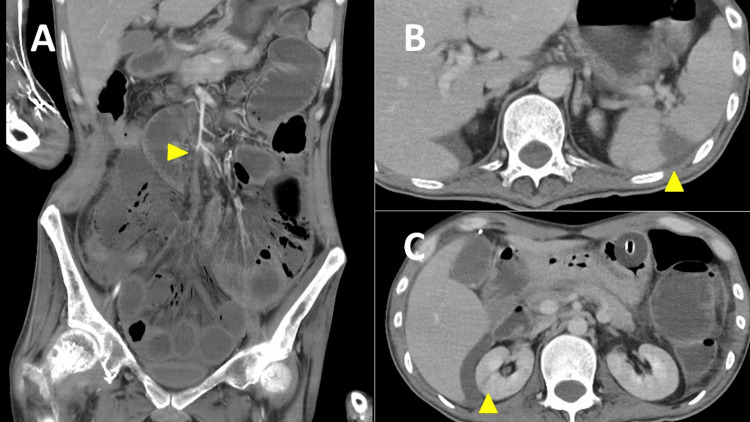 Figure 1
Figure 1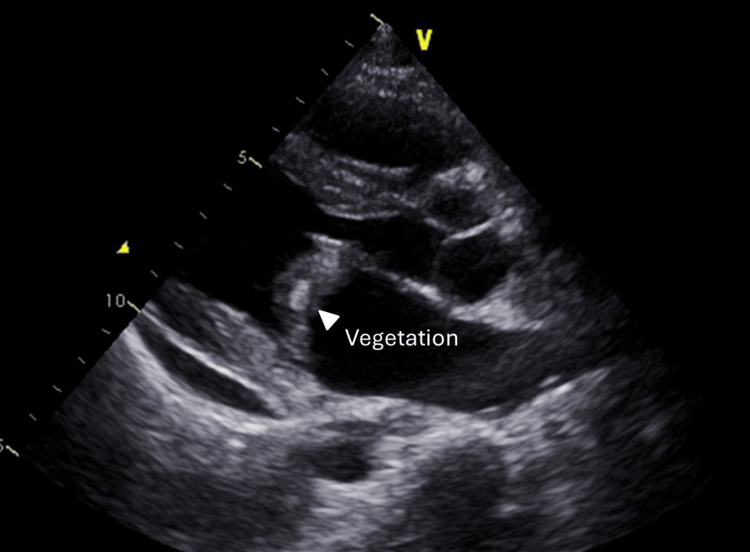 Figure 2
Figure 2| Laboratory Parameters | Patient's values | Reference range |
| White blood cell (WBC) | 24,700/mm3 | 3,300-8,600/mm3 |
| Neutrophils | 93.5% | 32.0-75.0% |
| Lymphocytes | 2.6% | 18.0-47.0% |
| Monocytes | 3.7% | 2.0-8.0% |
| Eosinophils | 0.1% | < 7% |
| Basophils | 0.1% | < 1% |
| Hemoglobin | 8.8 g/dL | 13.7-16.8 g/dL |
| Platelet | 115,000/mm3 | 158,000-348,000/mm3 |
| Serum albumin | 2.0 g/dL | 3.8-5.1 g/dL |
| C-reactive protein | 40.69 mg/dL | < 0.3 mg/dL |
| Fibrinogen | > 700 mg/dL | 200 - 400 mg/dL |
| Prothrombin time (PT) | 15.9 seconds | 10.0-13.5 seconds |
| Activated partial thromboplastin time (APTT) | 87.2 seconds | 24.0-39.0 seconds |
| Fibrin degradation products (FDP) | 15.6 µg/mL | < 5.0 µg/mL |
| D-dimer | < 1.0 µg/mL | < 1.0 µg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Pericarditis and Cardiac Tamponade · Infectious Aortic and Vascular Conditions
Introduction
Acute mesenteric ischemia (AMI), characterized by sudden hypoperfusion in the small intestine, is a life-threatening condition [1,2]. The etiologies of AMI include embolic, thrombotic, and non-obstructive causes, with embolic mechanisms being the most common [1,2]. In rare instances, mesenteric embolism and AMI can result from infective endocarditis (IE) [3,4]. Such cases require prompt diagnosis and comprehensive treatment involving medical, surgical, and cardiothoracic interventions [3]. Nevertheless, due to its rarity, literature on AMI associated with IE is scarce, leaving optimal management uncertain. We present a unique and instructive case of AMI complicated by Candida endocarditis.
Case presentation
A 36-year-old man was transferred to our hospital due to fever, vomiting, and diarrhea. He had previously been treated for* Candida*-associated central venous catheter infection with catheter removal and antifungal therapy, which was completed three months prior. Upon arrival, his vital signs were as follows: blood pressure of 111/66 mmHg, heart rate of 127 beats/min and regular, respiratory rate of 21 breaths/min, and body temperature of 39.3 °C. Physical examination revealed abdominal distension. An electrocardiogram showed sinus tachycardia. The laboratory findings were significant, indicating increases in neutrophil-dominant leukocytosis, anemia, thrombocytopenia, elevated C-reactive protein levels, and coagulation abnormalities (Table 1). Contrast-enhanced computed tomography conducted at the referring hospital revealed thrombosis at the superior mesenteric artery (SMA), accompanied by small bowel ischemia, ascites, and infarctions in the spleen and right kidney (Figures 1A-1C).
Contrast-enhanced computed tomography showing a superior mesenteric artery thrombus, ischemic colitis, ascites, and infarctions in the spleen and right kidney.
Based on these findings, the patient was diagnosed with bowel necrosis due to AMI. An emergent laparotomy was performed. During surgery, necrosis of the ileum and impaired palpation of the ileocolic artery were observed, leading to a procedure involving resection of the small intestine and ileocecal region. The following day, two sets of blood cultures drawn upon the patient’s arrival yielded positive results for* Candida* species, subsequently identified as Candida tropicalis. In addition, transthoracic echocardiography revealed mitral valve vegetation measuring 23 × 13 mm (Figure 2).
Transthoracic echocardiography showing vegetation on the mitral valve leaflet.
These findings suggested IE due to* C. tropicalis* (Candida endocarditis); therefore, the patient underwent surgical mitral valve replacement and initiation of antifungal therapy. A heart valve culture identified C. tropicalis, which was the same organism grown from the blood cultures. Screening tests did not reveal a condition resulting in a hypercoagulable state, such as protein C/S deficiency, antithrombin III deficiency, or antiphospholipid antibody syndrome. The patient received postoperative intensive care and was administered six weeks of intravenous antifungal agent (Micafungin) followed by three months of chronic suppressive therapy (oral Voriconazole), resulting in complete resolution without complications.
Discussion
The presented case exemplifies the diagnostic complexity associated with IE, particularly when it presents atypical manifestations such as AMI, thereby complicating its recognition. IE often arises due to complications from septic embolism, which may mimic localized ischemia, bleeding, organ failure, infections, and even systemic vasculitis [5,6]. Consequently, the diagnosis of IE tends to be delayed, which can lead to poorer outcomes and increased mortality [7].
Patients with IE are well known to be at increased risk of arterial thromboembolic events [8,9]. However, the occurrence of AMI as a complication, as observed in this case, is uncommon. In a previous report of 68 IE patients, 35 experienced embolic complications, of which only one involved mesenteric artery embolization [4]. Moreover, instances of Candida endocarditis complicating AMI are unprecedented in the literature, underscoring the uniqueness of the present case.
On the patient’s day of admission, we identified no apparent risk factors for embolic AMI, such as a history of arrhythmias, valvular disease, or coronary heart disease [10], leaving its cause unknown. Fortunately, the following day, the growth of Candida spp. was identified from blood cultures obtained upon admission, prompting consideration of* Candida* endocarditis as the cause of AMI. A subsequent transthoracic echocardiogram confirmed the diagnosis of Candida endocarditis, leading to definitive therapy including mitral valve replacement surgery and initiation of antifungal therapy. This clinical course implies the importance of considering diagnostic testing for IE, such as blood culture and echocardiography, when encountering AMI in the absence of other common etiologies.
Conclusions
This case highlights an exceedingly rare occurrence of AMI due to Candida endocarditis. It suggests the necessity for clinicians to consider IE as a potential cause of AMI where the etiology is unclear and common causes of embolism are not evident. We believe that these findings will contribute to an appropriate approach to similar cases in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evolution in the presentation, treatment, and outcomes of patients with acute mesenteric ischemia Ann Vasc Surg Chou EL Wang LJ Mc Lellan RM 53627420213382326310.1016/j.avsg.2021.01.116PMC 8349780 · doi ↗ · pubmed ↗
- 2Predictive factors of intestinal necrosis in acute mesenteric ischemia: prospective study from an intestinal Stroke Center Am J Gastroenterol Nuzzo A Maggiori L Ronot M 59760511220172826659010.1038/ajg.2017.38 · doi ↗ · pubmed ↗
- 3Lessons of the month 1: mesenteric ischaemia secondary to infective endocarditis Clin Med (Lond) Quek E Monkman B Madani Y 2822842220223558482010.7861/clinmed.2022-0044 PMC 9135078 · doi ↗ · pubmed ↗
- 4Incidence and prognosis of embolic events and metastatic infections in infective endocarditis Eur Heart J Millaire A Leroy O Gaday V 677684181997912990110.1093/oxfordjournals.eurheartj.a 015315 · doi ↗ · pubmed ↗
- 52023 ESC guidelines for the management of endocarditis Eur Heart J Delgado V Ajmone Marsan N de Waha S 394840424420233762265610.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 6Infective endocarditis mimicking ANCA-associated vasculitis: does it require immunosuppressive therapy?: a case report and literature review Medicine (Baltimore) Shi XD Li WY Shao X Qu LM Jiang ZY 099202010.1097/MD.0000000000021358 PMC 737352832702934 · doi ↗ · pubmed ↗
- 7Clinical characteristics and outcome of patients with infective endocarditis diagnosed in a Department of Internal Medicine J Clin Med Kreitmann L Montaigne D Launay D 864920203224519610.3390/jcm 9030864 PMC 7141516 · doi ↗ · pubmed ↗
- 8Echocardiography predicts embolic events in infective endocarditis J Am Coll Cardiol Shapiro S Kupferwasser LI 107710793720011126361110.1016/s 0735-1097(01)01149-4 · doi ↗ · pubmed ↗