A Case of Idiopathic Multicentric Castleman’s Disease Diagnosed From Anemia and Renal Dysfunction on an Annual Check-Up
Sayato Fukui, Rikako Yokokura, Jura Oshida, Taisuke Kodama, Daiki Kobayashi

TL;DR
A 34-year-old man was diagnosed with idiopathic multicentric Castleman's disease after showing symptoms of anemia and kidney issues during a routine check-up.
Contribution
This case highlights the importance of considering iMCD in patients with unexplained anemia and renal dysfunction.
Findings
The patient exhibited anemia, renal dysfunction, and elevated immunoglobulins without monoclonal patterns.
Lymph node biopsy confirmed the diagnosis of idiopathic multicentric Castleman's disease.
The case emphasizes the need for thorough evaluation in patients with atypical symptoms.
Abstract
A 34-year-old man was referred to our hospital because of mild renal dysfunction and anemia. He had no specific preexisting medical conditions; his complaint was fatigue. Physical examination revealed several mobile, pinky head-sized (no tenderness) palpable lymph nodes on the bilateral neck. Blood biochemistry tests revealed anemia, renal dysfunction, increased inflammation, and a protein-albumin discrepancy. Immunological examination revealed polyclonal elevation of immunoglobulins (no shift in κ/λ ratio). A cervical lymph node biopsy was performed, and the pathological results showed numerous clusters of mature plasma cells (plasmacytic type), leading to the definitive diagnosis of idiopathic multicentric Castleman's disease (iMCD).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
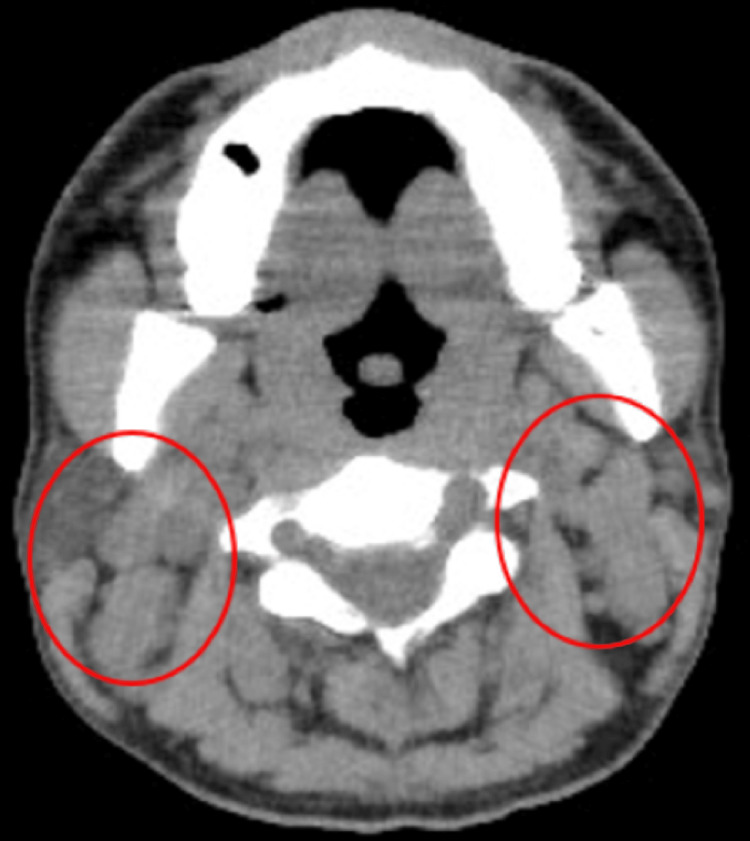 Figure 1
Figure 1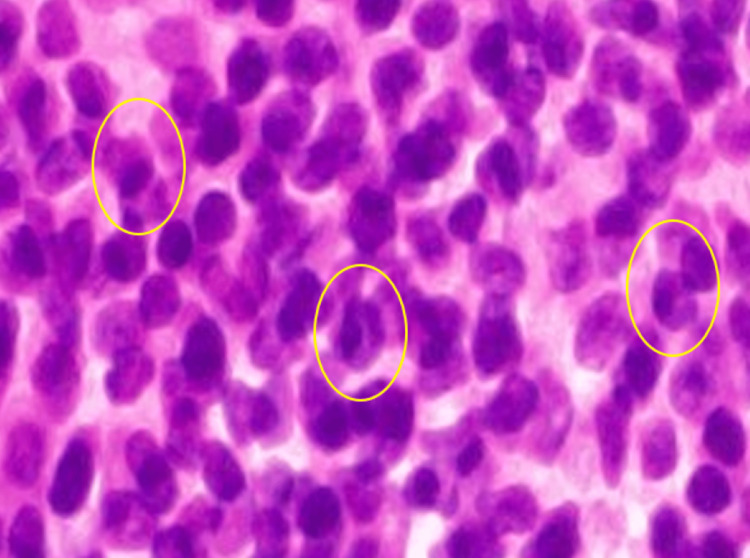 Figure 2
Figure 2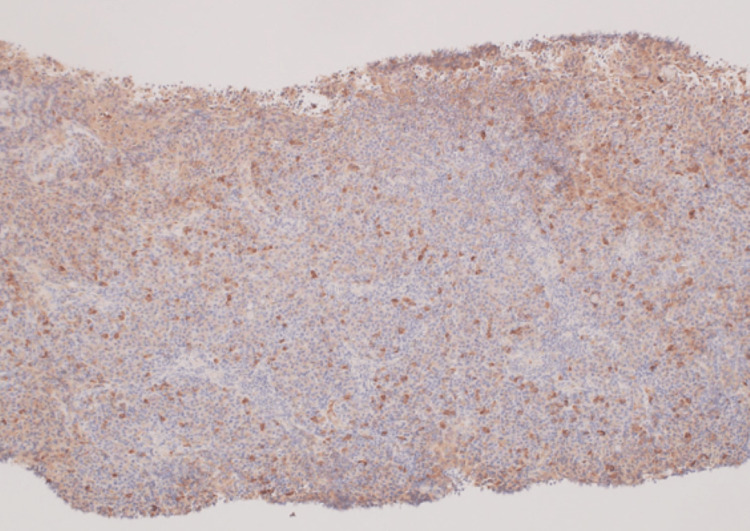 Figure 3
Figure 3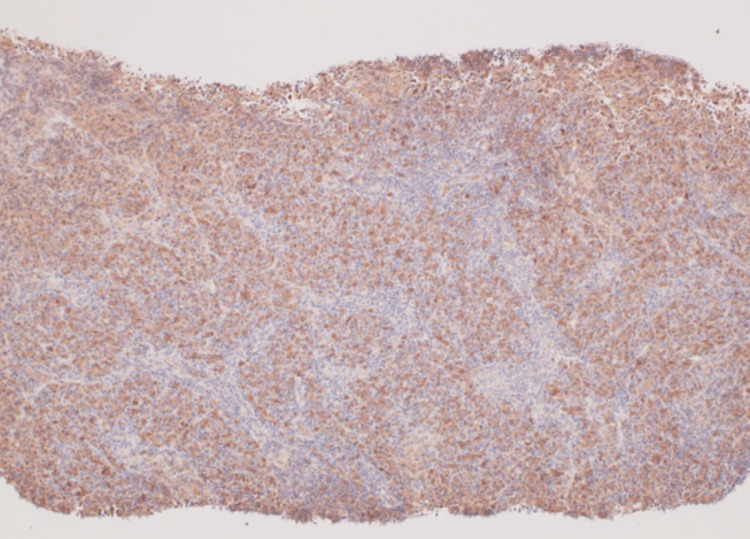 Figure 4
Figure 4| Blood test | Result | Normal range |
| White blood cells (/μL) | 9,000 | (4,000–8,000) |
| Neutrophils (%) | 72.6 | (40.0–75.0) |
| Lymphocytes (%) | 15.9 | (30.0–50.0) |
| Red blood cells (/μL) | 3.31 × 106 | (4.35 × 106–5.55 × 106) |
| Hemoglobin (g/dL) | 8.0 | (12.0–16.0) |
| Hematocrit (%) | 27.1 | (37.0–47.0) |
| Mean corpuscular volume (μ) | 81.9 | (88.0–99.0) |
| Mean corpuscular hemoglobin (pg) | 24.2 | (29–35) |
| Mean corpuscular hemoglobin concentration (%) | 29.5 | (29–35) |
| Red cell distribution width (fL) | 45.2 | (35.2–50.5) |
| Reticulocyte (‰) | 8.5 | (5–20) |
| Platelets (/μL) | 37.8 × 104 | (13.0 × 104–35.0 × 104) |
| Total protein (g/dL) | 10.4 | (6.7–8.3) |
| Albumin (g/dL) | 2.6 | (3.8–5.3) |
| Total bilirubin (mg/dL) | 0.4 | (0.2–1.0) |
| Aspartate aminotransferase (IU/L) | 15 | (12.0–32.0) |
| Alanine aminotransferase (IU/L) | 15 | (8.0–36.0) |
| Lactate dehydrogenase (IU/L) | 127 | (127.0–221.0) |
| Creatine kinase (IU/L) | 47 | (50.0–206.0) |
| Blood urea nitrogen (mg/dL) | 14.6 | (8.0–20.0) |
| Creatinine (mg/dL) | 1.21 | (0.65–1.07) |
| Sodium (mEq/L) | 139 | (134.0–147.0) |
| Potassium (mEq/L) | 4.0 | (3.2–4.8) |
| Chloride (mEq/L) | 102 | (98–108) |
| C-reactive protein (mg/dL) | 7.90 | (0.0–0.3) |
| Blood sedimentation rate (1 h value) (mm) | >140 | |
| Prothrombin time (s) | 15.0 | (9.5–13.5) |
| Activated partial thromboplastin time (s) | 34.8 | (24.0–32.0) |
| Immunoglobulin G (mg/dL) | 5196.1 | (861–1747) |
| Immunoglobulin A (mg/dL) | 689.3 | (93–393) |
| Immunoglobulin M (mg/dL) | 317.9 | (33–183) |
| κ-chain (mg/L) | 332 | (3.3–19.4) |
| λ-chain (mg/L) | 140 | (5.7–26.3) |
| κ/λ ratio | 2.37 | (0.26–1.65) |
| Soluble interleukin receptor (U/mL) | 2450 | (157–474) |
| β2-microglobulin (mg/L) | 3.89 | (0–2) |
| HIV screening test | negative | negative |
| Blood test | Result | Normal range |
| Interleukin-6 (IL-6) (pg/mL) | 23.4 | (<7.0) |
| HHV-8 DNA quantification (copy) | <2.0 × 101 | (<2.0 × 101) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Eosinophilic Disorders and Syndromes · Lymphoma Diagnosis and Treatment
Introduction
Castleman's disease (CD) is a rare lymphoproliferative disease. The CD was first reported as a disease of unknown cause by American pathologist Dr. Benjamin Castleman in 1956 and was named Castleman's disease [1]. CD is characterized by nonclonal lymph node hyperplasia [2]. It is classified as a hyaline, vascular, plasmacytic, or mixed cellularity type and may adopt a unicentric or multicentric presentation [2]. An association between the disease and human immunodeficiency virus (HIV) infection has been reported [2]. Human herpes virus 8 (HHV8) causes CD in immunosuppressed patients, including those infected with HIV (2). The cause of HHV8-negative multicentric CD is idiopathic and is called idiopathic multicentric Castleman's disease (iMCD) [3]. iMCD is a poorly understood lymphoproliferative disorder driven by hypercytokinemia. Patients have heterogeneous clinical features and characteristic lymph node histopathology. And multiple organ dysfunction occurs as it progresses [4]. In Japan, it is designated an intractable disease, and according to statistics from the Japan Intractable Diseases Information Center, the number of patients in Japan is approximately 1,500.
This case report describes a rare case in which the patient did not present to the hospital with multiorgan failure, as described above, but was diagnosed with renal dysfunction and anemia during an annual check-up.
Case presentation
A 34-year-old man was referred to our hospital because of mild renal dysfunction and anemia during an annual check-up in 2023. The annual check-up in 2022 showed no renal function or anemia. However, the current blood test in 2023 showed creatinine of 1.37 mg/dL and hemoglobin of 8.5 g/dL.
He had no specific preexisting medical conditions; his chief complaint was fatigue. When he visited our hospital, his vital signs were normal, and a physical examination revealed several mobile, pinky-head-sized (no tenderness) lymph nodes on the bilateral neck. Other than this, no other obvious abnormal findings, including splenomegaly, were evident upon physical examination. Blood biochemistry tests revealed anemia, renal dysfunction, increased inflammation, and a protein-albumin discrepancy. Immunological examination revealed polyclonal elevation of immunoglobulins (no shift in κ/λ ratio) (Table 1).
Table 1: Blood and biochemistry test resultsHIV: human immunodeficiency virus
<table><tbody><tr><td rowspan="1" colspan="1">Blood test</td><td rowspan="1" colspan="1">Result</td><td rowspan="1" colspan="1">Normal range</td></tr><tr><td rowspan="1" colspan="1">White blood cells (/μL)</td><td rowspan="1" colspan="1">9,000</td><td rowspan="1" colspan="1">(4,000–8,000)</td></tr><tr><td rowspan="1" colspan="1">Neutrophils (%)</td><td rowspan="1" colspan="1">72.6</td><td rowspan="1" colspan="1">(40.0–75.0)</td></tr><tr><td rowspan="1" colspan="1">Lymphocytes (%)</td><td rowspan="1" colspan="1">15.9</td><td rowspan="1" colspan="1">(30.0–50.0)</td></tr><tr><td rowspan="1" colspan="1">Red blood cells (/μL)</td><td rowspan="1" colspan="1">3.31 × 10<sup>6</sup> </td><td rowspan="1" colspan="1">(4.35 × 10<sup>6</sup>–5.55 × 10<sup>6</sup>)</td></tr><tr><td rowspan="1" colspan="1">Hemoglobin (g/dL)</td><td rowspan="1" colspan="1">8.0</td><td rowspan="1" colspan="1">(12.0–16.0)</td></tr><tr><td rowspan="1" colspan="1">Hematocrit (%)</td><td rowspan="1" colspan="1">27.1</td><td rowspan="1" colspan="1">(37.0–47.0)</td></tr><tr><td rowspan="1" colspan="1">Mean corpuscular volume (μ)</td><td rowspan="1" colspan="1">81.9</td><td rowspan="1" colspan="1">(88.0–99.0)</td></tr><tr><td rowspan="1" colspan="1">Mean corpuscular hemoglobin (pg)</td><td rowspan="1" colspan="1">24.2</td><td rowspan="1" colspan="1">(29–35)</td></tr><tr><td rowspan="1" colspan="1">Mean corpuscular hemoglobin concentration (%)</td><td rowspan="1" colspan="1">29.5</td><td rowspan="1" colspan="1">(29–35)</td></tr><tr><td rowspan="1" colspan="1">Red cell distribution width (fL)</td><td rowspan="1" colspan="1">45.2</td><td rowspan="1" colspan="1">(35.2–50.5)</td></tr><tr><td rowspan="1" colspan="1">Reticulocyte (‰)</td><td rowspan="1" colspan="1">8.5</td><td rowspan="1" colspan="1">(5–20)</td></tr><tr><td rowspan="1" colspan="1">Platelets (/μL)</td><td rowspan="1" colspan="1">37.8 × 10<sup>4</sup> </td><td rowspan="1" colspan="1">(13.0 × 10<sup>4</sup>–35.0 × 10<sup>4</sup>)</td></tr><tr><td rowspan="1" colspan="1">Total protein (g/dL)</td><td rowspan="1" colspan="1">10.4</td><td rowspan="1" colspan="1">(6.7–8.3)</td></tr><tr><td rowspan="1" colspan="1">Albumin (g/dL)</td><td rowspan="1" colspan="1">2.6</td><td rowspan="1" colspan="1">(3.8–5.3)</td></tr><tr><td rowspan="1" colspan="1">Total bilirubin (mg/dL)</td><td rowspan="1" colspan="1">0.4</td><td rowspan="1" colspan="1">(0.2–1.0)</td></tr><tr><td rowspan="1" colspan="1">Aspartate aminotransferase (IU/L)</td><td rowspan="1" colspan="1">15</td><td rowspan="1" colspan="1">(12.0–32.0)</td></tr><tr><td rowspan="1" colspan="1">Alanine aminotransferase (IU/L)</td><td rowspan="1" colspan="1">15</td><td rowspan="1" colspan="1">(8.0–36.0)</td></tr><tr><td rowspan="1" colspan="1">Lactate dehydrogenase (IU/L)</td><td rowspan="1" colspan="1">127</td><td rowspan="1" colspan="1">(127.0–221.0)</td></tr><tr><td rowspan="1" colspan="1">Creatine kinase (IU/L)</td><td rowspan="1" colspan="1">47</td><td rowspan="1" colspan="1">(50.0–206.0)</td></tr><tr><td rowspan="1" colspan="1">Blood urea nitrogen (mg/dL)</td><td rowspan="1" colspan="1">14.6</td><td rowspan="1" colspan="1">(8.0–20.0)</td></tr><tr><td rowspan="1" colspan="1">Creatinine (mg/dL)</td><td rowspan="1" colspan="1">1.21</td><td rowspan="1" colspan="1">(0.65–1.07)</td></tr><tr><td rowspan="1" colspan="1">Sodium (mEq/L)</td><td rowspan="1" colspan="1">139</td><td rowspan="1" colspan="1">(134.0–147.0)</td></tr><tr><td rowspan="1" colspan="1">Potassium (mEq/L)</td><td rowspan="1" colspan="1">4.0</td><td rowspan="1" colspan="1">(3.2–4.8)</td></tr><tr><td rowspan="1" colspan="1">Chloride (mEq/L)</td><td rowspan="1" colspan="1">102</td><td rowspan="1" colspan="1"> (98–108)</td></tr><tr><td rowspan="1" colspan="1">C-reactive protein (mg/dL)</td><td rowspan="1" colspan="1">7.90</td><td rowspan="1" colspan="1">(0.0–0.3)</td></tr><tr><td rowspan="1" colspan="1">Blood sedimentation rate (1 h value) (mm)</td><td rowspan="1" colspan="1">>140</td><td rowspan="1" colspan="1"> </td></tr><tr><td rowspan="1" colspan="1">Prothrombin time (s)</td><td rowspan="1" colspan="1">15.0</td><td rowspan="1" colspan="1">(9.5–13.5)</td></tr><tr><td rowspan="1" colspan="1">Activated partial thromboplastin time (s)</td><td rowspan="1" colspan="1">34.8</td><td rowspan="1" colspan="1">(24.0–32.0)</td></tr><tr><td rowspan="1" colspan="1">Immunoglobulin G (mg/dL)</td><td rowspan="1" colspan="1">5196.1</td><td rowspan="1" colspan="1">(861–1747)</td></tr><tr><td rowspan="1" colspan="1">Immunoglobulin A (mg/dL)</td><td rowspan="1" colspan="1">689.3</td><td rowspan="1" colspan="1">(93–393)</td></tr><tr><td rowspan="1" colspan="1">Immunoglobulin M (mg/dL)</td><td rowspan="1" colspan="1">317.9</td><td rowspan="1" colspan="1">(33–183)</td></tr><tr><td rowspan="1" colspan="1">κ-chain (mg/L)</td><td rowspan="1" colspan="1">332</td><td rowspan="1" colspan="1">(3.3–19.4)</td></tr><tr><td rowspan="1" colspan="1">λ-chain (mg/L)</td><td rowspan="1" colspan="1">140</td><td rowspan="1" colspan="1">(5.7–26.3)</td></tr><tr><td rowspan="1" colspan="1">κ/λ ratio</td><td rowspan="1" colspan="1">2.37</td><td rowspan="1" colspan="1">(0.26–1.65)</td></tr><tr><td rowspan="1" colspan="1">Soluble interleukin receptor (U/mL)</td><td rowspan="1" colspan="1">2450</td><td rowspan="1" colspan="1">(157–474)</td></tr><tr><td rowspan="1" colspan="1">β2-microglobulin (mg/L)</td><td rowspan="1" colspan="1">3.89</td><td rowspan="1" colspan="1">(0–2)</td></tr><tr><td rowspan="1" colspan="1">HIV screening test</td><td rowspan="1" colspan="1">negative</td><td rowspan="1" colspan="1">negative</td></tr></tbody></table>A computed tomography (CT) scan showed multiple enlarged bilateral cervical lymph nodes (Figure 1).
Computed tomography revealed multiple enlarged bilateral cervical lymph nodes (red circles)
At this point, lymphoproliferative diseases, including Castleman's disease (CD) and malignant lymphoid species, were listed as differential diagnoses, and a cervical lymph node biopsy was performed. Pathological results showed numerous clusters of mature plasma cells (Figure 2).
Cervical lymph node biopsyPlasma cells with nuclei predominantly located on one side were observed (inside the yellow circles) (Hematoxylin-Eosin stain; magnification ×400)
Immunostaining showed that all immunoglobulin staining was similar (no staining for specific immunoglobulins) (Figures 3, 4), ruling out plasmacytoma and suggesting multicentric Castleman's disease (plasmacytic type).
Immunoglobulin G immunostaining (overall stained) (×400)
Light chain κ immunostaining (overall stained) (×400)
Subsequently, additional blood tests showed elevated interleukin-6 (IL-6); 23.4 pg/mL (normal value; <7.0 pg/mL). In addition, human herpesvirus type 8 (HHV-8) DNA quantification was below detection sensitivity (Table 2).
Table 2: Additional blood test resultsHHV: human herpes virus
<table><tbody><tr><td rowspan="1" colspan="1">Blood test</td><td rowspan="1" colspan="1">Result</td><td rowspan="1" colspan="1">Normal range</td></tr><tr><td rowspan="1" colspan="1">Interleukin-6 (IL-6) (pg/mL)</td><td rowspan="1" colspan="1">23.4</td><td rowspan="1" colspan="1">(<7.0)</td></tr><tr><td rowspan="1" colspan="1">HHV-8 DNA quantification (copy)</td><td rowspan="1" colspan="1"><2.0 × 10<sup>1</sup> </td><td rowspan="1" colspan="1">(<2.0 × 10<sup>1</sup>)</td></tr></tbody></table>Furthermore, human immunodeficiency virus (HIV), autoimmune diseases, and malignant tumors were also excluded. These findings led to the definitive diagnosis of idiopathic multicentric Castleman's disease (iMCD).
Discussion
Idiopathic multicentric Castleman's disease (iMCD) is a group of poorly understood lymphoproliferative disorders driven by hypercytokinaemia [4]. Patients have heterogeneous clinical features (characteristic lymph node histopathology and multiple organ dysfunction as it progresses) [4]. Although the progression of symptoms is thought to be gradual, there have been reports of cases diagnosed after severe disease, leading to multiple organ failure [5,6]. The present case was diagnosed based on minor abnormal findings during an annual check-up and was considered early. The only symptom was fatigue. The patient did not have any B symptoms, nor was he aware of the swollen lymph nodes in his neck. Castleman's disease (CD) would not have been included in the differential diagnosis without imaging if lymphadenopathy had not been detected on physical examination. This finding suggests the importance of a thorough physical examination in all cases.
The characteristic clinical findings of iMCD include multicentric lymphadenopathy, anemia, elevated C-reactive protein level, hypergammaglobulinemia, hypoalbuminemia, elevated IL-6, hepatomegaly or splenomegaly, fever, edema, ascites, anasarca, or a combination of these [4]. In our case, there was no fever or pleural effusion; therefore, we believe the patient did not notice any unusual symptoms. However, the blood test results were typical. Furthermore, if thrombocytopenia presents with marked pleural effusion, TAFRO (thrombocytopenia, anasarca (edema, pleural effusion, and ascites), fever, reticulin myelofibrosis (or renal insufficiency), and organomegaly (hepatosplenomegaly and lymphadenopathy)) syndrome should be considered a differential diagnosis. Because lymph node histology is similar between TAFRO syndrome with CD, TAFRO syndrome is described as related to CD [7].
Additionally, there are reports of biomarker studies in which C-X-C motif chemokine ligand (CXCL)-13 has been identified and validated as the protein most prominently upregulated in iMCD [8]. Furthermore, increases in inflammatory cytokines (serum IL-10 and IL-23) and chemokines such as CXCL-10 and vascular endothelial growth factor (VEGF)-A have been observed. And their relationship with pathogenesis has attracted attention [9]. The usefulness of these markers suggests that CD is caused by a cytokine storm. A few case reports are available in which adverse reactions to vaccines were thought to have elicited cytokine storms [10].
Treatment inevitably involves a therapy that suppresses cytokinesis. Cytokine-targeted therapy is the basis of treatment with corticosteroid monotherapy and IL-6-targeted therapy (tocilizumab or siltuximab) [4,11]. Our patient is currently undergoing treatment at this stage.
Conclusions
We diagnosed the patient with idiopathic multicentric Castleman's disease (iMCD) at a relatively early stage. Diagnoses based on abnormalities during annual check-ups are rare. A detailed physical examination provided clues for the diagnosis.
On this day, and in the age of rapid developments in testing, including imaging tests, we were reminded again of the importance of detailed physical examination.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Case records of the Massachusetts General Hospital: case No. 40231 N Engl J Med CAB TOVW 1001100525019541316594410.1056/NEJM 195406102502308 · doi ↗ · pubmed ↗
- 2Castleman's disease. A review AIDS Rev Roca B 37112009 https://pubmed.ncbi.nlm.nih.gov/19290029/19290029 · pubmed ↗
- 3Idiopathic multicentric Castleman's disease: a systematic literature review Lancet Haematol Amy Y Liu Christopher S Nabel Brian S Finkelman 1631753201610.1016/S 2352-3026(16)00006-527063975 · doi ↗ · pubmed ↗
- 4The collaborative network approach: a new framework to accelerate Castleman's disease and other rare disease research Lancet Haematol David C Fajgenbaum Jason R Ruth Dermot Kelleher Rubenstein AH 1501523201610.1016/S 2352-3026(16)00007-727063967 · doi ↗ · pubmed ↗
- 5Severe inflammatory idiopathic multicentric Castleman’s disease coexisting with advanced renal cancer: a case report Tohoku J Exp Med Chiba D Kawasaki Y Miyagi A 12713325720223541853310.1620/tjem.2022.J 025 · doi ↗ · pubmed ↗
- 6Remissions of different quality following rituximab, tocilizumab and rituximab, and allogeneic stem cell transplantation in a patient with severe idiopathic multicentric Castleman's disease Ann Hematol Angenendt L Kerkhoff A Wiebe S 124112439420152579124310.1007/s 00277-015-2353-8 · doi ↗ · pubmed ↗
- 7Castleman disease and TAFRO syndrome Ann Hematol Masaki Y Arita K Sakai T Takai K Aoki S Kawabata H 48549010120223504451310.1007/s 00277-022-04762-6PMC 8768434 · doi ↗ · pubmed ↗
- 8CXCL 13 is a predictive biomarker in idiopathic multicentric Castleman disease Nat Commun Pierson SK Katz L Williams R 72361320223643399610.1038/s 41467-022-34873-7PMC 9700691 · doi ↗ · pubmed ↗