Parental Knowledge, Attitude, and Practice Toward Children’s Developmental Milestones in the Western Region of Saudi Arabia
Mohammed R. Alhayli, Ahmed A. Alhayli, Shatha M Alamri, Atheer M. Alamri, Jaber A Alfaifi, Mohsen H AlRashdi, Maryam H Almaqadi, Jawaher M Alamri, Abdulrahman R. Alhayli, Fahd Y. Somili

TL;DR
This study examines how well parents in Saudi Arabia's Western region understand their children's developmental milestones and the factors influencing their knowledge.
Contribution
The study provides new insights into parental knowledge gaps and influential factors in a specific Saudi region.
Findings
Most parents obtained information about child development from medical professionals.
Female parents showed higher awareness than male parents.
Divorced parents had lower awareness compared to widowed parents.
Abstract
Introduction: Parents' ability to engage and raise their children in a safe and appropriate manner is largely influenced by their knowledge of child development and childrearing. This study aimed to evaluate the parenting and developmental milestone (MS) knowledge of Western region Saudi parents and identify the related elements that influence their knowledge. Methods: This cross‑sectional study was conducted for a period of six months. Ethical approval was duly sanctioned by the Institutional Review Board (IRB), and prior to participation, written informed consent was diligently procured from all the individuals involved in the study. In adherence to the paramount principles of privacy, rigorous measures were employed to de‑identify the personal data of the participants, thereby safeguarding their confidentiality and anonymity. All research procedures were meticulously executed in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
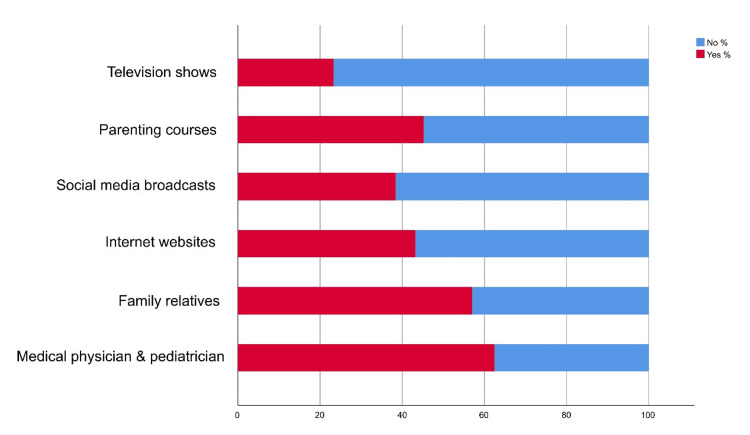 Figure 1
Figure 1| Category | N | % | |
| Gender | Male | 201 | 23.00% |
| Female | 672 | 77.00% | |
| Age | < 30 | 323 | 37.00% |
| 31-39 | 235 | 26.90% | |
| 40-49 | 226 | 25.90% | |
| 50-59 | 77 | 8.80% | |
| 60 or more | 12 | 1.40% | |
| Marital status | Single | 198 | 22.70% |
| Married | 635 | 72.70% | |
| Divorced | 29 | 3.30% | |
| Widowed | 11 | 1.30% | |
| Nationality | Saudi | 772 | 88.40% |
| Non-Saudi | 101 | 11.60% | |
| Geographical region | Northern | 0 | 0.00% |
| Southern | 97 | 11.10% | |
| Central | 39 | 4.50% | |
| Eastern | 51 | 5.80% | |
| Western | 686 | 78.60% | |
| Residency | Urban area | 700 | 80.20% |
| Rural area | 173 | 19.80% | |
| Educational level | Uneducated | 6 | 0.70% |
| Elementary | 12 | 1.40% | |
| Middle | 29 | 3.30% | |
| High school | 196 | 22.50% | |
| University | 582 | 66.70% | |
| Postgraduate | 48 | 5.50% | |
| Employment | Student | 138 | 15.80% |
| Unemployed | 287 | 32.90% | |
| Employed | 397 | 45.50% | |
| Entrepreneur | 12 | 1.40% | |
| Retired | 39 | 4.50% | |
| Monthly income | Less than 5000 | 398 | 45.60% |
| 5000-10000 | 275 | 31.50% | |
| More than 10000 | 200 | 22.90% |
| Parameter | Category | N | % |
| When does the infant start to move his head? | 1 week | 295 | 33.80% |
| 3 weeks | 263 | 30.10% | |
| 6 weeks | 156 | 17.90% | |
| 1 month | 159 | 18.20% | |
| When does the infant begin to turn over? | 1 month | 120 | 13.70% |
| 6 months | 669 | 76.60% | |
| 10 months | 65 | 7.40% | |
| 1 year | 19 | 2.20% | |
| When does the infant start to stand? | 8 months | 233 | 26.70% |
| 10 months | 474 | 54.30% | |
| 1 year and half | 150 | 17.20% | |
| 2 years | 16 | 1.80% | |
| When does the child walk alone steadily? | 10 months | 65 | 7.40% |
| 12 months | 337 | 38.60% | |
| 15 months | 295 | 33.80% | |
| 20 months | 176 | 20.20% | |
| When does the child start to climb stairs? | 12 months | 91 | 10.40% |
| 14 months | 121 | 13.90% | |
| 18 months | 274 | 31.40% | |
| 24 months | 387 | 44.30% | |
| When can a child follow things with his eyes? | At birth | 41 | 4.70% |
| 1 week | 214 | 24.50% | |
| 6 weeks | 519 | 59.50% | |
| 1 year | 99 | 11.30% | |
| When can a child approach an object? | 1 week | 14 | 1.60% |
| 1 month | 47 | 5.40% | |
| 6 months | 434 | 49.70% | |
| 1 year | 378 | 43.30% | |
| When can a child do manual skills like drawing? | 1 month | 18 | 2.10% |
| 6 months | 32 | 3.70% | |
| 1 year | 150 | 17.20% | |
| At 3 years and above | 673 | 77.10% |
| Parameter | Category | N | % |
| At what age does the child begin to respond to the mother's voice? | 1 week | 199 | 22.80% |
| 3 weeks | 266 | 30.50% | |
| 6 weeks | 231 | 26.50% | |
| 1 month | 177 | 20.30% | |
| At what age does a child start saying "Mama and Papa"? | 4 months | 73 | 8.40% |
| 6 months | 188 | 21.50% | |
| 8 months | 298 | 34.10% | |
| 10 months | 314 | 36.00% | |
| At what age does a child start smiling? | 6 weeks | 476 | 54.50% |
| 8 weeks | 212 | 24.30% | |
| 12 weeks | 98 | 11.20% | |
| 14 weeks | 66 | 7.60% | |
| 1 month | 8 | 0.90% | |
| 2 months | 13 | 1.50% | |
| At what age does a child begin to know his age and his name? | 1 year | 244 | 27.90% |
| 2 years | 271 | 31.00% | |
| 3 years | 240 | 27.50% | |
| 4 years | 118 | 13.50% | |
| At what age does a child start saying "bye-bye"? | 6 months | 111 | 12.70% |
| 10 months | 242 | 27.70% | |
| 1 year | 361 | 41.40% | |
| 2 years | 159 | 18.20% | |
| At what age can a child drink from a cup? | 12 months | 282 | 32.30% |
| 18 months | 290 | 33.20% | |
| 2 years | 234 | 26.80% | |
| 3 years | 67 | 7.70% | |
| At what age does a child begin to control urination? | 1 year | 46 | 5.30% |
| 2 years | 175 | 20.00% | |
| 3 years | 421 | 48.20% | |
| 4 years | 231 | 26.50% |
| Parameter | Category | Median (IQR) | p-value |
| Gender | Male | 5.0 (4.0-7.0) | < 0.001 |
| Female | 6.0 (5.0-7.0) | ||
| Age | < 30 | 6.0 (4.0-7.0) | < 0.001 |
| 31-39 | 6.0 (5.0-7.0) | ||
| 40-49 | 6.0 (5.0-7.0) | ||
| 50-59 | 6.0 (4.5-7.0) | ||
| 60 or more | 5.5 (3.25-7.0) | ||
| Marital status | Single | 6.0 (4.0-7.0) | 0.007 |
| Married | 6.0 (5.0-7.0) | ||
| Divorced | 5.0 (4.0-6.5) | ||
| Widowed | 6.0 (6.0-8.0) | ||
| Nationality | Saudi | 6.0 (5.0-7.0) | 0.768 |
| Non-Saudi | 6.0 (4.0-7.0) | ||
| Geographical region | Southern | 5.0 (3.0-7.0) | 0.044 |
| Central | 6.0 (5.0-7.0) | ||
| Eastern | 6.0 (5.0-7.0) | ||
| Western | 6.0 (5.0-7.0) | ||
| Residency | Urban area | 6.0 (5.0-7.0) | 0.599 |
| Rural area | 6.0 (4.0-7.0) | ||
| Educational level | Uneducated | 2.5 (0.75-6.75) | 0.109 |
| Elementary | 5.0 (4.0-6.75) | ||
| Middle | 6.0 (3.0-7.0) | ||
| High school | 6.0 (5.0-7.0) | ||
| University | 6.0 (5.0-7.0) | ||
| Postgraduate | 6.0 (5.0-8.0) | ||
| Employment | Student | 6.0 (4.0-7.0) | 0.079 |
| Unemployed | 6.0 (5.0-7.0) | ||
| Employed | 6.0 (5.0-7.0) | ||
| Entrepreneur | 5.5 (4.25-7.0) | ||
| Retired | 6.0 (4.0-7.0) | ||
| Monthly income | Less than 5000 | 6.0 (5.0-7.0) | 0.153 |
| 5000-10000 | 6.0 (4.0-7.0) | ||
| More than 10000 | 6.0 (5.0-7.0) |
| Parameter | Category | Beta | 95% CI | p-value | |
| LB | UB | ||||
| Gender | Male | -0.582 | -0.890 | -0.274 | < 0.001 |
| Female | Ref. | Ref. | Ref. | Ref. | |
| Age | < 30 | 0.230 | -0.916 | 1.377 | 0.693 |
| 31-39 | 0.968 | -0.168 | 2.103 | 0.095 | |
| 40-49 | 0.878 | -0.255 | 2.011 | 0.129 | |
| 50-59 | 0.352 | -0.821 | 1.525 | 0.556 | |
| 60 or more | Ref. | Ref. | Ref. | Ref. | |
| Marital status | Single | -0.863 | -2.080 | 0.355 | 0.165 |
| Married | -0.762 | -1.935 | 0.412 | 0.203 | |
| Divorced | -1.641 | -2.993 | -0.288 | 0.017 | |
| Widowed | Ref. | Ref. | Ref. | Ref. | |
| Geographical region | Southern | -0.234 | -0.653 | 0.186 | 0.275 |
| Central | 0.001 | -0.613 | 0.616 | 0.996 | |
| Eastern | -0.393 | -0.932 | 0.147 | 0.153 | |
| Western | Ref. | Ref. | Ref. | Ref. | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild and Adolescent Health · Childhood Cancer Survivors' Quality of Life · Ethics and Legal Issues in Pediatric Healthcare
Introduction
Parents' expectations of and interactions with their children are influenced by their understanding of and awareness of child development [1]. The literature has shown that a child's early life experiences play a significant role in shaping their future social skills, with the first five years of life being particularly critical for brain development [2].
Research conducted in industrialized nations revealed a significant correlation between a mother's capacity to improve her child's growth and her understanding of child development [3]. However, research indicates that parents who are ignorant about child development may overestimate their child's rate of development, which could result in unreasonable expectations, intolerance, and impatience [4].
A child's degree of achievement at a particular stage is indicated by the word "milestone" (MS). Because children develop at different rates, developmental MSs are not set in stone and have a typical range of variation. Developmental MSs serve as approximate indicators of when one can anticipate specific changes in a child's growth and development as they progress through different stages of childhood. Nevertheless, it is important to acknowledge the inherent variability in individual development, making it a challenging task to predict when a child will master a particular skill precisely [5].
Understanding early life MSs, continuous developmental processes, and being familiar with parenting techniques are all ways to gain knowledge about child development. Research from several industrialized nations revealed a significant correlation between mothers' increased capacity to support their children's development and their understanding of child development [6].
The ongoing process of developing and using the information and abilities necessary for organizing, conceiving, giving birth, raising, and taking care of children is referred to as "parenting" [6]. Proficient in their child's development, parents exhibit high levels of efficacy and competence in parenting. Conversely, even though they were effective parents, parents with insufficient information had insufficient parenting skills [7,8].
In the 1980s and 1990s of the previous century, child psychologists were concerned with developmental expectations and mothers' awareness of developmental MSs. This is why it is a common topic in Western literature [9]. Studies from the Arab world, Saudi Arabia included, are, on the other hand, rare. Thus, the purpose of this study was to evaluate Western Saudi parents' knowledge, attitudes, and practices regarding developmental MSs for infants, as well as the sociodemographic factors relevant to learning and the sources of information regarding these MSs.
Materials and methods
This cross‑sectional study and an online survey were sent to participants through a short message service (SMS). They explained the research and its purpose, with informed consent required before participating and completing the questionnaire. This study’s protocol with IRB number HAPO-02-K-012-2023-05-1628 was approved by the Institutional Review Board (IRB) of Umm Al-Qura University. Data de‑identification measures were employed to safeguard participant privacy, and research procedures adhered to relevant guidelines and regulations. The study included Saudi parents from the Western Province with children up to six years who provided informed consent. No age or ethnic origin restrictions were imposed. Exclusions comprised parents of infants with confirmed developmental abnormalities, complex perinatal and postnatal histories, and neurologically deficient infants, as these factors could skew developmental norm findings. Participant recruitment occurred through visits to Governmental Primary Healthcare Centers (PHCs) in the Western Province of Saudi Arabia. The total sample size was 873 using the purposive sampling technique during the study period.
Methodology
Data collection was executed through a questionnaire comprising three distinct sections. The initial section was designed to capture sociodemographic information, while the second section involved the administration of "The Knowledge of Infant Development Inventory (KIDI)," an instrument developed by David McPhee [10].
Before applying the KIDI tool in this study, formal permission to utilize it was sought and obtained from the original author. The KIDI tool, structured as a univariate scale consisting of 58 items, was specifically devised to evaluate an individual's knowledge pertaining to parenting practices and child developmental processes. The first 39 items of the original KIDI focused on assessing knowledge regarding normative child behaviors, requiring respondents to express their agreement, disagreement, or uncertainty regarding various statements. In the subsequent part (items 40-58), which centered on a child's developmental MSs, respondents were prompted to specify whether a younger or older child could attain a given developmental MS when expressing disagreement [10].
The KIDI instrument encompassed two segments, one dedicated to childrearing practices and the other to developmental MSs. The third section of the questionnaire was a modified adaptation of the "Parental Sources of Information Questionnaire," which had been employed in a previous, similar study conducted in Jordan [6]. Approval from the original authors was secured prior to incorporating this questionnaire into the present study.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 26 (Released 2019; IBM Corp., Armonk, New York, United States). Categorical sociodemographic data were expressed in terms of frequencies and percentages. Mann-Whitney and Kruskal-Wallis tests were employed to assess the relationship between the outcome numerical variable and sociodemographic factors. These tests provided medians, interquartile ranges, and associated p-values.
Generalized linear regression models were established to ascertain the predictors of high scores in parental awareness and knowledge concerning children's developmental MSs. These models were based on the sociodemographic variables that exhibited statistical significance in relation to the primary outcome. The results of the regression analyses were presented in the form of beta coefficients, along with their corresponding 95% CIs. Statistical significance was determined at a p-value of less than 0.05.
Results
As per Table 1, in our study on parental awareness and knowledge about children's developmental MSs, we examined a diverse sample of 873 participants, predominantly female (77.00%). The data in Table 1 has been represented as N (number of participants) and % (percentage). A p-value of less than 0.05 was considered statistically significant.
Table 1: Sociodemographic data (n = 873)Sociodemographic data (n = 873) representing the number of participants (N) and percentage (%) in the study. Significance level: p<0.05.
The age distribution revealed that a substantial portion of the respondents were below 30 (37.00%). Regarding marital status, the majority were married (72.70%). A significant proportion of the participants identified as Saudi nationals (88.40%). Geographically, the majority resided in the Western region (78.60%). In terms of residency, 80.20% lived in urban areas. Educational levels varied, with a significant proportion holding university degrees (66.70%). Employment status showed diversity, with 45.50% being employed. The monthly income distribution varies, with the highest proportion (45.60%) earning less than 5000.
Based on Table 2, the results of our study on parental awareness of children's developmental MSs revealed significant variation in participants' perceptions of when infants typically reach various developmental stages. The data in Table 2 has been represented as N (number of participants) and % (percentage). A p-value of less than 0.05 was considered statistically significant. For the question regarding when an infant starts to move their head, the majority (33.80%) believed it occurs at one week. When it comes to infants turning over, 76.60% of respondents believed this occurs at six months. In the case of standing, the most common perception was that it begins at 10 months (54.30%). Concerning walking alone steadily, 38.60% believed it happens at 12 months. Climbing stairs was thought to start at 24 months by 44.30% of respondents. The ability to follow things with the eyes was perceived by 59.50% to start at six weeks. Most participants believe a child approaches objects at six months (49.70%). A substantial 77.10% believed this begins at three years and above for manual skills like drawing.
Table 2: Descriptive analysis of parental awareness and knowledge about children's developmental milestone (gross and fine motors) (n = 873)Descriptive analysis of parental awareness and knowledge about children's developmental milestones (gross and fine motors) (n = 873), representing the number of participants (N) and percentage (%) in the study. Significance level: p<0.05.
Respondents reported diverse beliefs about when a child begins to respond to the mother's voice, with 30.50% perceiving this to occur at three weeks. The initiation of saying "Mama and Papa" was thought to commence predominantly at 10 months (36.00%). The MS of smiling was believed to start at six weeks by (54.50%) of participants, while the recognition of age and name was perceived as beginning mostly at two years (31.00%). Saying "bye-bye" was thought to start at one year by 41.40%, and drinking from a cup was perceived as achievable at 18 months by 33.20%. Finally, regarding the control of urination, a significant 48.20% believed it begins at three years (Table 3).
Table 3: Descriptive analysis of parental awareness and knowledge about children's developmental milestone (speech and language, social and emotional) (n = 873)Descriptive analysis of parental awareness and knowledge about children's developmental milestone (speech and language, social and emotional) (n = 873), representing the number of participants (N) and percentage (%) in the study. Significance level: p<0.05.
Most respondents (62.40%) sought information from medical physicians and pediatricians (Figure 1).
Source of information regarding parental awareness and knowledge about children's developmental milestoneThe data has been represented as %.
The overall median and IQR of knowledge score is 6.0 (5.0-7.0). Regarding Table 4, a statistically significant difference (p-value < 0.001) was observed between genders, with females reporting a slightly higher median awareness score (6.0, IQR 5.0-7.0) compared to males (5.0, IQR 4.0-7.0). Age also showed significant differences (p-value < 0.001), where participants aged below 30 and between 31-39 and 40-49 had a median awareness score of 6.0, whereas those aged 50-59 had a median of 6.0 (IQR 4.5-7.0), and those aged 60 or more had a slightly lower median of 5.5 (IQR 3.25-7.0). Marital status significantly impacted (p-value = 0.007) awareness, with divorced individuals reporting a median of 5.0 (IQR 4.0-6.5), while singles, married, and widowed participants had a median score of 6.0. The geographical region demonstrated a significant difference (p-value = 0.044), with the Southern region showing a median awareness score of 5.0 (IQR 3.0-7.0), while other regions had a median of 6.0. However, no significant differences were found based on nationality, residency, educational level, employment status, or monthly income.
Table 4: Association between sociodemographic data and parental awareness and knowledge about children's developmental milestoneDescriptive analysis of knowledge scores with medians (median) and interquartile ranges (IQR), along with p-values for various demographic parameters (n = 873). Significance level: p < 0.05.
In Table 5, the results of our regression analysis examining the impact of various demographic factors on parental awareness of children's developmental MSs revealed several notable findings. Gender had a significant effect, with males showing a lower awareness level compared to females (Beta = -0.582, 95% CI [-0.890, -0.274], p-value < 0.001). Marital status demonstrated significance, where divorced individuals showed a lower awareness level than widowed participants (Beta = -1.641, 95% CI [-2.993, -0.288], p-value = 0.017). At the same time, no significant differences were found for singles or married individuals.
Table 5: Linear regression showing predictors of parental awareness and knowledge about children's developmental milestone based on the statistically significant sociodemographic data Regression analysis results with Beta values, 95% confidence intervals (CI), and p-values for the impact of various demographic factors on parental awareness of children's developmental milestones (n = 873). Significance level: p < 0.05.
Discussion
The current study outlines Western Saudi Arabia's parents' understanding of newborn development stages and childrearing. The well-being of children, parents, and society as a whole depends on parenting expertise and a grasp of childrearing and development processes. As far as we know, Saudi Arabia lacks such information in the Western region.
In contrast, Saudi women demonstrated a greater understanding of the parent-child relationship [6]. As opposed to 25% in the previous study, 42.4% of our study participants reject the notion that carrying a crying infant will spoil him or her [6]. In a similar vein, our study revealed a more positive interpretation of the causes of a baby's crying than the Jordanian one [6], with 51.7% of the moms in our sample disagreeing that babies cry merely to cause problems compared to 29.5% of the mothers in the Jordanian study.
Typically, parents get virtually exclusively physical information from healthcare practitioners, with little to no emphasis placed on cognitive, emotional, and parent-infant interaction skills [11]. Furthermore, it is evident that the primary focus of physical healthcare services is on vaccines, physical examinations, and evaluations of the growth and development of infants. According to earlier research in the literature, pediatricians have a crucial role in parenting practices by focusing on basic treatment and health maintenance while ignoring discussions with them regarding parts of childrearing education [12]. The current investigation revealed a high degree of physical aspect understanding.
Most services provided by PHCs concentrate on immunizations, growth parameter checks, and general health-related concerns like constipation, feeding difficulties, and nutritional challenges. This highlights our population's general lack of maternal information. Because PHC practitioners handle such general health-related themes, the health and safety subscale, which had the greatest level of knowledge (63.4%) among mothers, is an excellent example of such a shortage in the PHC function. Another study conducted by Arabs has likewise made the same observation. Furthermore, fundamental security and physical health subjects like immunization and diet are periodically covered in-depth on various media channels. While most pediatricians address fundamental health maintenance issues, worldwide studies have revealed that other areas of childrearing and development instruction are often disregarded [13,14].
The primary sources of information regarding developmental MSs in the current study were medical education websites, mothers' families, healthcare providers, and the presence of an older kid. The current way information is accessed is expected to change as the internet becomes more widely available [15]. Parents also depend on information from their own families, and studies have shown that mothers' understanding of infant development is closely correlated with that of their own mothers [15]. Contrary to our findings [16], a similar Iraqi study found that mothers learned the majority of knowledge about their children's developmental MSs from their own experiences (71.5%), with very small percentages learning it from doctors (16.5%) and PHC institutions (5.5%).
According to other research of a similar nature, moms who are employed and educated - especially those with a higher degree of education - have a good developmental understanding [15]. The results of the current study indicated a substantial correlation between the mother's work and understanding of the overall development MSs. This went against the findings [16], which showed a strong correlation between homemaker moms' understanding of motor development and their level of education. Regarding parity, the number of delivered kids and the mother's awareness of a child's developmental MSs did not significantly correlate, consistent with a 2015 study that also revealed no significant correlation [17].
Conclusions
A child's early years significantly impact their future social, physical, mental, and cognitive development. Furthermore, as parents are typically in charge of providing childcare at this crucial time in most cultures and groups, their understanding of developmental MSs affects the type and standard of care the kid receives. However, parents have gaps in their knowledge of children's development, even though women are better at identifying MSs than men. The majority of parents lacked appropriate levels of knowledge and were unable to accurately respond to questions about the developmental MSs of their children.
In general, it is believed that Western region Saudi parents only have a limited understanding of certain areas of childrearing - primarily physical safety precautions. It was noted that there was a lack of expertise in other parenting abilities. The lack of emphasis on interactions between mothers and healthcare professionals may be the primary cause of this inadequate knowledge, particularly given that mothers mainly acquired their childrearing knowledge from nurses and physicians. Nurses and doctors are advised to educate and assist families by providing parenting education across all developmental stages of children as a workable solution to such an issue.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maternal knowledge of child development and quality of parenting among White, African‑American and Hispanic mothers J Appl Dev Psychol Huang K O’Brien Caughy M 149170262015
- 2Maternal attitudes and knowledge of child-rearing: associations with family and child outcomes Child Dev Benasich AA Brooks-Gunn J 11861205671996 https://pubmed.ncbi.nlm.nih.gov/8706517/8706517 · pubmed ↗
- 3What do mothers know? Maternal knowledge of child development Infant Ment Health J Reich S 1431562620052868252110.1002/imhj.20038 · doi ↗ · pubmed ↗
- 4Early childhood development and Iranian parents' knowledge: a qualitative study Int J Prev Med Habibi E Sajedi F Afzali HM Hatamizadeh N Shahshahanipour S Glascoe FP 84820172914265010.4103/ijpvm.IJPVM_159_17PMC 5672654 · doi ↗ · pubmed ↗
- 5Assessment of mothers knowledge regarding the developmental milestone among children under two years in Iraq Am J Appl Sci Alkhazrajy LA Aldeen ER 869877142017 https://www.researchgate.net/publication/321394485_Assessment_of_Mothers_Knowledge_Regarding_the_Developmental_Milestone_among_Children_Under_Two_Years_in_Iraq
- 6Jordanian mothers' knowledge of infants' childrearing and developmental milestones Int Nurs Rev. Safadi RR Ahmad M Nassar OS Alashhab SA Abdel Kader R Amre HM 5059632016 https://www.academia.edu/35050680/Jordanian_mothers_knowledge_of_infants_childrearing_and_developmental_milestones 2575692710.1111/inr.12185 · doi ↗ · pubmed ↗
- 7Mothers' knowledge of child health matters: are we doing enough?J Family Community Med Al-Ayed IH 22281720102202266710.4103/1319-1683.68785 PMC 3195075 · doi ↗ · pubmed ↗
- 8Transforming the Workforce for Children Birth Through Age: A Unifying Foundation Allen L Kelly BB Washington (DC), USA National Academies Press 2015 https://pubmed.ncbi.nlm.nih.gov/26269871/26269871 · pubmed ↗