Case report of pulmonary vein isolation in situs inversus totalis
Annina Stauber, Raban Jeger, Omer Dzemali, Andreas Stephan Müller

TL;DR
This case report describes a successful treatment of atrial fibrillation through pulmonary vein isolation in a patient with a rare condition called situs inversus totalis.
Contribution
The novelty lies in demonstrating the successful execution of pulmonary vein isolation in a patient with situs inversus totalis.
Findings
Pulmonary vein isolation was successfully performed in a patient with situs inversus totalis.
The patient showed no recurrence of atrial fibrillation for two years post-procedure.
Abstract
Situs inversus totalis (SIT) is a rare condition, where all the organs in the body are mirrored. Atrial fibrillation occurs in patients with SIT. We describe the case of pulmonary vein isolation (PVI) in SIT. A patient with atrial fibrillation was referred to our hospital due to palpitations. Diagnosis of atrial fibrillation was made by electrocardiogram. The patient reported to have a SIT that was confirmed. Meticulous preparation was done including a three-dimensional model and radiofrequency PVI was performed successfully. No recurrence of atrial fibrillation was detected until last follow-up 2 years after PVI. Pulmonary vein isolation in SIT can be performed successfully and with excellent long-term result.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
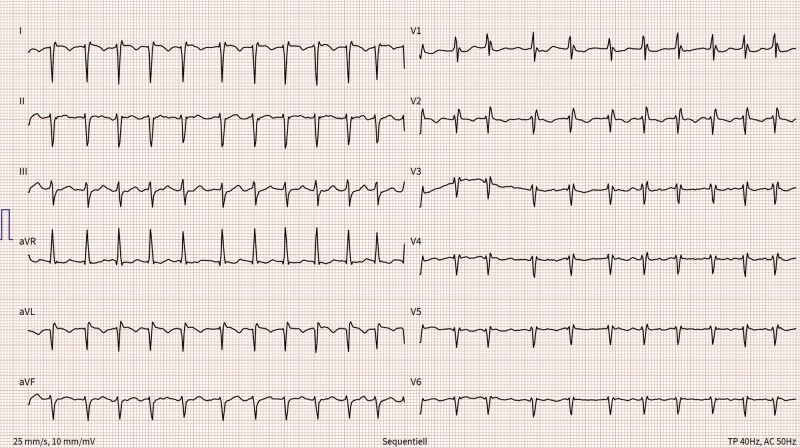 Figure 1
Figure 1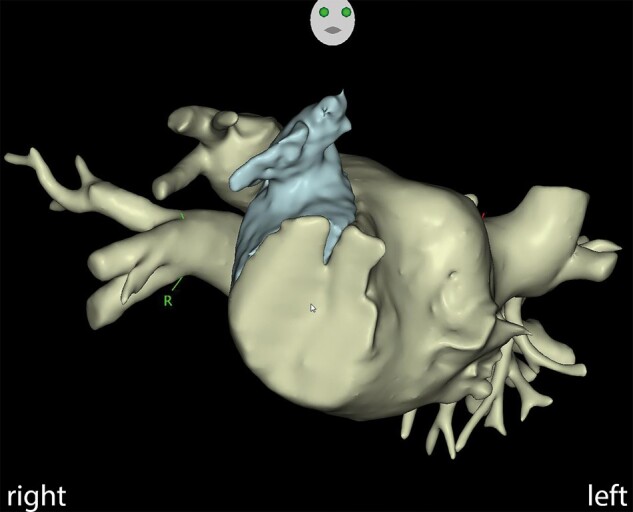 Figure 2
Figure 2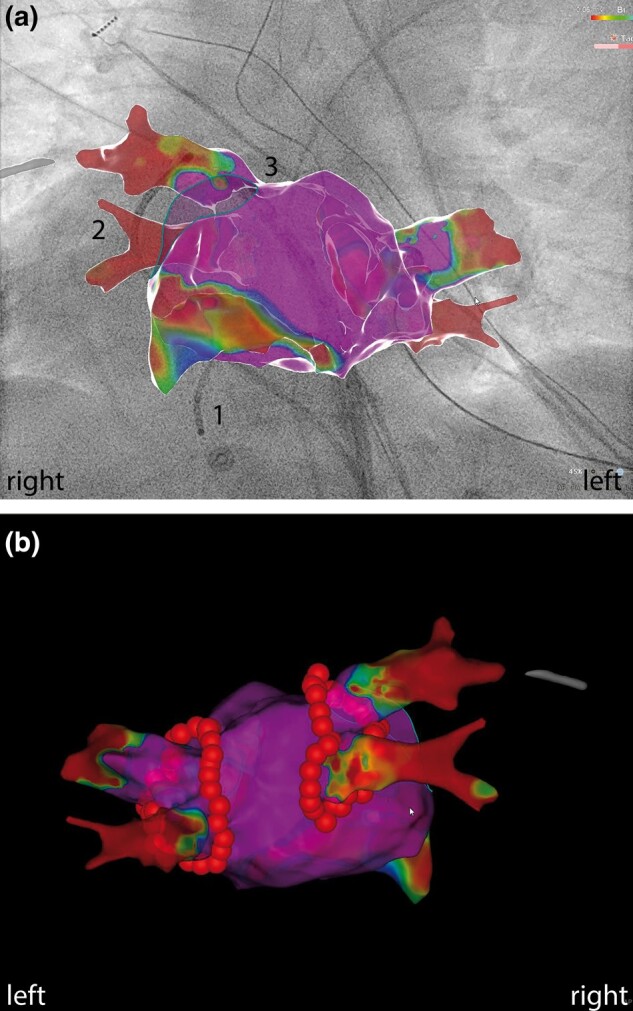 Figure 3
Figure 3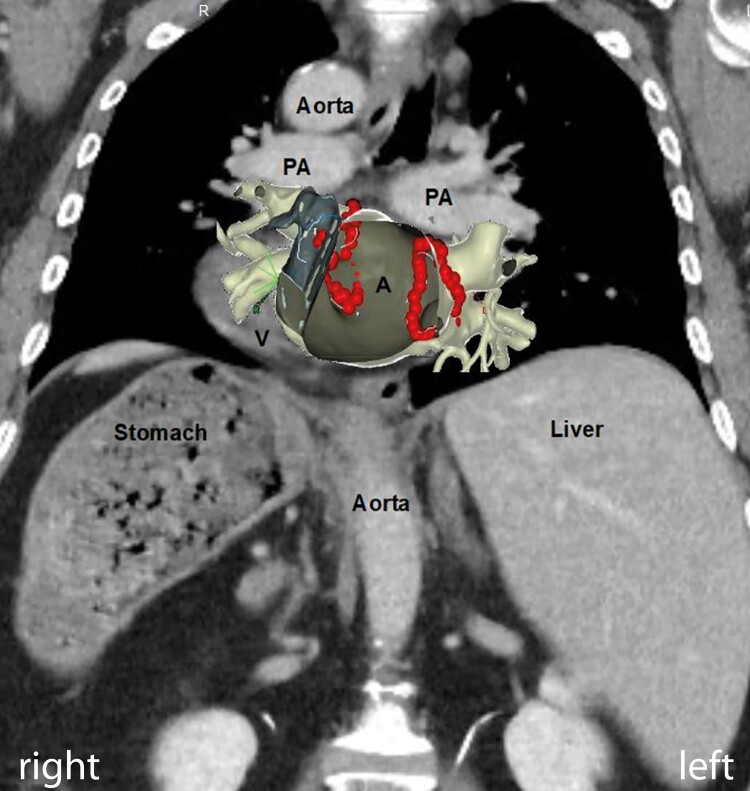 Figure 4
Figure 4| 1999 |
First manifestation of palpitations and chest pain |
| 01/2021 |
Electrocardiogram (ECG) and transthoracic echocardiography confirmed the situs inversus reported by the patient |
| 03/2021 |
Coronary angiography ruled out coronary heart disease |
| 03/2021 |
Computed tomography confirmed diagnosis of situs inversus totalis |
| 03/2021 |
ECG revealed paroxysmal atrial fibrillation |
| 06/2021 |
Pulmonary vein isolation for atrial fibrillation was performed |
| 06/2023 |
Follow-up including long-term ECG demonstrating stable sinus rhythm |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac Valve Diseases and Treatments · Congenital Heart Disease Studies
Introduction
Pulmonary vein isolation (PVI) has become increasingly popular in the last years, and its results have improved with technological advances. However, whether success rates of PVI are similar in patients with atypical anatomy is not known. We describe the case of a patient with situs inversus totalis (SIT) undergoing PVI. In SIT, all the thoracic and abdominal organs are mirrored.
Summary figure
**: **
Case summary
We report the case of a 68-years old, otherwise healthy, female patient being referred to our hospital due to chest pain and palpitations. At the first visit in the outpatient clinic, vital parameters were within normal range and she was cardiopulmonary compensated. Twelve lead electrocardiogram (ECG) showed signs of dextrocardia and transthoracic echocardiography was challenging but supported the diagnosis of situs inversus, which was reported by the patient. The patient was admitted to hospital for coronary angiography, which ruled out coronary heart disease. A computed tomography (CT) was performed, and a complete situs inversus totalis was documented, with the heart and all the other organs mirrored. No cardiac malformation was found. During this hospitalization, symptomatic tachycardic atrial fibrillation was documented on ECG (Figure 1). The existing medication with bisoprolol that was initially started with 2.5 mg for palpitations was increased to 10 mg daily and rivaroxoban 20 mg daily was administered. However, she remained symptomatic. In discussion with the patient and the team, the patient refused to take antiarrhythmic drugs because of the potential side effects and together the decision to perform the PVI was made.
Electrocardiogram in dextrocardia showing atrial fibrillation: right axis deviation with positive QRS complexes in aVR and negative QRS complexes in the lead I and aVL. R waves continuously decrease from V1 to V6.
Preparation before procedure
We studied the mirrored anatomy on CT in detail. The CT was segmented in the CARTOSEG TM® system (Biosense Webster, NJ, USA) (Figure 2). Both improved our understanding of anatomy. However, understanding the anatomy is the basic requirement, but precise control and guidance of the catheters, sheaths, and needles are also essential for the successful performance of a procedure. It seemed that this could be best prepared by a three-dimensional (3D) model and therefore we built one. Every important step of the procedure was performed in this model prior to the procedure using similar materials to those used in the procedure.
3D reconstruction of cardiac CT, showing the systemic atrium and atrial appendage (RAO view).
Ablation procedure
Ablation was performed under general anaesthesia. The ultrasound-assisted venous access was chosen via right groin puncture. A quadripolar catheter was placed into the subpulmonary ventricle, and a decapolar catheter was placed into the coronary sinus. A guide wire was positioned into the superior vena cava, and a non-steerable long sheath (SL0, Abbott, St. Paul, MN, USA) was placed over the wire into the superior vena cava. The wire was exchanged with a Brockenbrough™ needle (BRK-1, Abbott, St. Paul, MN, USA). The sheath-needle system was retracted at an 8 o’clock position until the second ‘jump’. The position of the needle in the septum was checked with an X-ray [right anterior oblique (RAO) 47° and left anterior oblique (LAO) 39°] and transoesophageal echocardiography (TEE, view rotation 83°). Transseptal puncture (TSP) was performed on the first attempt without complication (see Supplementary material online, Videos S1 and S2). The guide wire was advanced to the lateral superior pulmonary vein above the atrial appendage. The non-steerable sheath was exchanged with a steerable sheath (Agilis, Abbott, St. Paul, MN, USA). The non-steerable sheath was placed in the subpulmonary atrium via a second guide wire. Next, the ablation catheter was introduced into the systemic atrium in a two-over-one method. A PentaRay®NAV catheter (Biosense Webster, NJ, USA) was introduced via the steerable sheath into the systemic atrium. The 3D map was acquired with the PentaRay®NAV catheter (Biosense Webster, NJ, USA). The voltage map showed normal voltage myocardium (Figure 3A). The sheath-catheter combination was changed for ablation, and ablation was performed with the THERMOCOOL SMARTTOUCH® SF Catheter (Biosense Webster, NJ, USA) in the steerable sheath (Agilis, Abbott, St. Paul, MN, USA). The wide antral cirumferential ablation was performed with 30 W at the posterior wall and 40 W at the anterior wall (target ablation index 400 posterior, 550 anterior). First pass isolation was achieved on both sides, confirmed by entrance and exit block (Figures 3B and 4). Procedure time was 132 min, fluoroscopy time 7.9 min, X-ray dose (dose area product) 83.4 cGy cm^2^, and total ablation time 31 min.
(A) CARTO 3D voltage map with normal myocardium, (1) catheter in subpulmonary ventricular apex, (2) coronary sinus catheter, (3) ablation catheter (AP view). (B) CARTO 3D map, successful ablation with ablation points (PA view).
CT with overlaying Carto geometry. A, atrium; V, ventricle; PA, pulmonary artery.
Follow-up
No atrial fibrillation symptoms were reported until the most recent control 2 years after the procedure. After six weeks, a 48 h long-term ECG and after six months and 2 years a 72 h long-term ECG were performed and none of them showed atrial fibrillation recurrence.
Discussion
Electrocardiogram
SIT is a rare condition and sometimes this condition can remain undetected for decades. A first hint for SIT can be found on ECG due to the dextrocardia.^1^ Electrocardiogram in dextrocardia shows a right axis deviation, positive P and QRS in lead aVR, and negative P and QRS in lead I and aVL, and R waves are continuously decreasing from V1 to V6. If the leads are positioned mirrored, the ECG changes can be unmasked. An important differential diagnosis is the dextroposition of the heart, where the heart is shifted to the right side but not mirrored (e.g. in case of right-sided pneumothorax). In that case, ECG cannot be reversed by positioning the leads mirrored.
Pulmonary vein isolation in situs inversus totalis
PVI is one of the standard procedures in electrophysiology. In special anatomical situations such as SIT, challenges can be mastered by meticulous preparation. In this case, CT helped to understand detailed anatomy. CT and transthoracic echocardiogram were able to exclude additional congenital heart disease, which are more prevalent in SIT.^2^ We created a 3D model prior to the procedure, whereby the mirrored anatomy was studied and understood in detail. We considered performing the procedure from the left-sided groin and mirroring the X-ray projections, but this idea was discarded given the additional unfamiliarity.
TSP turned out to be the most crucial step of the procedure. The needle-sheath system for TSP was held in an 8 o’clock position as described in literature, mirroring the 4 o’clock position in patients without SIT.^3^ It was guided by X-ray as usually done at our centre and additionally TEE. Good preparation with deep insertion of a coronary sinus catheter into the distal coronary sinus helped to visualize the anatomy of the atrioventricular groove radiologically and to guide transseptal access. We found that TEE contributed to additional safety in this specific case, because the correct position in X-ray could be confirmed by a second image modality. Transoesophageal echocardiography rotation in our case was 83°, somehow mirroring the standard 135°. Intracardiac echocardiography (ICE) could have been another modality to use, but our experience with ICE guided TSP is limited. For mapping and ablation the same catheters and sheets as we usually use for routine PVIs were used. Also here, movements had to be performed mirrored and every movement had to be considered carefully beforehand. 3D model was very useful to learn these mirrored movements.
Screening the literature about PVI in SIT, minimal experience is found because SIT is a rare condition (∼1:10 000).^2^ Due to its rare nature and lack of evidence, there is no specific advice how to treat patients with atrial fibrillation and SIT in the ESC guidelines.^4^ To the best of our knowledge, no severe complication in PVI in SIT is documented in literature. It is essential to assess the risk–benefit individually for every patient since a long procedure duration or high radiation times and doses were found in some reports.^5–8^ In our case, the long-term result was excellent, no complication occurred and the procedural data (X-ray time, X-ray dose, procedure time, ablation time) were similar to patients with normal anatomy.^9–11^
Conclusion
To conclude, PVI in SIT is feasible and can be performed successfully without complication, with excellent long-term result and with procedural data comparable to PVI with normal anatomy. However, meticulous preparation is crucial.
Supplementary Material
ytae067_Supplementary_DataClick here for additional data file.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Golzarian H, Widmer MB, Mughal S, Patel SM. ECG challenge: beating at the right place at the right time. Eur Heart J Case Rep 2023;7:ytad 094.10.1093/ehjcr/ytad 094PMC 999104336895296 · doi ↗ · pubmed ↗
- 2Eitler K, Bibok A, Telkes G. Situs inversus totalis: a clinical review. Int J Gen Med 2022;15:2437–2449.35264880 10.2147/IJGM.S 295444 PMC 8901252 · doi ↗ · pubmed ↗
- 3Zhao X, Su X, Long DY, Sang CH, Bai R, Tang RB, et al Catheter ablation of atrial fibrillation in situs inversus dextrocardia: challenge, improved procedure, outcomes, and literature review. Pacing Clin Electrophysiol 2021;44:293–305.33372281 10.1111/pace.14144 · doi ↗ · pubmed ↗
- 4Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–49 · doi ↗ · pubmed ↗
- 5Del Greco M, Marini M, Centonze M, Disertori M. Atrial fibrillation ablation procedure using electroanatomic reconstruction of the right and left atrium in a patient affected by dextrocardia. Europace 2009;11:1399–1400.19654126 10.1093/europace/eup 209 · doi ↗ · pubmed ↗
- 6Xue ZM, Sang CH, Dong JZ, Ma CS. Catheter ablation of persistent atrial fibrillation in a patient with dextrocardia. Chin Med J (Engl) 2012;125:1839–1840.22800910 · pubmed ↗
- 7Chong E, Chang SL, Chen SA. Pulmonary vein isolation in a patient with dextrocardia. Europace 2012;14:1725.23002200 10.1093/europace/eus 325 · doi ↗ · pubmed ↗
- 8Okajima K, Nakanishi T, Ichibori H, Shirai T, Kadotani M, Shimizu H, et al Trans-aortic pulmonary vein isolation using magnetic navigation system for paroxysmal atrial fibrillation in a patient with dextrocardia, situs inversus, and inferior vena cava continuity with azygos vein. J Arrhythm 2018;34:583–585.30327707 10.1002/joa 3.12096 PMC 6174455 · doi ↗ · pubmed ↗