Disseminated Superficial Porokeratosis: A Case Report
Aysha Taha, Ghadah Khormi, Laila Alali, Afnan Maashi, Ahlam Alharbi

TL;DR
This case report describes a rare skin condition called disseminated superficial porokeratosis in a 45-year-old woman, highlighting its diagnosis, treatment, and the importance of long-term care.
Contribution
The paper presents a detailed case of disseminated superficial porokeratosis with multimodal treatment and emphasizes diagnostic and management insights.
Findings
Histopathological confirmation of coronoid lamellae confirmed the diagnosis.
Multimodal treatment including topical and systemic therapies led to satisfactory clinical outcomes.
Long-term follow-up and patient education are crucial for managing the condition and improving quality of life.
Abstract
Disseminated superficial porokeratosis is a rare dermatological disorder characterized by annular keratotic lesions, presenting diagnostic challenges due to its variable clinical manifestations. The pathogenesis involves genetic predisposition and environmental factors, with mutations in the mevalonate pathway implicated. Despite its benign nature, this condition significantly impacts patients' quality of life, necessitating accurate diagnosis and effective therapeutic strategies. We present the case of a 45-year-old female with a three-year history of annular plaques on sun-exposed areas progressing to involve multiple body regions. The characteristic histopathological finding of coronoid lamellae confirmed the diagnosis of disseminated superficial porokeratosis. Treatment involved a multimodal approach, including topical corticosteroids, calcineurin inhibitors, and systemic retinoids,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2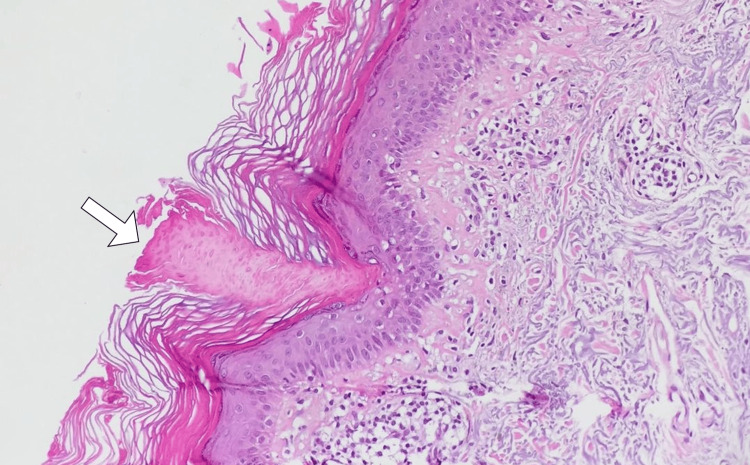 Figure 3
Figure 3| Lab Test | Result | Reference Range |
| Hemoglobin | 12.5 g/dL | 12.0 - 15.5 g/dL |
| White Blood Cell Count | 7,200 cells/mm³ | 4,000 - 11,000 cells/mm³ |
| Platelet Count | 250,000 cells/mm³ | 150,000 - 450,000 cells/mm³ |
| Aspartate Aminotransferase | 25 U/L | 10 - 40 U/L |
| Alanine Aminotransferase | 30 U/L | 7 - 56 U/L |
| Alkaline Phosphatase | 75 U/L | 44 - 147 U/L |
| Total Bilirubin | 0.8 mg/dL | 0.2 - 1.2 mg/dL |
| Blood Urea Nitrogen | 18 mg/dL | 7 - 20 mg/dL |
| Creatinine | 0.9 mg/dL | 0.6 - 1.3 mg/dL |
| Glucose | 90 mg/dL | 70 - 100 mg/dL |
| Sodium | 138 mEq/L | 135 - 145 mEq/L |
| Potassium | 4.2 mEq/L | 3.5 - 5.1 mEq/L |
| Bicarbonate | 26 mmol/L | 23 - 29 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and rare skin diseases. · Cancer and Skin Lesions · Dermatologic Treatments and Research
Introduction
Disseminated superficial porokeratosis is a rare and distinctive dermatological disorder characterized by the development of multiple, annular keratotic lesions with a central atrophic core [1]. First described by Mibelli in 1893, disseminated superficial porokeratosis remains a challenging condition due to its diverse clinical manifestations and the potential for misdiagnosis [1]. The pathogenesis of disseminated superficial porokeratosis is multifactorial, involving genetic predisposition and environmental factors. Alterations in the mevalonate pathway and impaired immune regulation contribute to its development. While typically benign, disseminated superficial porokeratosis can significantly impact patients' quality of life, prompting the need for accurate diagnosis and tailored management strategies [1,2].
This case report presents a comprehensive analysis of a 45-year-old female with disseminated superficial porokeratosis, emphasizing the intricate diagnostic process, therapeutic interventions, and clinical outcomes. The report underscores the importance of a meticulous clinical approach and highlights the challenges in managing this rare porokeratotic disorder.
Case presentation
A 45-year-old female presented to our dermatology clinic with a chief complaint of persistent skin lesions. The patient reported a gradual onset of asymptomatic, small, annular plaques with a characteristic raised border and atrophic center over the past three years. She noted the lesions initially appeared on sun-exposed areas, such as the forearms and face, but later involved the trunk and lower extremities. The patient's medical history revealed no significant comorbidities or relevant family history of dermatological conditions.
Upon detailed questioning, the patient reported a lack of response to over-the-counter topical treatments, including corticosteroids and emollients. She denied any systemic symptoms, such as fever, weight loss, or joint pain. Social history was unremarkable, with no history of excessive sun exposure or relevant occupational exposures.
Physical examination revealed multiple, well-defined, annular plaques with a raised border and central atrophy distributed symmetrically on the face, neck, upper chest, back, forearms, and lower extremities. The lesions exhibited a characteristic coronoid lamella at the periphery, suggestive of disseminated superficial porokeratosis (Figures 1-2). The differential diagnosis considered at this stage included other forms of porokeratosis, such as linear porokeratosis and punctate porokeratosis, as well as conditions presenting with annular lesions, such as tinea corporis and granuloma annulare.
Clinical image of the lower extremity depicting characteristic annular plaques with a raised border and central atrophy, representative of porokeratosis
Dermatoscopic image revealing distinctive features of porokeratosis, including a coronoid lamella, supporting the clinical diagnosis of porokeratosis
Laboratory investigations, including complete blood count, liver and renal function tests, and metabolic panel, were within normal limits (Table 1). An initial skin biopsy was performed on a representative lesion, confirming the clinical suspicion of disseminated superficial porokeratosis by revealing the characteristic coronoid lamella in the epidermis (Figure 3).
Histopathological micrograph of a skin biopsy, highlighting the presence of a coronoid lamella (arrow) confirming the diagnosis of porokeratosis
The final diagnosis of disseminated superficial porokeratosis was established based on the characteristic clinical features, supported by histopathological findings. Management involved a combination of topical therapies, including corticosteroids and calcineurin inhibitors, as well as systemic retinoids to target the underlying pathogenic process.
The hospital course was uneventful, with the patient showing gradual improvement in lesion size and morphology. Regular follow-up appointments were scheduled to monitor treatment response, assess for adverse effects, and provide ongoing patient education regarding sun protection measures.
Discussion
The presented case of disseminated superficial porokeratosis offers valuable insights into the clinical and therapeutic challenges associated with this rare dermatological disorder. Diagnostic challenges in disseminated superficial porokeratosis are well-recognized due to the condition's variable presentation and potential mimicry of other dermatoses. The characteristic histopathological finding of a coronoid lamella is crucial for definitive diagnosis [3,4]. In this case, the initial presentation on sun-exposed areas and subsequent involvement of other body regions underscore the importance of considering disseminated superficial porokeratosis in the differential diagnosis of annular lesions. The correlation between clinical features and histopathology remains pivotal for accurate identification, especially when distinguishing disseminated superficial porokeratosis from other forms of porokeratosis [1-3].
The multifactorial etiology of disseminated superficial porokeratosis involves a complex interplay of genetic predisposition and environmental triggers. Recent advancements in molecular genetics have identified mutations in the mevalonate pathway as potential contributors to the development of porokeratotic lesions [1,4]. However, further research is warranted to elucidate the precise mechanisms underlying disease pathogenesis. Investigating the genetic landscape of disseminated superficial porokeratosis may unveil potential therapeutic targets, paving the way for more targeted and effective treatment strategies [3-5].
Management of disseminated superficial porokeratosis remains challenging, with limited consensus on the optimal therapeutic approach [1]. Our case highlights the use of a combination of topical corticosteroids, calcineurin inhibitors, and systemic retinoids to achieve satisfactory clinical outcomes. This approach aligns with existing literature suggesting that a multimodal treatment strategy may be necessary for comprehensive disease control. Nonetheless, the need for long-term follow-up and the potential for disease recurrence necessitate ongoing research to refine treatment protocols and enhance patient outcomes [1,2].
Conclusions
In conclusion, the presented case of disseminated superficial porokeratosis sheds light on the intricate clinical course and therapeutic challenges associated with this rare dermatological disorder. The multimodal treatment approach, incorporating topical corticosteroids, calcineurin inhibitors, and systemic retinoids, demonstrated satisfactory outcomes, emphasizing the importance of a comprehensive strategy in managing this condition. The diagnostic journey, marked by characteristic histopathological findings and distinctive clinical features, underscores the need for a meticulous approach to distinguishing porokeratosis from other dermatoses. The case contributes to the evolving understanding of disseminated superficial porokeratosis, emphasizing the importance of continued research to refine diagnostic criteria and optimize therapeutic interventions. As an enigmatic entity, disseminated superficial porokeratosis warrants further exploration, and this case offers valuable insights that may guide future clinical decisions and research endeavors in the field of dermatology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Porokeratoses-a comprehensive review on the genetics and metabolomics, imaging methods and management of common clinical variants Metabolites Pietkiewicz P Korecka K Salwowska N 11761320233813285710.3390/metabo 13121176 PMC 10744643 · doi ↗ · pubmed ↗
- 2A case of disseminated superficial actinic porokeratosis successfully treated with topical lovastatin/cholesterol gel Cureus Sultan Q Massey B Cotter DG 015202310.7759/cureus.40582 PMC 1035247037469822 · doi ↗ · pubmed ↗
- 3Disseminated superficial actinic porokeratosis following hydroxyurea treatment: a case report Australas J Dermatol Romagnuolo M Riva D Alberti Violetti S Di Benedetto A Barberi F Moltrasio C 0564202310.1111/ajd.1394336320094 · doi ↗ · pubmed ↗
- 4A rare case of disseminated superficial porokeratosis-case report J Family Med Prim Care Ramakrishnan R Vignesh TA Durai PC Narasimhan M 119511971120223549580810.4103/jfmpc.jfmpc_1232_21PMC 9051733 · doi ↗ · pubmed ↗
- 5A case of inflammatory disseminated superficial porokeratosis in a colon cancer patient Ann Dermatol Choi KH Kim TY 1501532120092052377410.5021/ad.2009.21.2.150PMC 2861214 · doi ↗ · pubmed ↗