Uncommon Haematological Transformation: Chronic Myeloid Leukaemia Transitioning Into Plasma Cell Leukaemia in a Single Patient
Mili A Jain, Sourya Acharya, Aryan S Pal, Lalit Raut

TL;DR
A patient with chronic myeloid leukaemia developed plasma cell leukaemia, highlighting a rare disease transformation.
Contribution
This case study reports a rare transformation from CML to PCL and suggests a possible role of tyrosine kinase inhibitors in triggering it.
Findings
A patient with CML transitioned to plasma cell leukaemia after two years of imatinib treatment.
The transformation was confirmed through haematological tests and peripheral smear analysis.
The case suggests a possible link between tyrosine kinase inhibitors and disease transformation.
Abstract
A 40-year-old male patient who was a known case of chronic myeloid leukaemia (CML) was diagnosed two years back on tab imatinib 400 mg/day; he came with complaints of easy fatigability, syncopal attacks, and bone pain associated with low-grade fever for 15 days. Repeat haematological profile and a peripheral smear of the patient suggested features of plasma cell leukaemia (PCL)/plasma cell dyscrasia (PCD). A definitive treatment protocol of lenalidomide, bortezomib, and dexamethasone for PCL was prescribed to the patient. This medical case study emphasizes the rare possibility of the transformation of CML into PCL and the possible trigger of tyrosine kinase inhibitor for the same.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
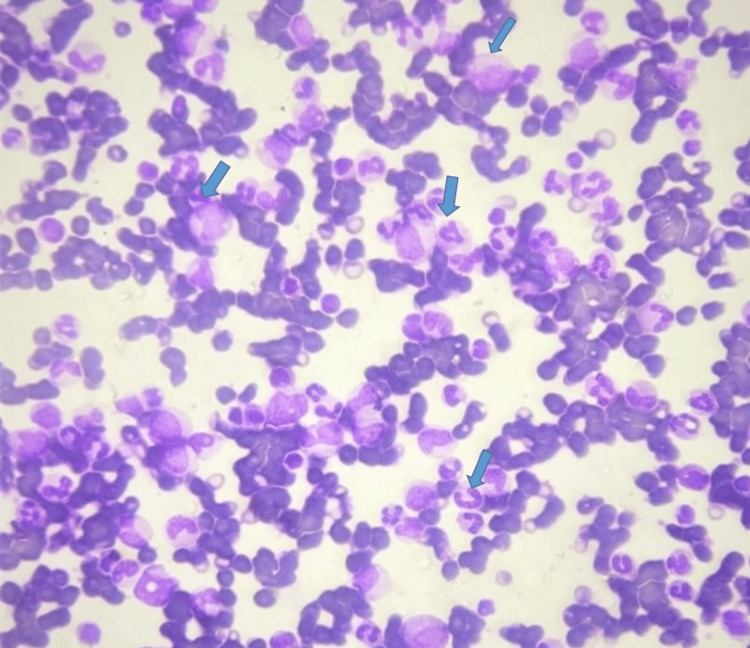 Figure 1
Figure 1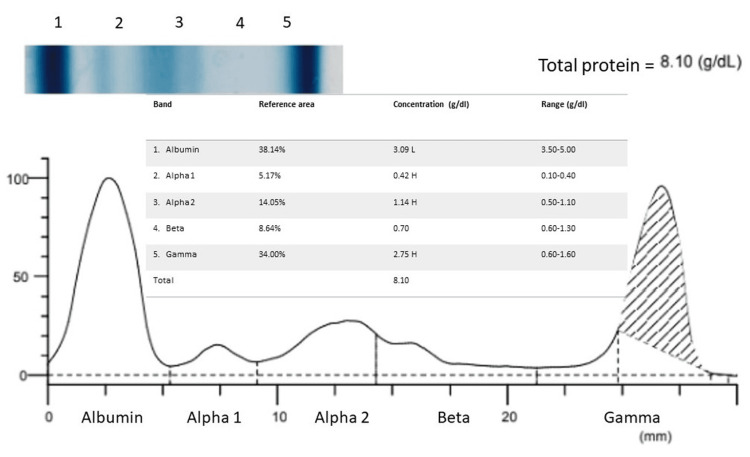 Figure 2
Figure 2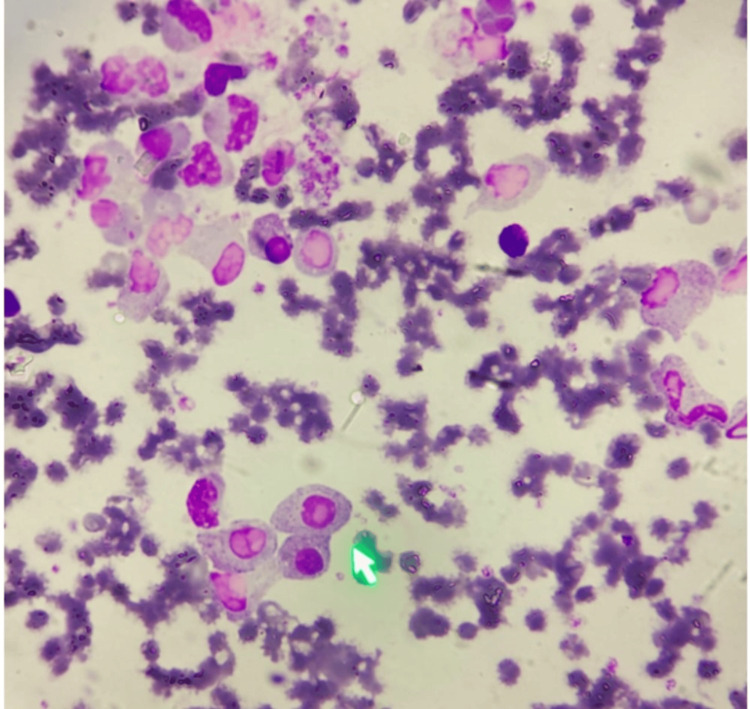 Figure 3
Figure 3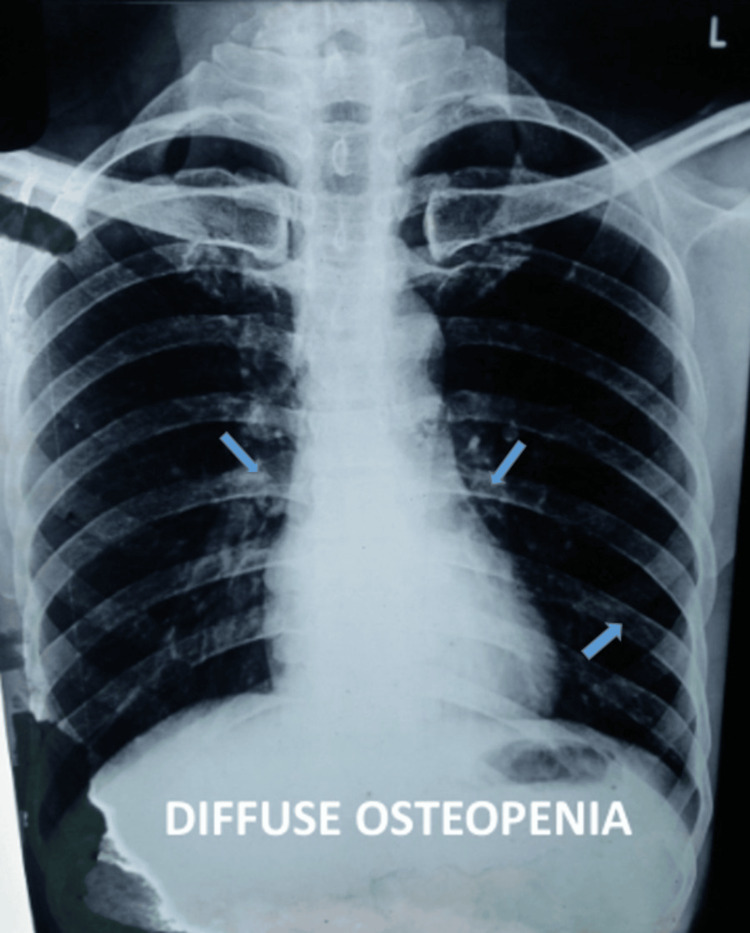 Figure 4
Figure 4| Parameters | Result |
| Haemoglobin | 9.7 g/dl |
| Red blood cells | 3.4 million/mm3 |
| Haematocrit | 28.2% |
| RDW | 17.5% |
| White blood cells | 99,900/mm3 |
| Absolute neutrophil count | 71,000/mm3 |
| Eosinophil count | 2880/mm3 |
| Basophil count | 20,390/mm3 |
| Monocyte count | 230/mm3 |
| MID# | 23,500/mm3 |
| Absolute lymphocyte count | 5,400/mm3 |
| Platelet count | 1,69,000/mm3 |
| Cellularity | Hypercellular |
| Erythroid series | Normoblastic maturation seen |
| Myeloid series | Marked granulocytic hyperplasia with majorly compromising of myelocytes, metamyelocytes, and neutrophils |
| Myeloid/erythroid (M:E) ratio | 8:1 |
| Plasma cells | 1% with normal morphology |
| Differential count: blasts | 4% |
| Promyelocytes | 3% |
| Myelocytes | 19% |
| Metamyelocytes | 12% |
| Neutrophils | 55% |
| Lymphocytes | 7% |
| Eosinophils | 6% |
| Basophils | 3% |
| Parameters | Result |
| Haemoglobin | 11.3 g/dl |
| Red blood cells | 4.24 million/mm3 |
| Haematocrit | 35% |
| RDW | 16.3% |
| White blood cells | 7,400/mm3 |
| Absolute neutrophil count | 5,500/mm3 |
| Eosinophil count | 296/mm3 |
| Basophil count | 45/mm3 |
| Monocyte count | 359/mm3 |
| MID# | 700/mm3 |
| Absolute lymphocyte count | 1,200/mm3 |
| Platelet count | 3,71,000/mm3 |
| Parameters | Result |
| Haemoglobin | 8.3 g/dl |
| Red blood cells | 3.27 million/mm3 |
| Haematocrit | 25.1% |
| RDW | 17% |
| MCV | 76.9 fL |
| White blood cells | 76,320/mm3 |
| Platelet count | 3,02,000/mm3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Chronic Myeloid Leukemia Treatments · Chronic Lymphocytic Leukemia Research
Introduction
Chronic myeloid leukaemia (CML) is a myeloproliferative disorder which is characterised by the presence of Philadelphia (Ph) chromosome [1-3]. The Ph chromosome results from a translocation between the long arm of chromosome 22 and chromosome 9 [1,3]. This results in the breakpoint cluster region protein-Abelson murine leukemia viral oncogene homolog (BCR-ABL) fusion gene, which codes for a protein with abnormal tyrosine kinase activity; this plays a crucial role in determining cellular proliferation, differentiation, and survival [3]. Plasma cell dyscrasia (PCD) is a spectrum of disorders which include monoclonal gammopathies of undetermined significance (MGUS), multiple myeloma, primary amyloidosis, cryoglobulinemia, etc. [2,4]. Plasma cell leukaemia (PCL) is subcategorised within multiple myeloma, a distinctive feature being having more than 20% plasma cells in the peripheral blood [4,5]. Presenting features vary depending on the variant, primary or secondary form. Secondary varieties are the haematological transition of multiple myeloma instances, while the primary form does not show any evidence of multiple myeloma [2,5]. PCL is an aggressive form of tumour and is rarely found in the general population, and evidence also shows that tyrosine kinase inhibitors (TKI) which are the cornerstone drugs used to treat CML may induce the transformation of CML into monoclonal gammopathy [1]. This case report discusses the haematological metamorphosis happening in an individual from CML to PCL.
Case presentation
A 40-year-old male patient had presented two years back with complaints of low-grade fever, generalized weakness, and early satiety of three-month duration. The fever was not relieved on medication, and no diurnal variation was present. On general examination, pallor was evident in the lower palpebral conjunctiva. Abdominal examination revealed massive splenomegaly, extending up to the umbilicus and non-tender on palpation with smooth edges. Mild hepatomegaly extending 2 cm below the costal margin and non-tender with a smooth surface was palpable. No other significant clinical findings were appreciated on examination.
Investigations
Haematological parameters, peripheral smear, and bone marrow aspiration suggested CML. The haematological picture revealed the following findings (Table 1).
Peripheral smear testing demonstrated the following findings (Figure 1).
Abundance of immature granulocytes, neutrophils, basophils, and eosinophils (blue arrow) in CML-CP in a Leishman's-stained peripheral smear under 100x magnification.CML-CP: chronic stable phase of chronic myeloid leukaemia
Bone marrow aspiration assessment suggested the diagnosis of chronic stable phase of chronic myeloid leukaemia (CML-CP) (Table 2).
Serum protein electrophoresis (SPEP) depicted the following findings (Figure 2).
SPEP showed the following findings.SPEP: serum protein electrophoresis
The BCR-ABL study was positive, confirming the diagnosis. The Sokal score was 1.02 which suggested intermediate relative risk. The patient was started on standard imatinib mesylate therapy 400 mg once a day to be taken orally daily and was asked to follow up every three months for one year and then six monthly for one year. The patient came for a follow-up after six months. He was asymptomatic. On examination, the spleen and liver were not palpable. Haematological investigations were repeated, which showed the following picture (Table 3). The patient was not willing to do BCR-ABL quantitative polymerase chain reaction (PCR) studies. Imatinib 400 mg once a day was continued.
Further, the patient did not come for follow-up for more than a year as the presenting symptoms subsided. After two years, the patient presented again with complaints of easy fatigability for one month and bone pain which was associated with low-grade fever for 15 days. The patient also gave a history of two to three episodes of syncopal attacks lasting for a few seconds. On general examination, pallor was observed in the lower palpebral conjunctiva and the tip of the tongue. Abdominal examination revealed mild splenomegaly on deep palpation. A haematological assay of the patient was done (Table 4).
Peripheral smear testing demonstrated the following finding (Figure 3).
Increased number of plasma cells (more than 20%) (green arrow) in a Leishman's-stained peripheral smear under 100x magnification.
X-ray of the chest was advised as a part of the workup, which displayed diffuse osteopenia (Figure 4).
PA view of chest X-ray displaying areas of diffuse osteopenia (blue arrow).PA: posteroanterior
After careful correlation between all the clinical findings and investigations, a provisional diagnosis of CML progressing into PCL was made. The patient was advised lenalidomide, bortezomib, and dexamethasone therapy for the newly diagnosed PCL. Also, imatinib mesylate was stopped, and dasatinib 100 mg once daily was started. Detailed counselling was advised. The patient was recommended a follow-up of three monthly for six months and six monthly for one year consequently.
Discussion
CML is a hematopoietic disorder in which a multipotent stem cell acquires an abnormal BCR-ABL fusion gene, which is famously known as the Ph chromosome [1,3,6]. The chromosome comes into existence by a balanced reciprocal translocation between the long arms of chromosomes 9 and 22 (t 9;22) [1,7]. The shortened chromosome 22 is known as the Ph chromosome. This fusion gene has infrequently been identified in essential thrombocytosis, multiple myeloma, and myelodysplastic syndromes [7]. The existence of CML and PCL in a single person is not well understood. Various hypotheses have been put forward, such as since CML arises from a pluripotent stem cell, it may be possible that CML can transform into malignant cells [1,8,9]. This may be detected by next-generation sequencing techniques, fluorescence in situ hybridisation (FISH) analysis, and PCR [3,7].
Another hypothesis indicates that the secondary malignancies developing in a patient with CML may be related to TKI treatment [3]. A study in 2002 conducted by Gunnarsson et al. [1,9] revealed that secondary malignancies such as gastrointestinal tract cancer, breast cancer, prostate cancer, and throat cancer may have been developed due to TKI therapy. It is unclear from the studies that the cause of the development of secondary malignancies is TKI [1,8,10]. However, the TKI and the pathogenesis of CML in combination may play a crucial role in the transformation of CML into PCL [1].
Conclusions
Synergistic co-occurrence of CML and plasma cell disorder in a single patient is extremely rare in haematological practice. This patient highlights transition from CML to PCL. We presume that TKI and other cytogenetic changes led to this progression. Another potential factor may be the initial gene translocation trigger that led to chronic sustained clonal proliferation. Larger studies into this rare entity may lead to better understanding of the disease process.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: a case report World J Clin Cases Zhang N Jiang TD Yi SH 469847031020223566306310.12998/wjcc.v 10.i 14.4698 PMC 9125270 · doi ↗ · pubmed ↗
- 2How I treat elderly patients with plasma cell dyscrasias Aging (Albany NY) Gavriatopoulou M Fotiou D Ntanasis-Stathopoulos I Kastritis E Terpos E Dimopoulos MA 424842681020183056802910.18632/aging.101707 PMC 6326666 · doi ↗ · pubmed ↗
- 3s VCAM-1, and TGFβ1 in chronic phase, chronic myeloid leukemia patients treated with tyrosine kinase inhibitors Egypt J Immunol Abdel Hammed MR Ahmed YA Adam EN Bakry R Elnaggar MG 163173292022 https://pubmed.ncbi.nlm.nih.gov/36208045/36208045 · pubmed ↗
- 4Plasma cell leukemia: a review of the molecular classification, diagnosis, and evidenced-based treatment Leuk Res Gowin K Skerget S Keats JJ Mikhael J Cowan AJ 10668711120213442532510.1016/j.leukres.2021.106687 · doi ↗ · pubmed ↗
- 5A clinical perspective on plasma cell leukemia; current status and future directions Blood Cancer J Tuazon SA Holmberg LA Nadeem O Richardson PG 231120213356390610.1038/s 41408-021-00414-6PMC 7873074 · doi ↗ · pubmed ↗
- 6The distribution of the Philadelphia chromosome in patients with chronic myelogenous leukemia Blood Whang J Frei E 3rd Tjio JH Carbone PP Brecher G 664673221963 https://pubmed.ncbi.nlm.nih.gov/14084628/14084628 · pubmed ↗
- 7An unprecedented case of p 190 BCR-ABL chronic myeloid leukemia diagnosed during treatment for multiple myeloma: a case report and review of the literature Case Rep Hematol Miki K Obara N Makishima K 7863943201820183040592210.1155/2018/7863943 PMC 6199862 · doi ↗ · pubmed ↗
- 8Multiple myeloma superimposed on chronic myelocytic leukemia Can Med Assoc J Derghazarian C Whittemore NB 104710501101974 https://pubmed.ncbi.nlm.nih.gov/4522851/4522851 PMC 1947744 · pubmed ↗