An unexpected ECG finding
Mathijs Kuiper, Albert Willems, Arthur A.M. Wilde

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
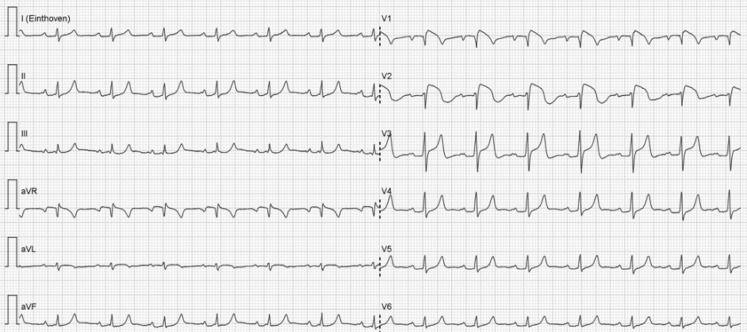 Figure 1
Figure 1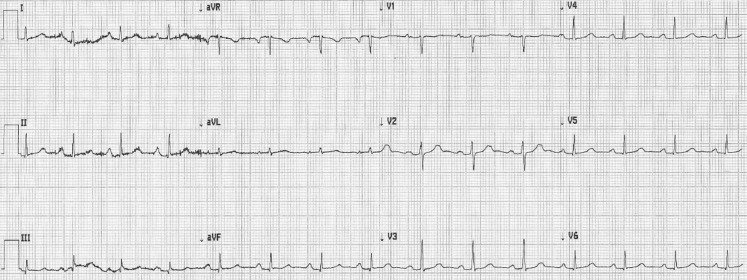 Figure 2
Figure 2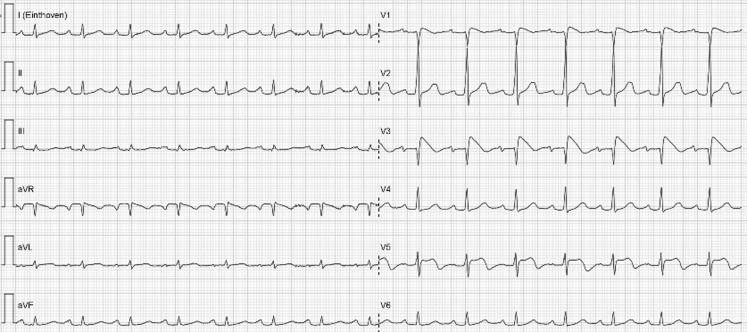 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHuman-Animal Interaction Studies
Answer
The ECG in Fig. 1 shows a sinus rhythm of 90 bpm with an intermediate axis, PQ delay of 202 ms and a narrow QRS complex. Convex ST elevation is seen in the right precordial leads. The ECG could be considered suspicious for acute septal myocardial infarction. However, reciprocal ST-segment changes are lacking and the QRS complex does not show any suspect abnormalities either. The ECG also has aspects of hyperkalaemia; in particular the sharp high voltage T waves point in that direction. The ECG in Fig. 1 is also compatible with a type 1 Brugada pattern. The patient has never had any cardiac symptoms, nor a family history of acute cardiac death.Fig. 1ECG at presentation
The patient was admitted to the intensive care unit for rhythm monitoring. Hyperkalaemia was based on the use of high-dose spironolactone, in combination with dehydration and accordingly matched the patient’s comorbidity. Figure 2 shows the ECG taken after correction of the hyperkalaemia (5.2 mmol/l). This ECG returned to normal in a period of 4 h, without ST elevation and no signs of Brugada. Considering this short period of time to normalisation, there is a strong possibility that high potassium levels are provoking this Brugada pattern, as has been described before [1, 2]. Subsequently, Brugada syndrome was confirmed by positive ajmaline provocation testing. Shortly after administration of ajmaline the exact same type of Brugada was reproduced (with alternative placement of leads V3 and V5 to the intercostal space above V1 and V2, respectively; Fig. 3). This drug-induced Brugada syndrome is considered to be a type with a low risk of acute cardiac death [3]. However, in general it is recommended to prevent fever and if fever occurs to perform an ECG for potential rhythm monitoring, and to avoid certain drugs with the potential to prolong the QT interval.Fig. 2ECG after correction of hyperkalaemia Fig. 3ECG during ajmaline provocation testing
Conclusion
Hyperkalaemia-induced Brugada syndrome.
Conflict of interest
None of the authors have any conflict of interest related to this report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Littmann L Monroe MH Taylor L 3rd Brearley WD Jr The hyperkalaemic Brugada sign J Electrocardiol 20074053910.1016/j.jelectrocard.2006.10.05717188975 · doi ↗ · pubmed ↗
- 2Postema PG Vlaar AP De Vries JH Tan HL Familial Brugada syndrome uncovered by hyperkalaemic diabetic ketoacidosis Europace 20111315091010.1093/europace/eur 15121576130 · doi ↗ · pubmed ↗
- 3Mizusawa Y Wilde AAM Arrhythmogenic disorders of genetic origin: brugada Syndrome Circ Arrhythm Electrophysiol 201256061610.1161/CIRCEP.111.96457722715240 · doi ↗ · pubmed ↗