Special Issue: Family Planning
Peter Byass, Babatunde Osotimehin, Yoonjoung Choi, Madeleine Short Fabic, Sennen Hounton, Desmond Koroma, Aluisio J. D. Barros, Ties Boerma, Ahmad R. Hosseinpoor, María C. Restrepo-Méndez, Kerry L. M. Wong, Cesar G. Victora, Abdoulaye Maïga, Sennen Hounton, Agbessi Amouzou

TL;DR
This paper analyzes global and regional progress toward meeting family planning goals by 2030, showing that most countries need to significantly accelerate their efforts.
Contribution
The study proposes a model to predict family planning coverage using contraceptive use prevalence, simplifying data collection in resource-limited settings.
Findings
To meet the 2030 benchmark, 63 countries need a 2.2 percentage point annual increase in modern contraceptive use, more than double current projections.
A predictive model using contraceptive use prevalence explains 95% of the variability in family planning coverage with high precision.
Low modern contraceptive use in Burkina Faso is linked to higher birth risks and child mortality, particularly in the Sahel, Est, and Sud-Ouest regions.
Abstract
In order to track progress towards the target of universal access to sexual and reproductive health care services of the post-2015 Sustainable Development Goals (SDGs), a measure (demand for family planning satisfied with modern contraceptive methods) and a benchmark (at least 75% by 2030 in all countries) have been recommended. The goal of this study was to assess the prospects of reaching the benchmark at the country level. Such information can facilitate strategic planning, including resource allocation at global and country levels. We selected 63 countries based on their status as least developed according to the United Nations or as a priority country in global family planning initiatives. Using United Nations estimates and projections of family planning indicators between 1970 and 2030, we calculated percent demand for family planning satisfied with modern contraceptive methods…
Click any figure to enlarge with its caption.
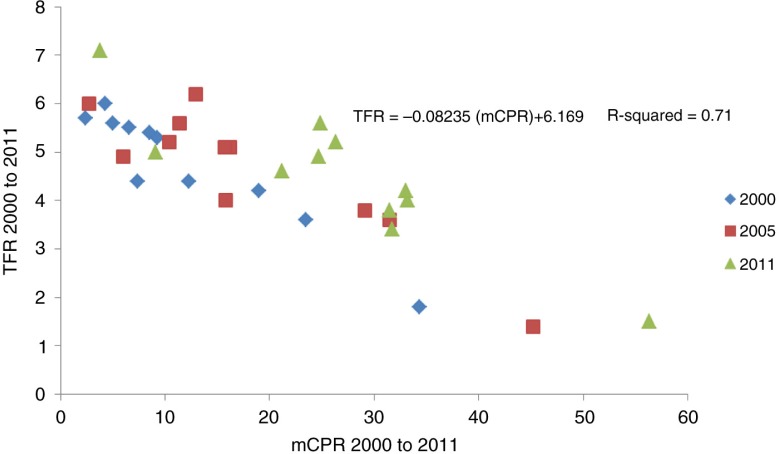 Figure 1
Figure 1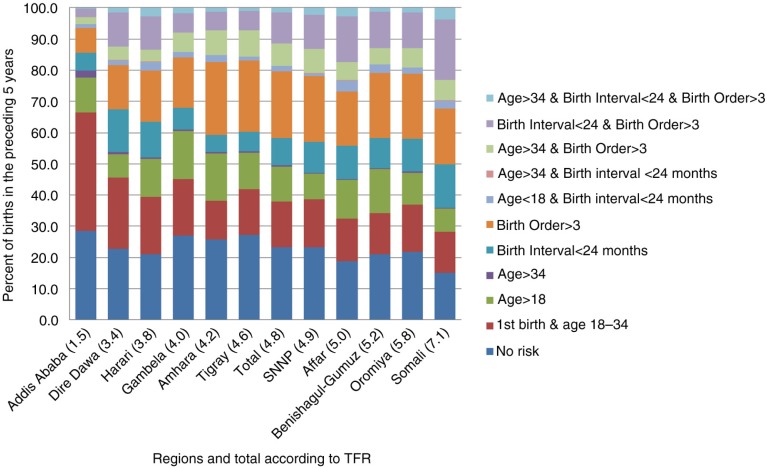 Figure 2
Figure 2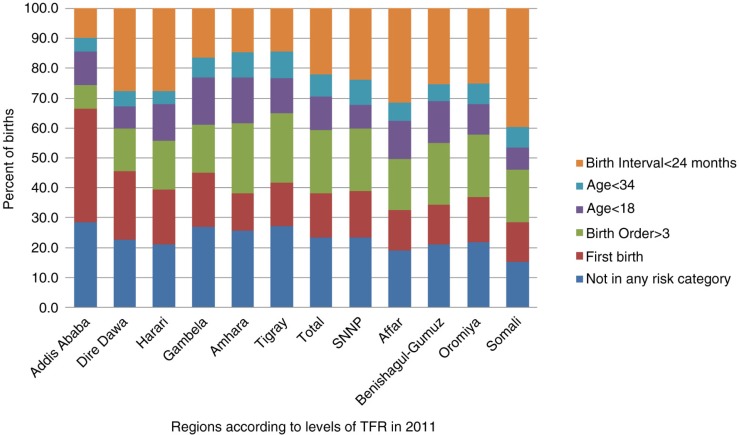 Figure 3
Figure 3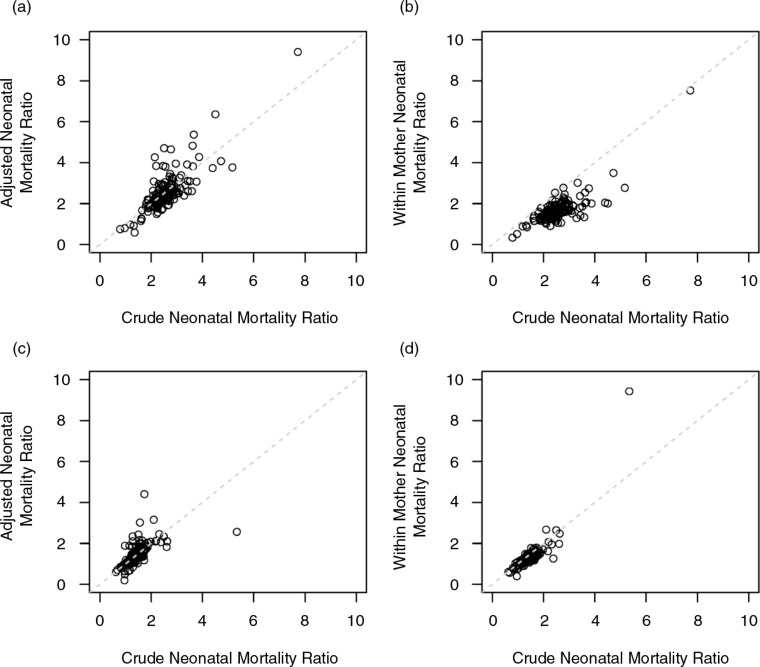 Figure 4
Figure 4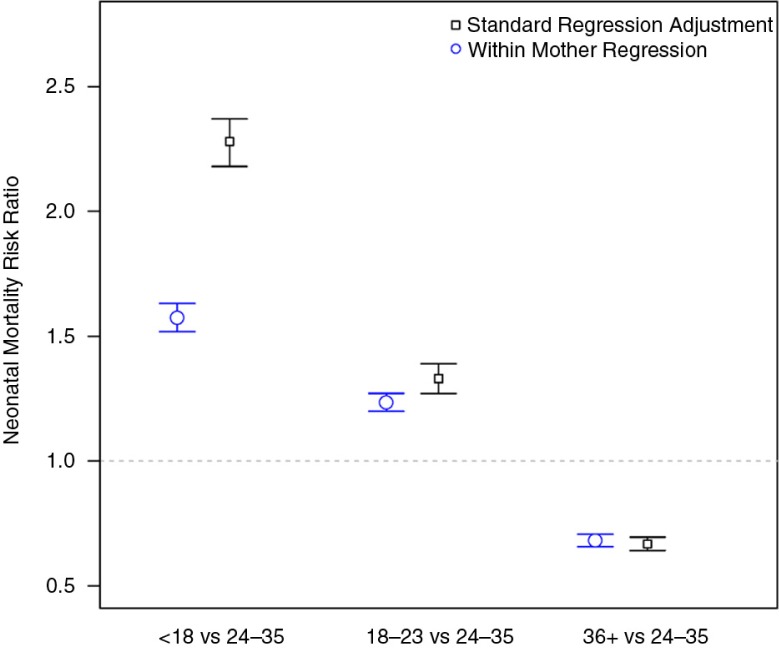 Figure 5
Figure 5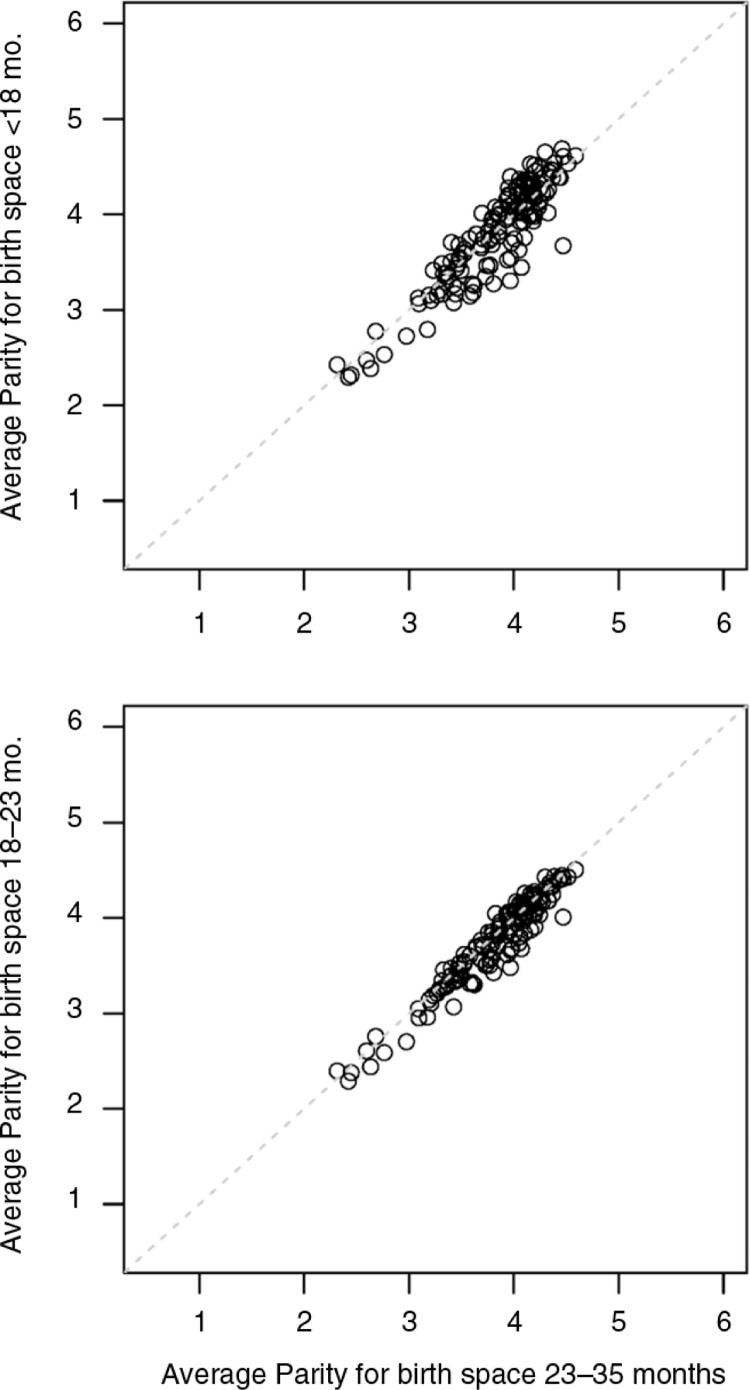 Figure 6
Figure 6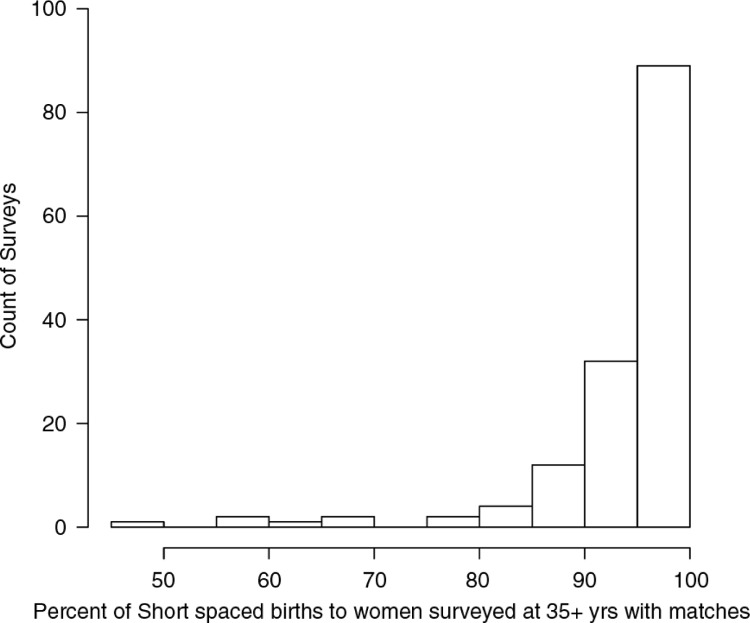 Figure 7
Figure 7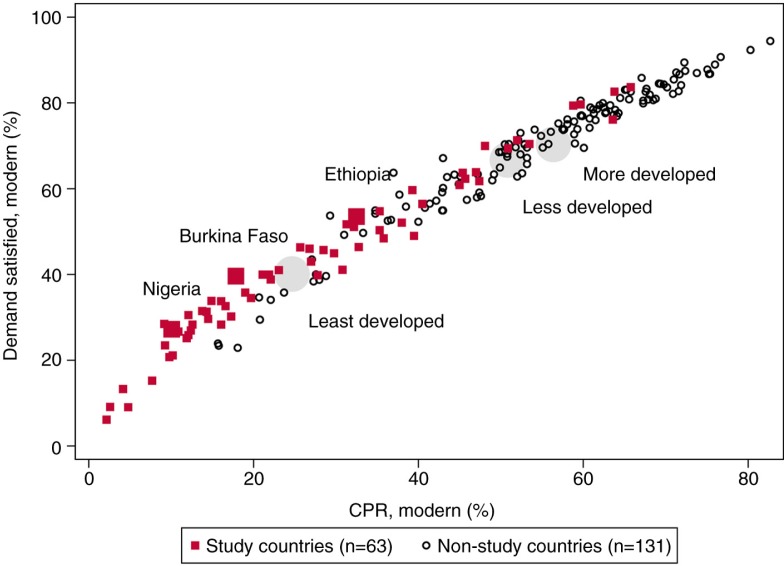 Figure 8
Figure 8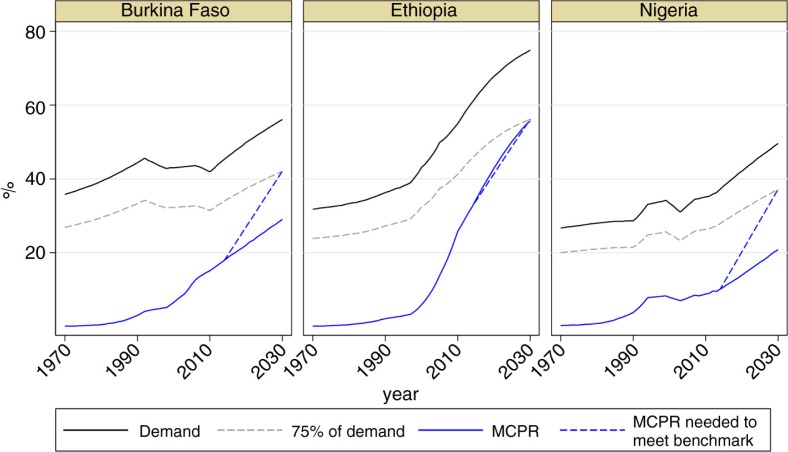 Figure 9
Figure 9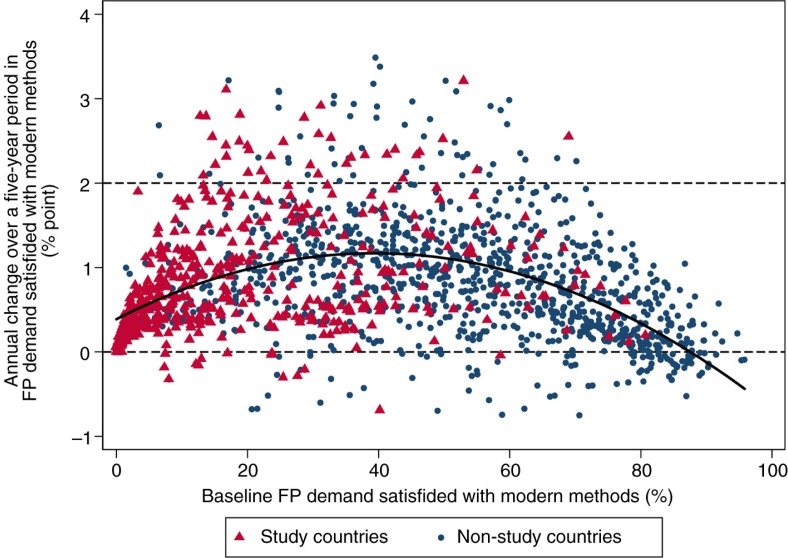 Figure 10
Figure 10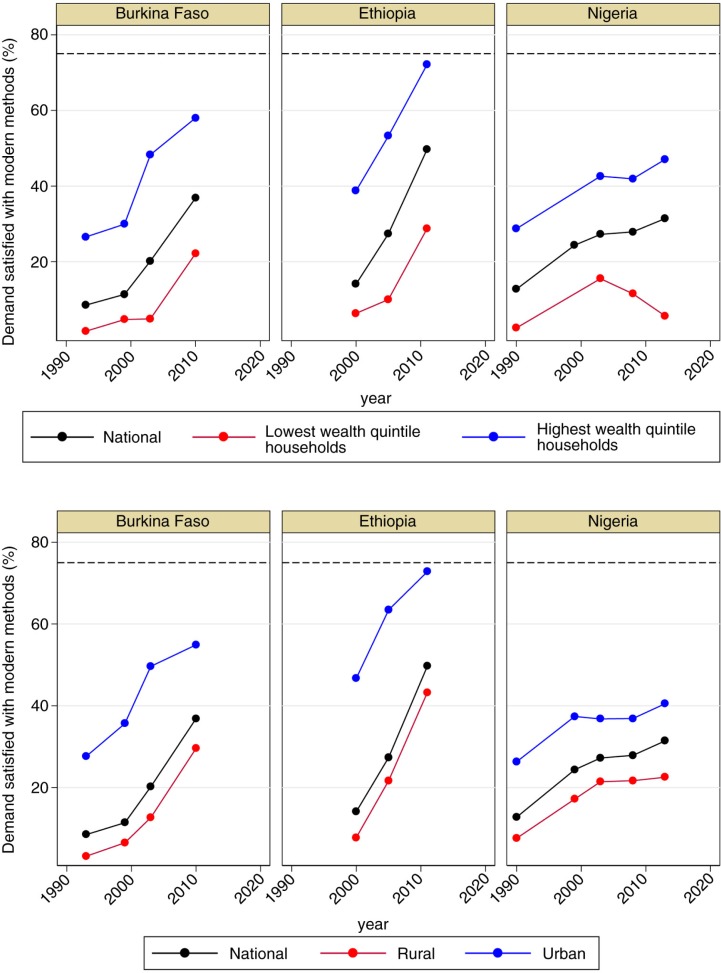 Figure 11
Figure 11 Figure 12
Figure 12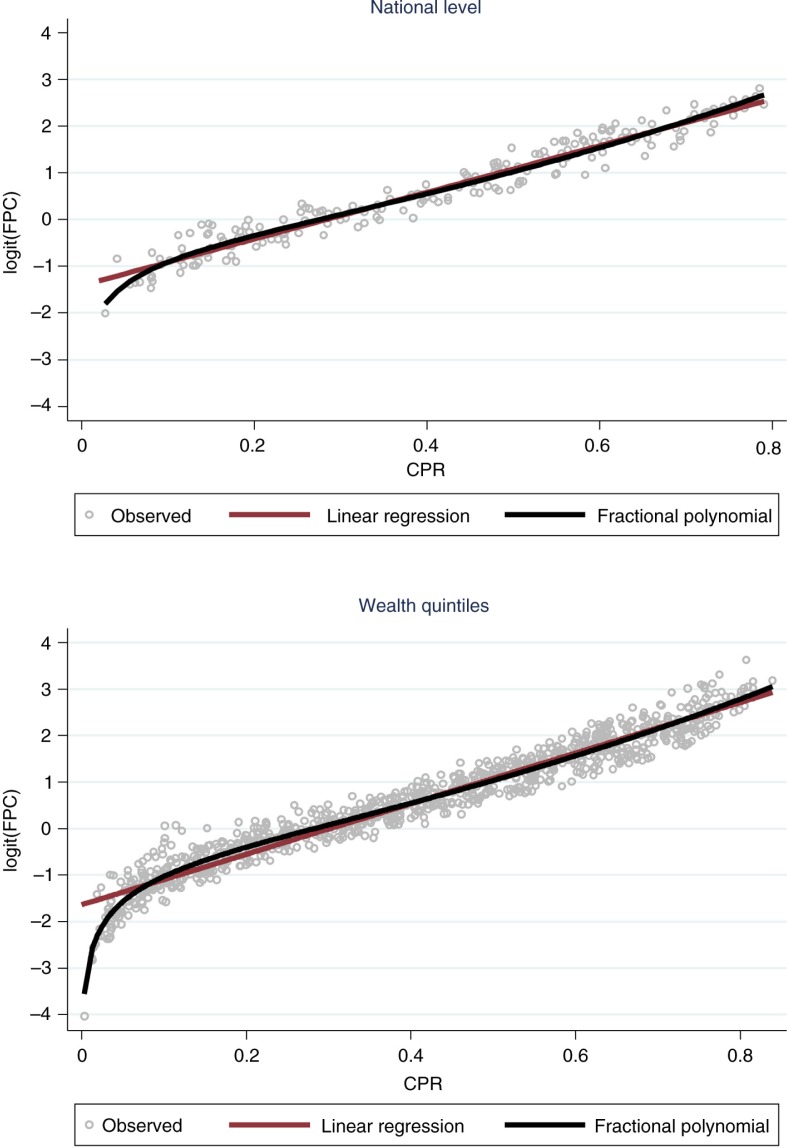 Figure 13
Figure 13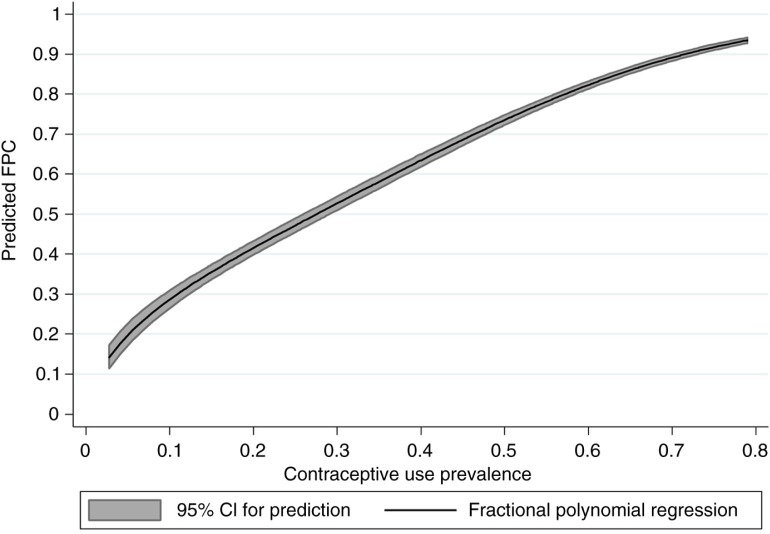 Figure 14
Figure 14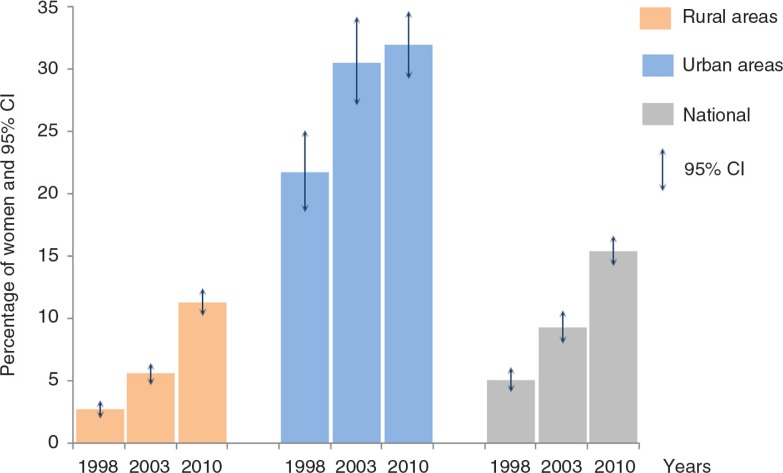 Figure 15
Figure 15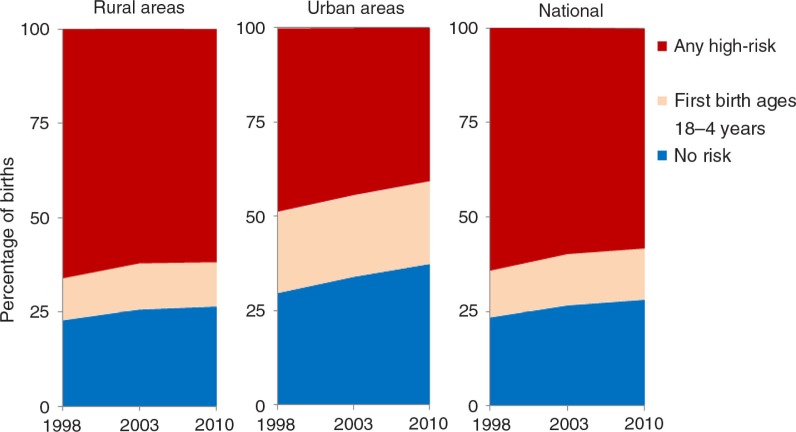 Figure 16
Figure 16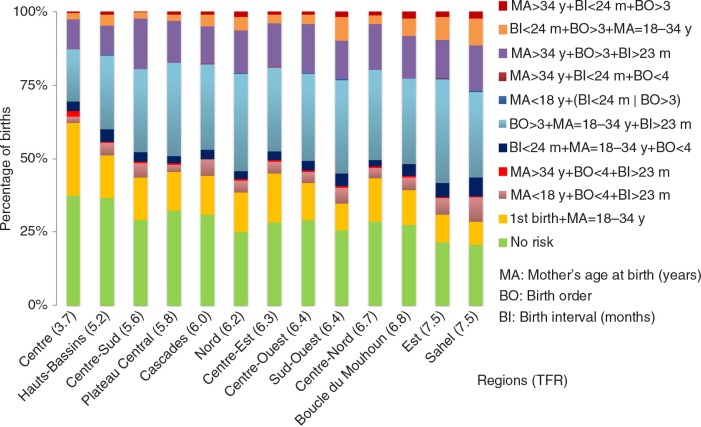 Figure 17
Figure 17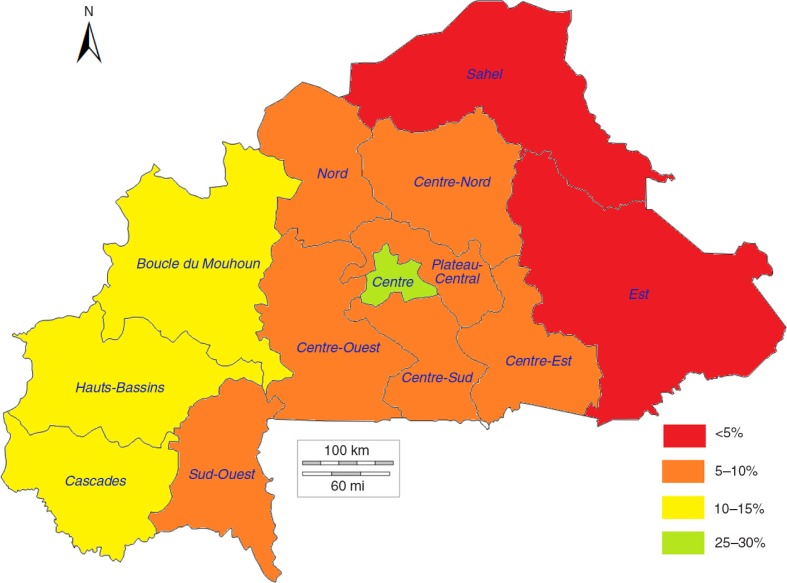 Figure 18
Figure 18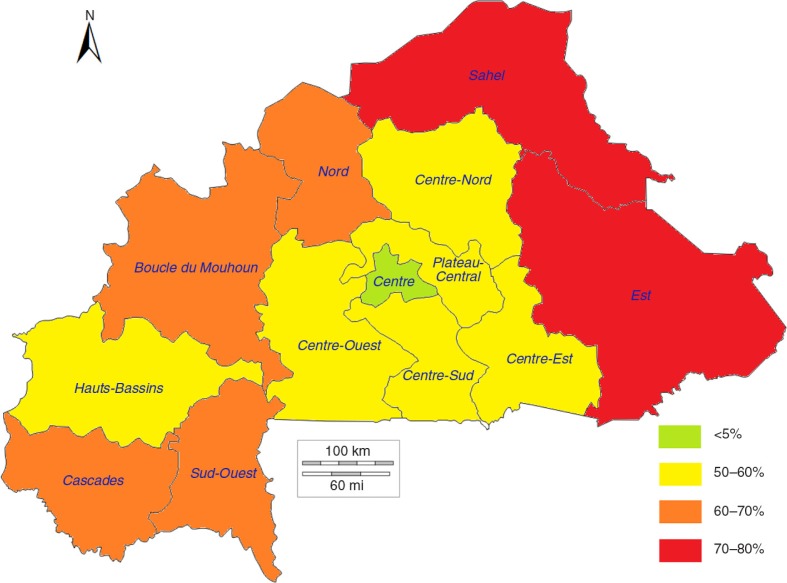 Figure 19
Figure 19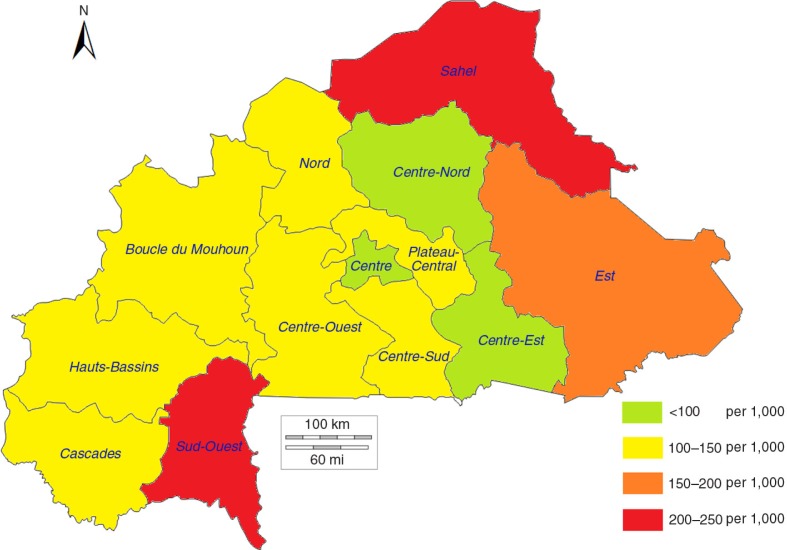 Figure 20
Figure 20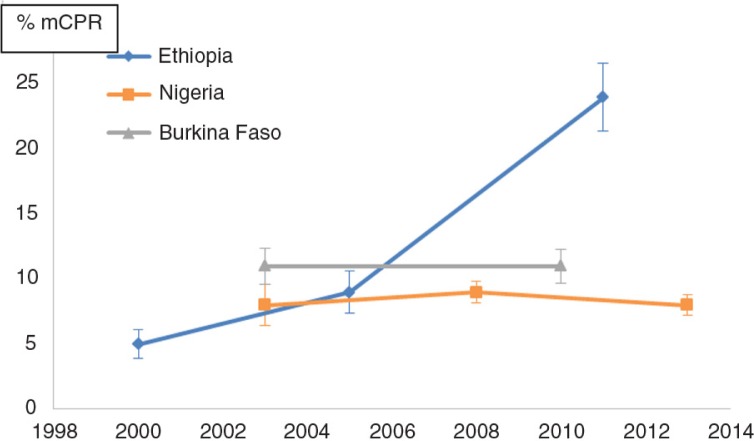 Figure 21
Figure 21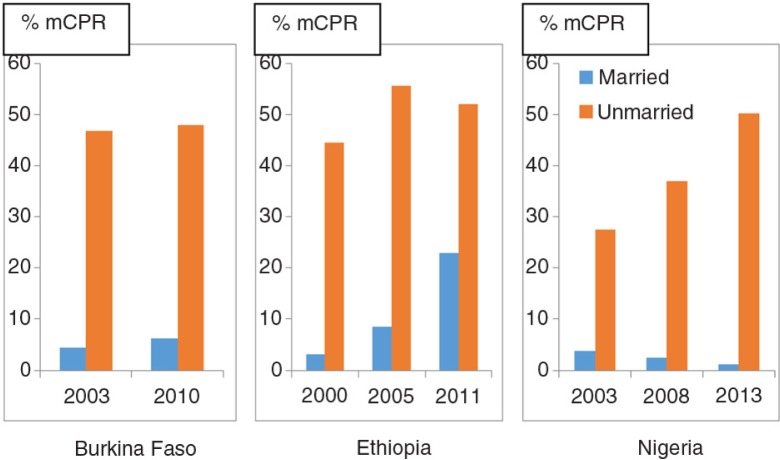 Figure 22
Figure 22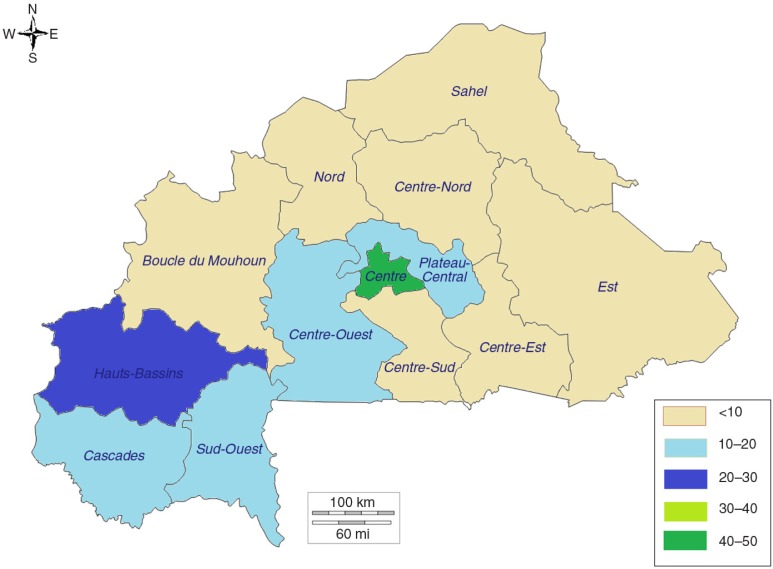 Figure 23
Figure 23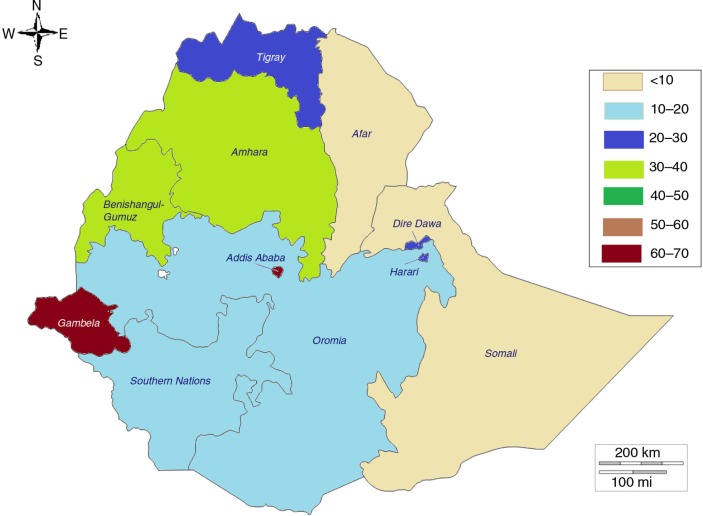 Figure 24
Figure 24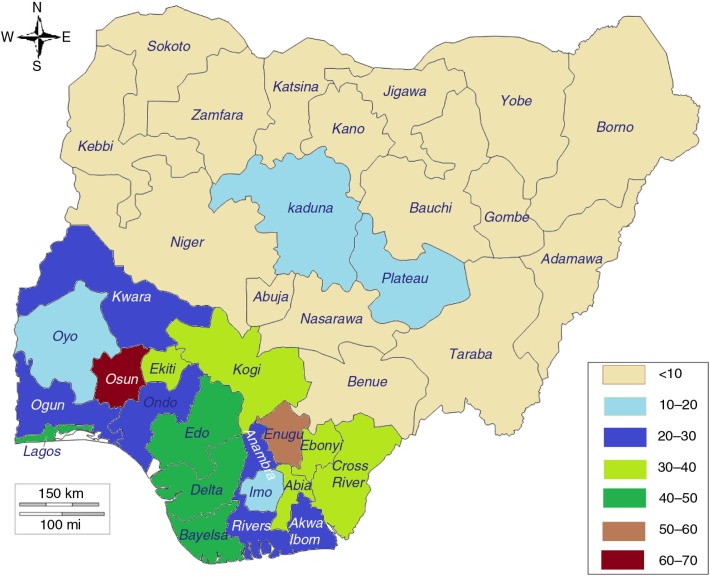 Figure 25
Figure 25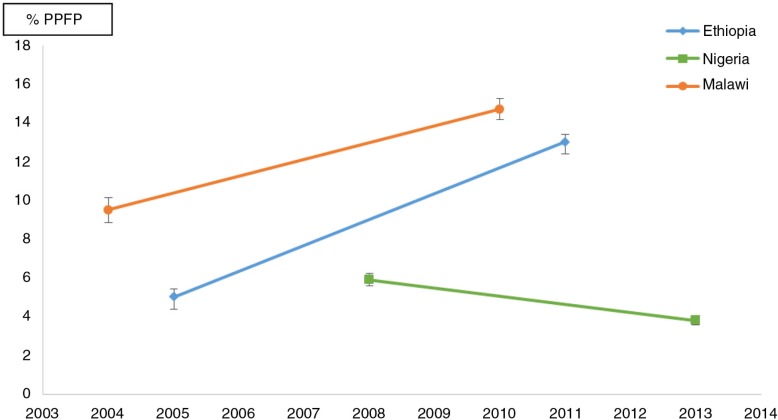 Figure 26
Figure 26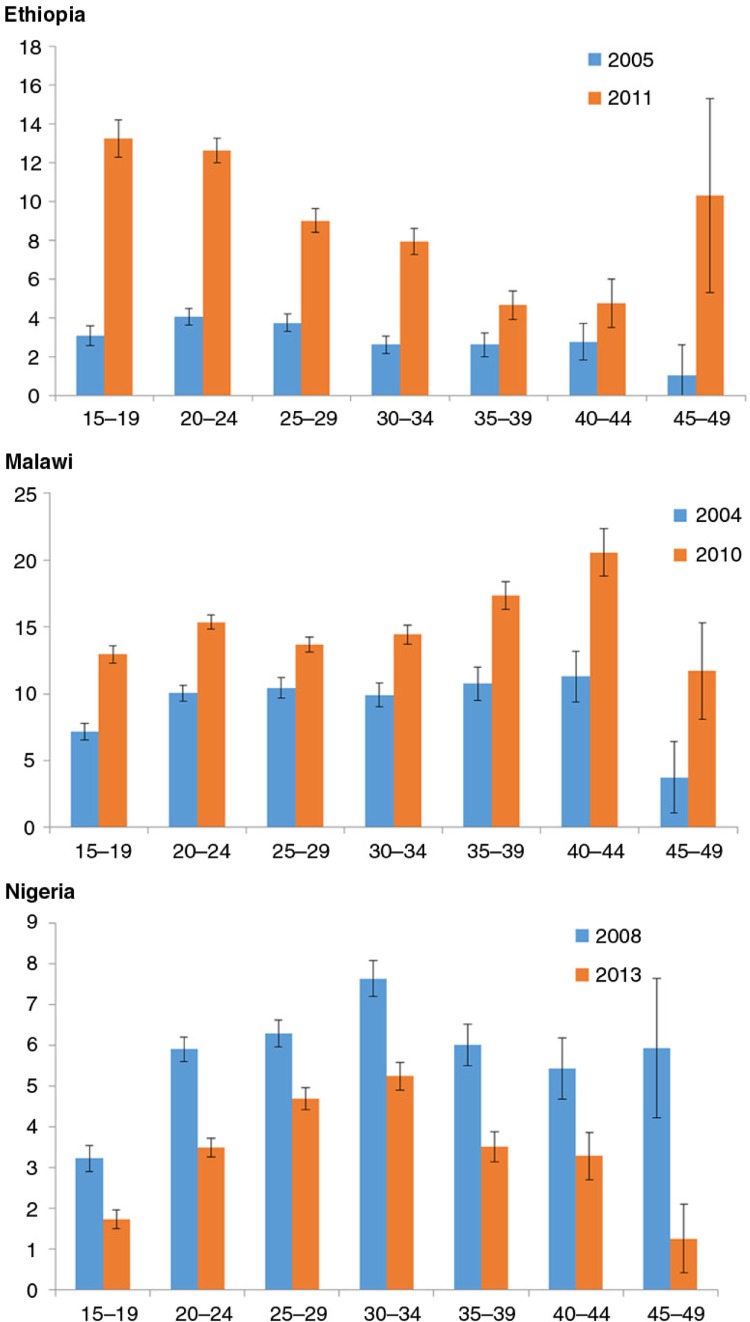 Figure 27
Figure 27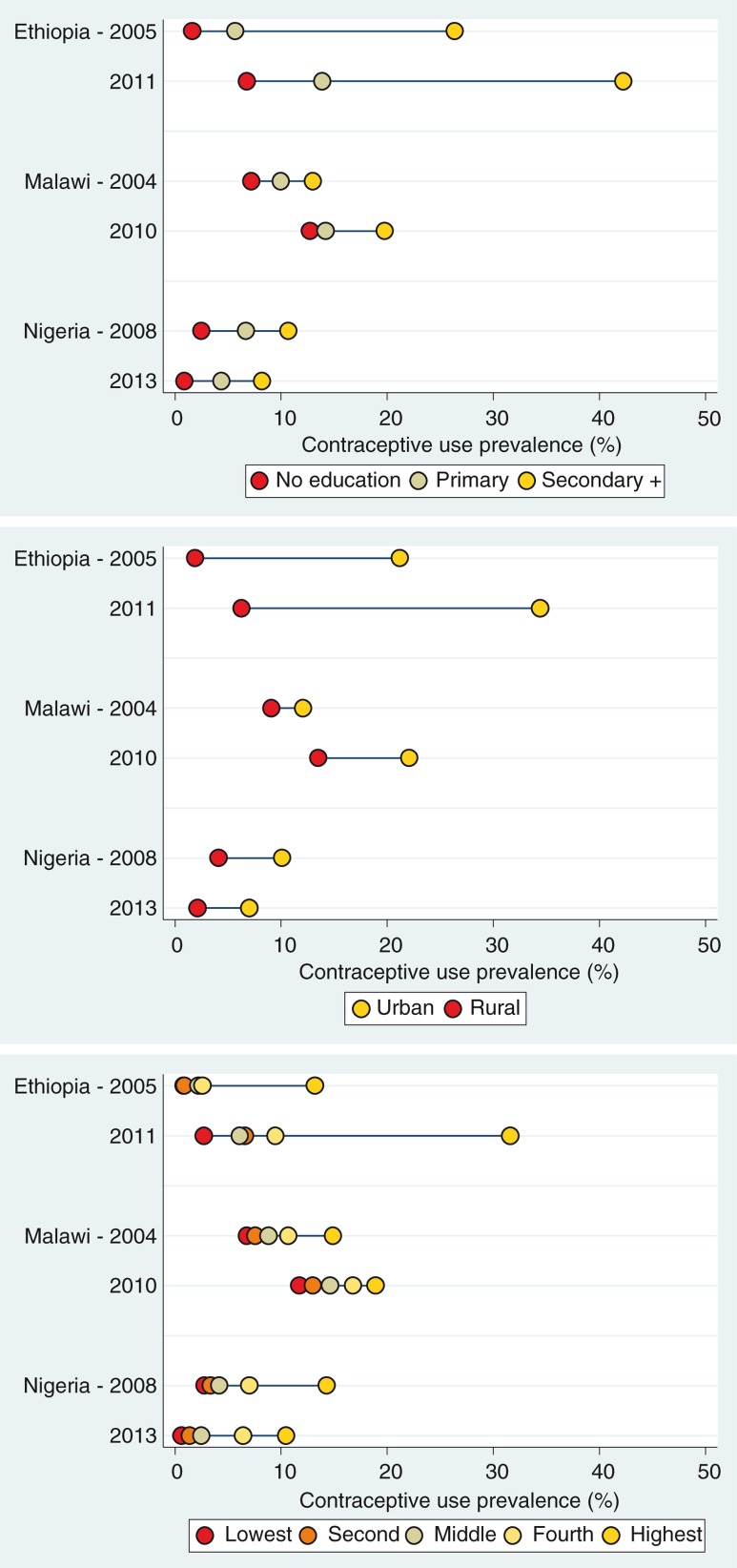 Figure 28
Figure 28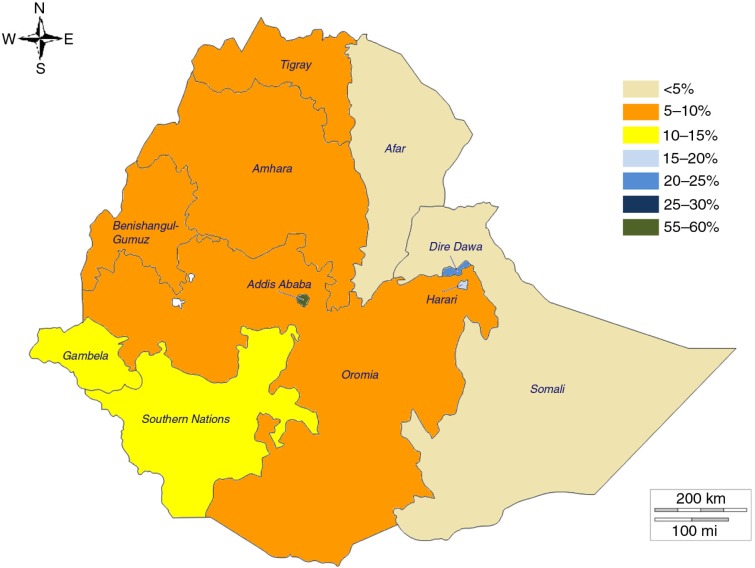 Figure 29
Figure 29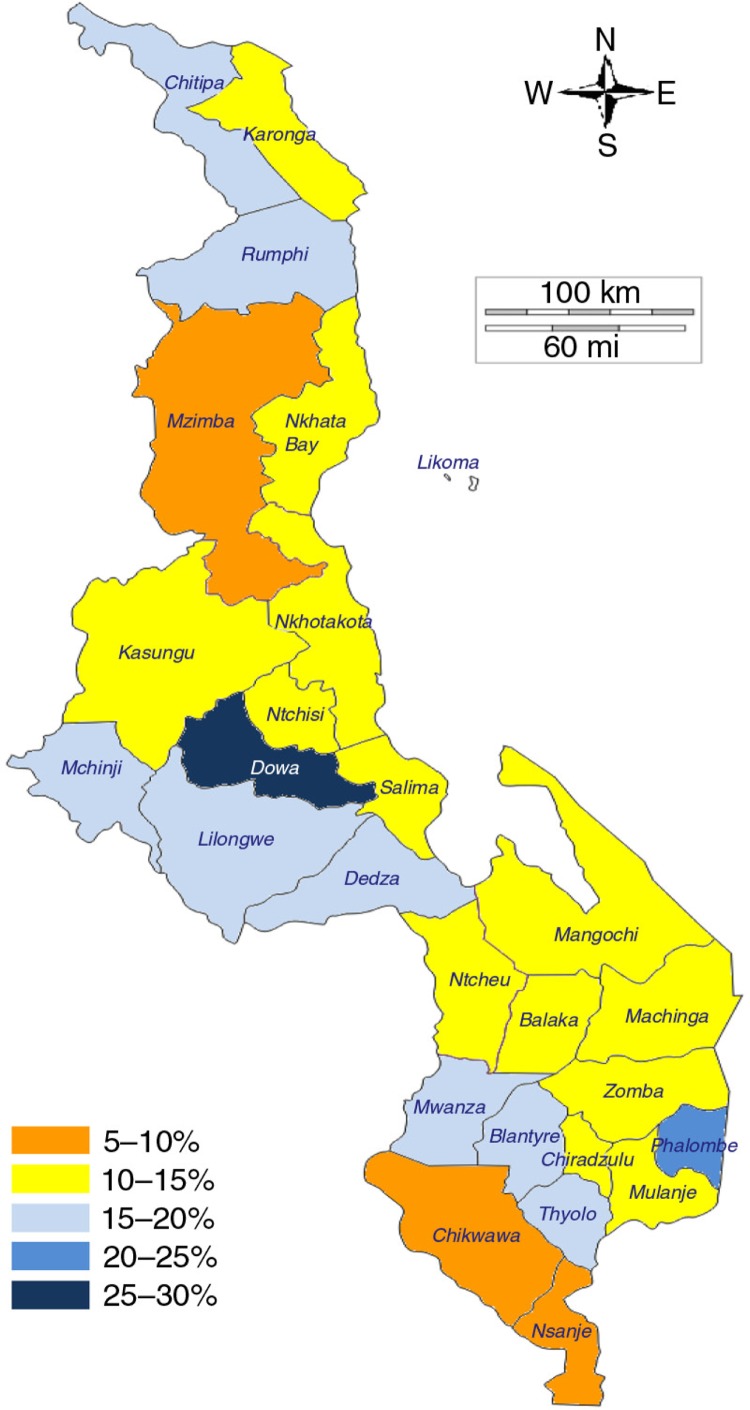 Figure 30
Figure 30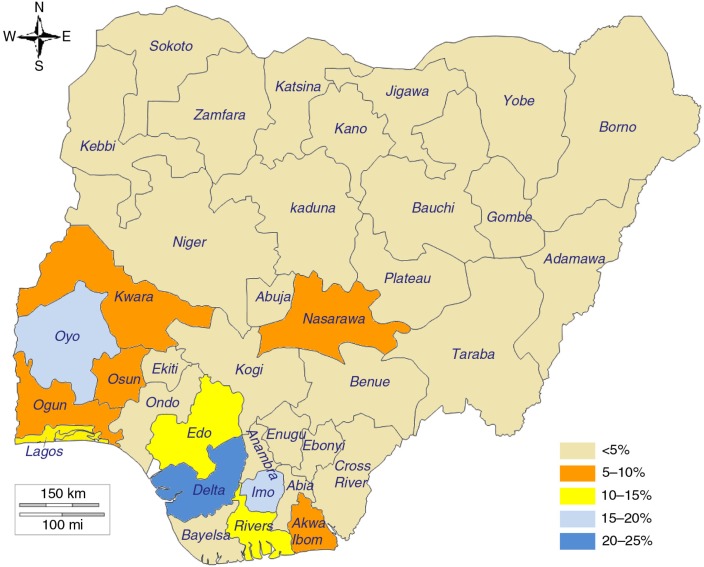 Figure 31
Figure 31 Figure 32
Figure 32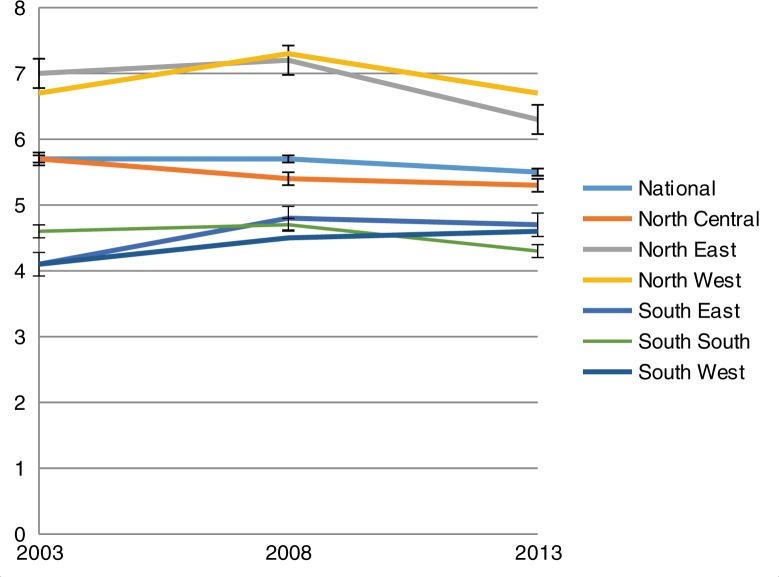 Figure 33
Figure 33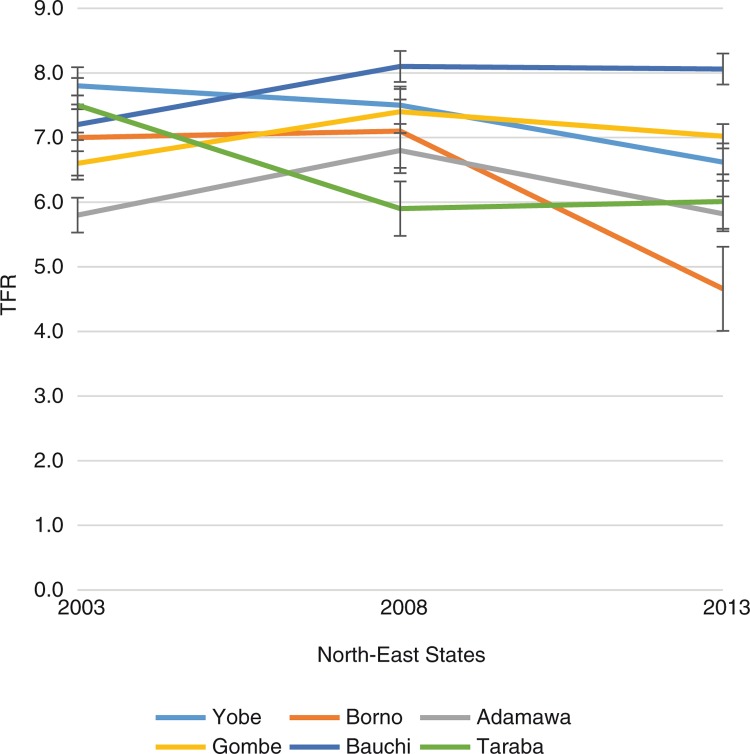 Figure 34
Figure 34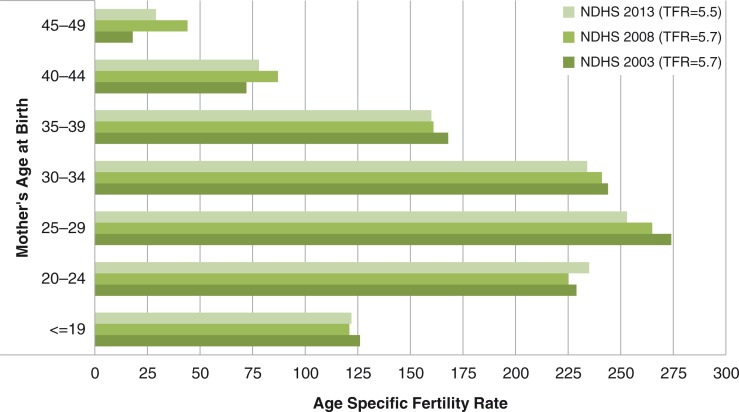 Figure 35
Figure 35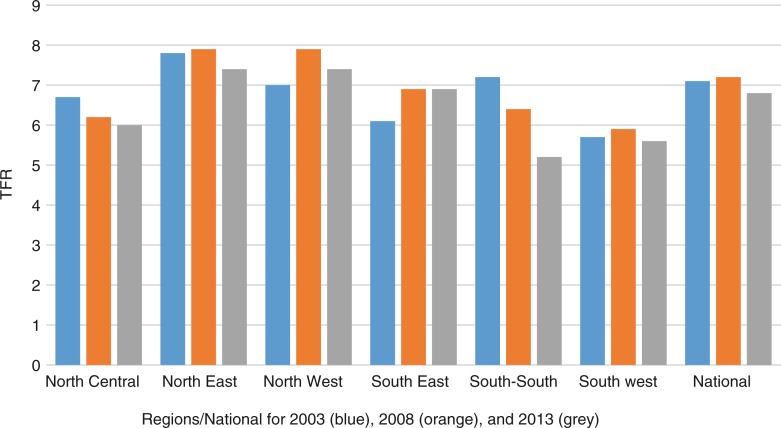 Figure 36
Figure 36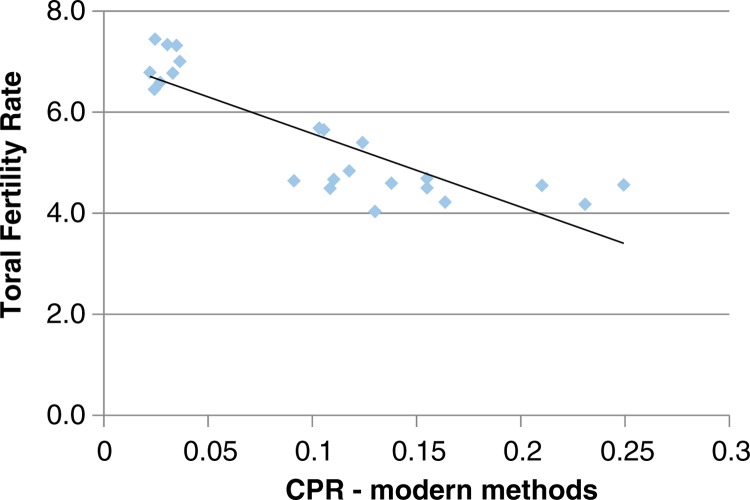 Figure 37
Figure 37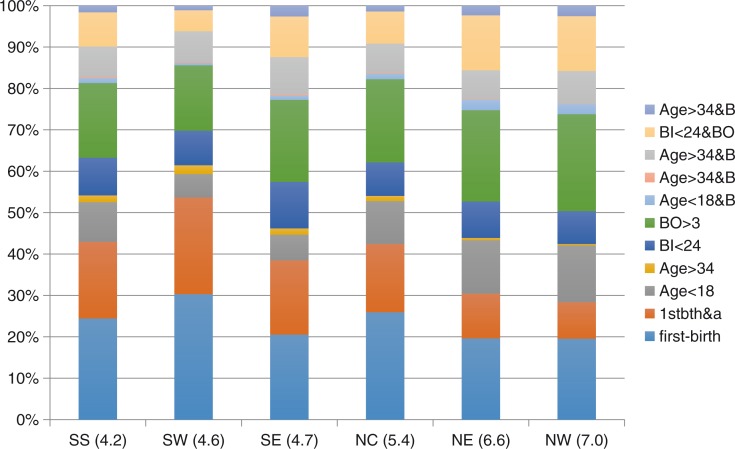 Figure 38
Figure 38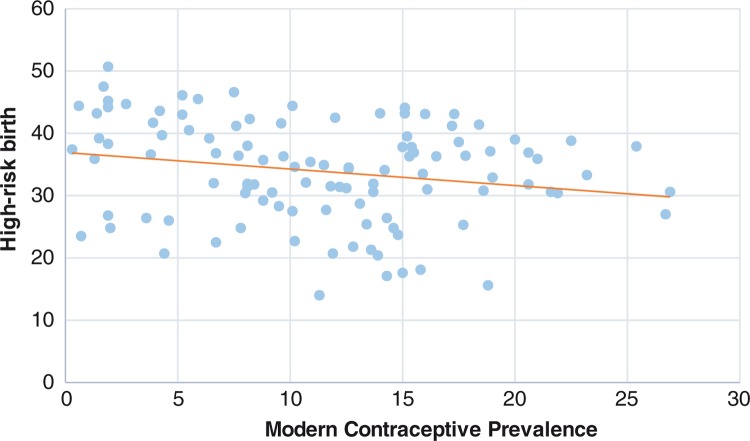 Figure 39
Figure 39Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health
In September 2015, under the leadership of United Nations Secretary-General Ban Ki-Moon, the international community took a huge step forward for people, the planet, and prosperity with the adoption of the 2030 Agenda for Sustainable Development. The 17 Sustainable Development Goals (SDGs) pave a brave path towards a world of equity and inclusion, health, including sexual and reproductive health and reproductive rights, education, and greater equality (1).
Over the 1990–2015 timeframe of the Millennium Development Goals and, particularly since the 1994 International Conference on Population and Development, considerable progress has been made in women's sexual and reproductive health, including increases in contraceptive use globally, expanded access to skilled maternity care, and the reduction of new HIV infections and maternal and newborn deaths. The secretary-general's ‘Every Woman Every Child’ strategy (2) has catalysed increased leadership and commitment from governments and strong support from all partners, including United Nations agencies, non-governmental organisations, foundations, academia and professional associations.
Behind the positive global trends, however, lie significant differences among and within countries. For example, around 225 million women in low- and middle-income countries (LMICs) who do not want to become pregnant are not using modern contraception. It is estimated that 30 million unplanned births and 40 million abortions, half of them illegal and unsafe, occur annually. An estimated 499 million new sexually transmitted infections (excluding HIV) occur annually, approximately half among girls and women (2, 3).
The papers in this Special Issue reinforce the centrality of universal access to modern contraception within the SDGs and targets set for 2030 (1). Indeed the research and findings presented here point to an ecological correlation between satisfying demand for family planning using modern contraceptives and economic development (4). To reach the proposed benchmark of 75%, demand satisfied with modern methods of contraception would need to increase by 2.2 percentage points annually between 2014 and 2030 – more than double the current projections on average across the 63 countries analysed. Such rapid progress would require significant effort, particularly to meet needs among adolescent girls. If the 75% benchmark were achieved, 334 million women across the LMICs studied would use a modern contraceptive method by 2030, compared to 226 million women in 2014.
Strategies to increase family planning coverage (FPC) have to be backed up by effective metrics for assessing progress. For this purpose, a new FPC indicator has been developed by the authors in this special issue, based on the prevalence of contraceptive use (5).
Although coverage is an important indicator, meeting unmet needs and ensuring universal access to human rights-based family planning will not be achieved without addressing equity and quality issues. In this Special Issue, some authors have taken a detailed look at differences in access and use at the subnational level and over time in three countries: Burkina Faso, Ethiopia, and Nigeria (6–8). In all three cases they discovered substantial variations in modern contraceptive use between rural and urban areas and by other socio-economic factors. Consistently across all three countries the results confirm an association between fertility history and modern contraceptive use, as well as between low modern contraceptive use and higher birth risks, leading to increased child mortality. Moreover, women living in rural areas have significantly higher odds of avoidable birth risks (and hence child mortality) compared to their counterparts living in urban areas. In Burkina Faso short birth spacing ranked as the highest risk in relation to child deaths (6).
As the world aspires to a situation in which every adolescent girl and woman has easy access to comprehensive sexuality education and contraceptive services, studies here on contraceptive use among sexually active adolescents in Burkina Faso, Ethiopia, and Nigeria (9) and postpartum family planning uptake in Ethiopia, Malawi, and Nigeria (10) also highlighted equity and quality issues. Health systems must address these issues as the global community moves towards universal access. Marriage at very young ages is not only a human rights issue in itself, but also a barrier to modern contraceptive use, and it thus disempowers girls. Adolescent girls experience significant inequality in access to modern contraception by education, residence, and wealth quintile. The results from Ethiopia, however, show that leadership and commitment at the country level can bring change. The authors reported a significant and systematic reduction of inequalities, but also a narrowing of the equity gap, most notably for childbearing adolescents with no education or living in rural areas.
Mortality risks associated with low birth spacing have been further studied to assess potential confounding in the association between short-birth intervals and increased neonatal, infant, and child mortality in order to better inform attributable effects (11). After adjusting for confounding, the authors reported that neonatal, infant, and child mortality remained strongly and significantly related to short birth intervals, albeit with a one third reduction in the attributable risk ratio.
Any resilient health system must take into account the provision of reproductive, maternal, newborn, and adolescent health services across the life cycle, including easy access to family planning. The findings in these papers point to missed opportunities for integrating maternal and newborn health, including failure to combine child immunisation with family planning, as the factor most associated with the non-uptake of modern contraception in the postpartum period (10).
As we celebrate the historic adoption of the SDGs and look ahead to their implementation, access to family planning represents an important entry point and a marker for universal access to reproductive health and rights. Access to modern contraception reduces the risks of maternal and newborn deaths (11) as well as reducing lifetime parity, and thus it affects health, life expectancy, and the dependency ratio. The availability of family planning affects education prospects and human capital among adolescent girls by preventing teenage pregnancies and enabling girls to stay in school. It could also improve access to food and reduce hunger by reducing the dependency ratio. Urbanisation and population dynamics are intrinsically linked, particularly internal and external migration, which have poverty as a root cause. Access to modern contraception can spur the economy, protect the environment, and contribute to overall poverty reduction.
The research findings in this Special Issue, which come from distinguished scientists in United Nations agencies, non-governmental organisations, and universities, present a range of global and local policy and programmatic priorities to address measurement, coverage, impact, quality and equity issues in family planning services, which are integral to the global sustainable development agenda. This is particularly important for countries in sub-Saharan Africa. We thus call on world leaders and financiers to join forces and work towards the future we want, a future in which every pregnancy is wanted, every birth is safe, and every young person's potential is fulfilled.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1United Nations Sustainable Development Goals 2015 New York United Nations
- 2United Nations Every woman every child 2015 New York United Nations
- 3Temmerman M Khosla R Bhutta ZA Bustreo F Towards a new global strategy for women's, children's and adolescents’ health BMJ 2015351 Suppl 1441410.1136/bmj.h 441426371228 · doi ↗ · pubmed ↗
- 4Choi Y Fabic MS Hounton S Koroma D Meeting demand for family planning within a generation: prospects and implications at country-level Glob Health Action 2015829734, doi: http://dx.doi.org/10.3402/gha.v 8.2973410.3402/gha.v 8.29734 PMC 464236926562140 · doi ↗ · pubmed ↗
- 5Barros AJD Boerma T Hosseinpoor AR Restrepo-Méndez MC Wong KLM Victora CG Estimating family planning coverage from contraceptive prevalence using national household surveys Glob Health Action 2015829735, doi: http://dx.doi.org/10.3402/gha.v 8.2973510.3402/gha.v 8.29735 PMC 464236126562141 · doi ↗ · pubmed ↗
- 6Maïga A Hounton S Amouzou A Akinyemi A Shiferaw S Baya B Trends and patterns of modern contraceptive use and relationships with high-risk births and child mortality in Burkina Faso: a sub-national analysis Glob Health Action 2015829736, doi: http://dx.doi.org/10.3402/gha.v 8.2973610.3402/gha.v 8.29736 PMC 464235926562142 · doi ↗ · pubmed ↗
- 7Shiferaw S Abdullah M Mekonnen Y Maïga A Akinyemi A Amouzou A Trends in modern contraceptive use and distribution of births with demographic risk factors in Ethiopia: a sub-national analysis Glob Health Action 2015829720, doi: http://dx.doi.org/10.3402/gha.v 8.2972010.3402/gha.v 8.29720 PMC 464236826562138 · doi ↗ · pubmed ↗
- 8Akinyemi A Adedini S Hounton S Akinlo A Adedeji O Adonri O Trends in modern contraceptive use and distribution of high-risk births in Nigeria: a sub-national analysis Glob Health Action 2015829745, doi: http://dx.doi.org/10.3402/gha.v 8.2974510.3402/gha.v 8.29745 PMC 464236326562145 · doi ↗ · pubmed ↗