SEED: the six excesses (Liu Yin) evaluation and diagnosis scale
Pei-Jung Chiang, Tsai-Chung Li, Chih-Hung Chang, Li-Li Chen, Jun-Dai Lin, Yi-Chang Su

TL;DR
This paper introduces a new diagnostic scale for infectious diseases based on traditional Chinese medicine's six excesses theory.
Contribution
The SEED scale is a novel diagnostic tool derived from Chinese medicine's Liu Yin theory using the Delphi method.
Findings
178 diagnostic items were selected with expert consensus ratings of 7 or above.
The SEED scale categorizes symptoms into six excess syndromes for infectious disease diagnosis.
The scale relies solely on signs and symptoms without laboratory tests.
Abstract
Infections such as common colds, influenza, acute upper respiratory infections, bacterial gastroenteritis, and urinary tract infections are usually diagnosed according to patients’ signs and symptoms. This study aims to develop a scale for the diagnosis of infectious diseases based on the six excesses (Liu Yin) etiological theory of Chinese medicine (CM) by the Delphi method. A total of 200 CM-guided diagnostic items measuring signs and symptoms for infectious diseases were compiled from CM literature archives from the Han to Ming dynasties, CM textbooks in both China and Taiwan, and journal articles from the China Knowledge Resource Integrated Database. The items were based on infections and the six excesses (Liu Yin) etiological theory, i.e., Feng Xie (wind excess), Han Xie (coldness excess), Shu Xie (summer heat excess), Shi Xie (dampness excess), Zao Xie (dryness excess), and Huo…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
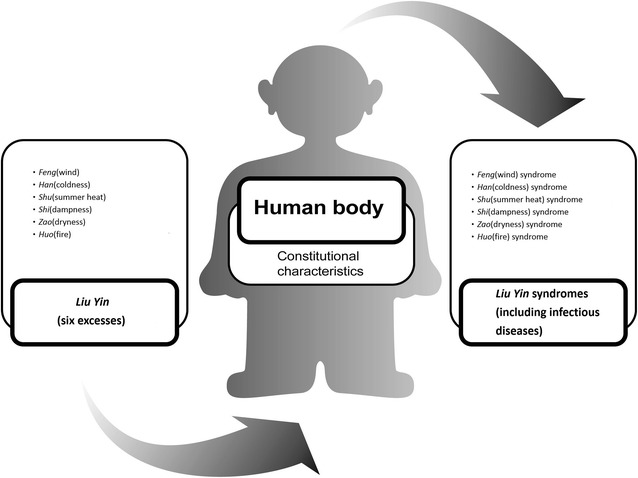 Figure 1
Figure 1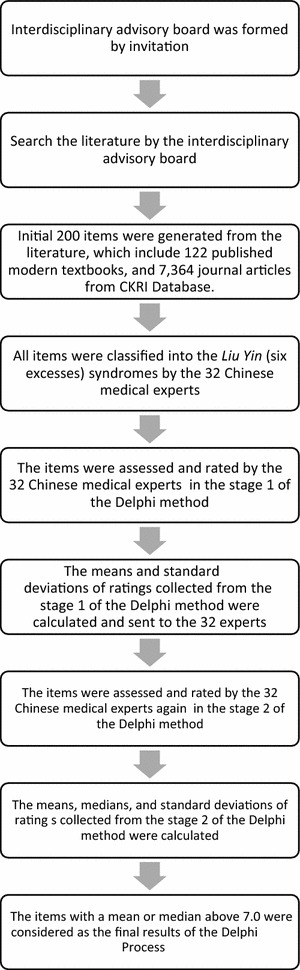 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClassical Antiquity Studies · Augustinian Studies and Theology
Background
Infections such as common colds, influenza, acute upper respiratory infections, bacterial gastroenteritis, and urinary tract infections are usually diagnosed according to patients’ signs and symptoms, while the diagnosis of pandemic infections such as influenza H1N1 [1–4] and H5N1 [5, 6] must be confirmed by expensive laboratory tests [7–9] or real-time RT-PCR assays of multiple specimens [10]. Pathogen testing in the laboratory might be of low sensitivity [11], and low accuracy in some cases [12–14], and above all time-consuming [15].
Chinese medicine (CM) can detect those infectious diseases mentioned above according to the etiological theory of Liu Yin (six excesses), i.e., Feng Xie (wind excess) representing varying temperature factors, Han Xie (coldness excess) representing falling temperature, Shu Xie (summer heat excess) representing rising temperature and humidity, Shi Xie (dampness excess) representing rising humidity, Zao Xie (dryness excess) representing falling humidity, and Huo Xie (fire excess) representing rising temperature [16, 17]. These Liu Yin (six excesses) collectively describe the circumstantial influences on Qi and Xue (blood), encompassing a number of CM diagnostic criteria checked by inquiry, inspection, olfaction, audition, percussion, palpation, and pulse examination (Fig. 1), and facilitate diagnostic and therapeutic decisions [18]. However, there has been no standard diagnostic assessment or measurement scales designed for infectious diseases based on the Liu Yin (six excesses) theory [19–28].Fig. 1. Infectious diseases were classifiable in CM according to the Liu Yin (six excesses), Feng (wind), Han (coldness), Shu (summer heat), Shi (dampness), Zao (dryness), and Huo (fire), and could be classified into Feng (wind), Han (coldness), Shu (summer heat), Shi (dampness), Zao (dryness), and Huo (fire) syndromes
This study aims to develop the six excesses (Liu Yin) evaluation and diagnosis (SEED) scale for infectious diseases based on the Liu Yin (six excesses) etiological theory in CM by a Delphi process among experts. The Delphi method aims to build consensus and generate ideas in research fields [29–41], and is useful for the establishment of diagnostic criteria in clinical medicine. It is a structured communication process to establish the definition of the syndromes, the diagnostic criteria or the staging of the diseases, and the suggested treatments in the medical guidelines [42–48].
Methods
The Delphi method [49] was used to achieve a group panel consensus on the diagnostic items for the Liu Yin (six excesses) syndromes among a panel of experts between 2007 and 2008. A nationally representative panel of Chinese medical experts were invited; only CM experts with good knowledge about CM and modern research methods with master or doctoral degrees, and more than 7 years of practicing experience were invited to join the Delphi panel. Based on this consensus, we carried out further statistical analyses for infectious diseases.
An interdisciplinary advisory board was formed by seven members, including five CM experts, one measurement methodologist, and one statistician. The advisory board selected the participants of the Delphi panel.
Representatives from various education backgrounds, medical disciplines, geographical distributions, and clinical experience were considered for the panel. Finally, a total of 32 CM experts meeting these criteria were invited, and all agreed to participate (Table 1). Of the 32 participants, 20 were from CM departments in medical centers, 6 were from district or regional teaching hospitals, and 6 were from private practices; 7 practiced in Northern region, 11 in central region, 6 in Southern region and 8 in other region. Twenty-one panelists held master degrees, 11 had doctoral degrees in medical sciences, and 26 panelists were teachers in academic institutions. The age (mean ± SD) of the panelists was 43 ± 7.0 years with a median of 42 years. The year of practicing experience (mean ± SD) was 11.3 ± 3.7 years with a median of 10 years.Table 1. Basic characteristics of the 32 CM expertsAge, mean (SD), years Average43 (SD = 7.0) Median42Spectrum of practice, mean (SD), years Average11.3 (SD = 3.7) Median10Educational background, n (%) Master degree21 (65.6 %) Doctorate degree11 (34.4 %)Geographic distribution, n (%) Northern7 (21.9 %) Central11 (34.4 %) Southern6 (18.8 %) Other8 (25.0 %)Practice institution, n (%) Medical centers20 (62.5 %) District teaching hospitals5 (15.6 %) Regional teaching hospitals1 (3.1 %) Private practices6 (18.8 %)Teaching in an academic institution, n (%) Yes26 (81.3 %) No6 (18.8 %)
The Delphi process was iterative. We began with a systematic review of traditional CM literature including the Medicine Encyclopedia collected by Kentang Wang (AC1552–1639), 122 published modern textbooks, and 7364 journal articles from the China Knowledge Resource Integrated Database. The search keywords included: Feng (wind), Han (coldness), Shu (summer heat), Shi (dampness), Zao (dryness), Huo (fire), Wai-gan (external contraction), Liu Yin (six excesses), and Yin (excess), and we identified and compiled a pool of 200 diagnostic items for the Liu Yin (six excesses) syndromes. The CM experts categorized each of these 200 items into one of the Liu Yin (six excesses) syndromes, and the results were reviewed and face-validated by the same experts. The numbers of items for each Yin (excess) syndrome were: Feng (wind), 23; Han (coldness), 32; Shu (summer heat), 25; Shi (dampness), 40; Zao (dryness), 18; and Huo (fire), 62. We had mailed the items to the panelists and invited them to add any items; the numbers remained the same.
The classified items were then incorporated into the processes of the Delphi method and circulated via mail to the panelists for their ratings with follow-up phone calls within 2 weeks (Fig. 2). In stage 1, the panelists were asked to rate the appropriateness of each of the classified signs and symptoms on a scale of 1 (highly inappropriate) to 9 (highly appropriate). They were also instructed to provide reasons for the items they rated as “inappropriate”. In stage 2, the results for the mean rating and standard deviation of the individual items were mailed to the panelists, and they were asked again to provide and return their ratings after reviewing the results. The two-stage Delphi method are enough to saturate consensus [49–57], which cannot be maximized by increasing the number of round [58–64]. The progress was assessed by any reduction in the variability of judgments among the panelists. The level of consensus was quantified by the standard deviation of their ratings. After the two-stage Delphi method, the expert-rated diagnostic items with an average or median rating of 7 or above were considered to have face-validity and integrated into the standardized assessment. The cut point of 7.0 had been chosen because it highly represents panelists’ agreement as well as the estimated time required to complete the selected items by CM doctors is expected to be no more than 30 min.Fig. 2. Flow chart of the Delphi process
Results
The mean, median and standard deviation of the ratings for each item from the first and second stages were calculated (Table 2). After the two-stage Delphi method, 15, 22, 25, 37, 17, and 62 diagnostic items with a rating of 7.0 or higher were retained in Feng (wind), Han (coldness), Shu (summer heat), Shi (dampness), Zao (dryness), and Huo (fire) syndromes, respectively. The standard deviations of all 178 retained items decreased from the first stage to the second stage because of the achieved agreement, with the following exceptions: “surging but weak pulse with dipped finger tip” (both 1.02) and “unclear head and eyesight” (1.01–1.06) in Shu (summer heat) syndrome; “edematous swelling in face and limbs” (both 1.10) and “unclear head and eyesight” (both 0.67) in Shi (dampness) syndrome; and “dry and yellow fur” (1.01–1.06) and “dry, yellow and white fur” (0.61–0.63) in Huo (fire) syndrome. However, the upward changes were relatively small.Table 2. Results of the two-stage Delphi methodSyndromeNo.ItemStage 1Stage 2Mean (SD)MedianMean (SD)Median Feng (wind) syndrome1Aversion to wind^a^ 8.03 (1.06)88.28 (0.96)82Floating pulse^a^ 7.63 (1.41)77.78 (0.87)73Itchy throat^a^ 7.25 (1.16)77.41 (0.80)74Headache^a^ 7.09 (1.30)67.16 (0.51)6.55Headache and painful stiffness in nape^a^ 7.06 (1.34)77.06 (0.80)76Floating and relaxed pulse^a^ 7.00 (1.42)67.28 (0.82)77Clear snivel^a^ 6.97 (1.23)77.09 (0.69)78Sneezing^a^ 6.94 (1.34)57.13 (0.79)59Pain at unfixed location6.88 (2.03)66.91 (1.09)610Painful stiffness in nape and back6.84 (1.22)66.84 (0.95)511Floating and rapid pulse^a^ 6.81 (1.42)77.19 (0.82)712Generalized pain^a^ 6.75 (1.59)77.06 (0.67)713Nasal congestion^a^ 6.69 (1.31)77.13 (0.75)714Cough, productive^a^ 6.59 (1.46)77.06 (0.67)715Floating and weak pulse^a^ 6.53 (1.65)76.59 (1.07)716Aches and pains in joints6.44 (1.39)5.56.69 (0.59)517Generalized itching6.44 (1.68)5.56.44 (1.37)518Thin white fur6.38 (1.79)66.50 (1.05)619Pale red tongue6.28 (1.90)66.41 (0.98)620Deviated eye and mouth6.16 (1.92)85.84 (1.44)821Opisthotonos^a^ 5.63 (2.23)75.09 (1.40)722Trismus (lockjaw)^a^ 5.53 (2.17)75.06 (1.37)723Hemiplegia5.22 (2.35)65.13 (1.43)6 Han (coldness) syndrome1Aversion to cold^a^ 8.22 (0.87)8.58.41 (0.61)82Floating and tight pulse^a^ 7.66 (1.10)77.78 (0.79)73Preference for hot drinks^a^ 7.53 (1.37)77.53 (0.67)74Clear phlegm^a^ 7.53 (0.98)77.47 (0.57)75Clear snivel^a^ 7.41 (0.95)67.50 (0.67)76A lot of clear and white phlegm^a^ 7.38 (1.07)77.34 (0.60)77Generalized pain^a^ 7.13 (1.34)77.41 (0.67)78Headache and painful stiffness in nape^a^ 7.13 (1.18)77.28 (0.58)79Shivering^a^ 7.06 (1.37)77.22 (0.91)710Ache in limbs^a^ 7.00 (1.39)77.28 (0.73)711Cold body and limbs^a^ 7.00 (1.87)77.28 (0.96)712Tight pulse^a^ 6.94 (1.39)67.13 (1.16)613Aches and pains in joints^a^ 6.88 (1.50)67.28 (0.58)614White and moist fur6.88 (1.50)66.81 (1.00)615Not thirsty^a^ 6.84 (1.32)67.03 (0.93)616White, moist and thin fur^a^ 6.84 (1.51)76.94 (0.95)717No desire to drink6.84 (1.27)66.81 (0.90)618Clear urine^a^ 6.81 (1.64)76.78 (0.75)719Painful stiffness in nape and back^a^ 6.78 (1.72)76.91 (0.95)720White and thin fur6.78 (1.72)66.84 (0.95)621Absence of sweating^a^ 6.69 (1.64)77.13 (1.01)722Cold feeling on nape and back6.69 (1.45)76.94 (0.76)623Headache^a^ 6.63 (1.36)77.06 (0.95)824Cough, productive6.53 (1.24)76.75 (0.72)625White fur6.53 (1.78)76.59 (1.01)626Sloppy stool6.50 (1.32)76.66 (1.00)627Reversal cold of extremities6.50 (1.80)76.59 (1.24)628White and slippery fur^a^ 6.44 (1.63)76.50 (1.02)729Nasal congestion6.38 (1.36)76.81 (0.63)630Sneezing6.38 (1.34)66.81 (0.64)631Lumbar pain or ache^a^ 6.13 (1.54)86.53 (0.67)832Breathlessness^a^ 5.88 (1.52)76.22 (1.10)7 Shu (summer heat) syndrome1Thirsty^a^ 7.97 (1.00)87.88 (0.71)82Fever^a^ 7.91 (1.09)88.00 (0.80)83High fever^a^ 7.84 (1.05)87.88 (0.66)84Profuse sweating^a^ 7.81 (1.57)87.53 (0.92)75Surging pulse^a^ 7.66 (0.94)87.66 (0.79)76Fatigue^a^ 7.59 (1.21)77.72 (0.73)77Aversion to heat^a^ 7.56 (1.41)77.72 (0.73)78Reddish yellow urine^a^ 7.56 (0.88)77.47 (0.67)79Red tongue^a^ 7.53 (0.92)67.63 (0.66)610Surging but weak pulse with dipped finger tip^a^ 7.53 (1.02)67.28 (1.02)611Desire to drink^a^ 7.47 (1.41)77.53 (0.67)712Unclear head and eyesight^a^ 7.44 (1.01)77.03 (1.06)713Rapid pulse^a^ 7.34 (1.29)87.28 (0.68)814Heavy or tired limbs^a^ 7.31 (1.38)87.25 (0.84)715Reddened complexion^a^ 7.28 (0.85)77.22 (0.61)716Preference for cold drinks^a^ 7.28 (1.51)77.13 (0.87)717Shortness of urine^a^ 7.22 (1.04)67.06 (0.95)618Red lips^a^ 7.19 (0.74)77.19 (0.64)619Agitation^a^ 7.13 (1.04)77.00 (0.76)720Lethargy^a^ 7.03 (1.26)76.78 (0.87)721Dry tongue with little saliva^a^ 7.00 (0.95)87.09 (0.93)722Anorexia^a^ 6.81 (1.15)86.81 (0.90)823Dizziness^a^ 6.50 (1.22)86.47 (1.08)824Stomach reflux^a^ 6.38 (1.07)76.34 (0.90)725Headache^a^ 6.19 (1.51)76.38 (1.10)7 Shi (dampness) syndrome1Heavy or tired limbs^a^ 8.19 (0.86)78.09 (0.73)72Heavy-headedness^a^ 8.09 (0.86)88.06 (0.76)83Fatigue^a^ 7.81 (0.90)77.81 (0.74)74White and slimy fur^a^ 7.75 (1.05)77.72 (0.68)75Unclear head and eyesight^a^ 7.50 (0.67)87.50 (0.67)86Viscous feeling in oral cavity^a^ 7.50 (0.95)77.47 (0.62)77Thick and slimy fur^a^ 7.47 (1.16)77.63 (0.79)78Soggy pulse^a^ 7.41 (1.34)87.47 (1.02)89Edematous swelling in face and limbs^a^ 7.41 (1.10)77.13 (1.10)710Edema, generalized7.28 (1.53)66.94 (0.95)611Rash7.25 (1.30)66.97 (1.09)612Sloppy stool^a^ 7.22 (1.21)77.38 (0.61)713Slippery pulse^a^ 7.19 (1.06)77.22 (0.79)714Soggy and relaxed pulse^a^ 7.19 (1.35)77.19 (0.90)715White and slippery fur^a^ 7.19 (1.40)67.19 (0.74)6.516No desire to drink^a^ 7.19 (1.23)67.00 (0.88)717Yellow and slimy fur^a^ 7.19 (1.18)76.97 (1.03)718Slippery fur^a^ 7.13 (1.43)77.16 (0.72)719Soft stool^a^ 6.97 (1.36)67.22 (0.61)720Anorexia^a^ 6.97 (1.40)67.22 (0.71)621Dizziness^a^ 6.94 (1.46)77.13 (0.83)722Lethargy^a^ 6.94 (1.34)77.09 (0.89)723White and moist fur^a^ 6.94 (1.32)76.97 (0.78)724Stool with discharge^a^ 6.94 (1.32)76.94 (0.72)725Oppression in chest^a^ 6.91 (1.42)77.13 (0.83)726White and moist fur^a^ 6.91 (1.53)77.13 (0.75)727Not thirsty^a^ 6.91 (1.17)76.97 (0.78)728Soggy and rapid pulse^a^ 6.91 (1.23)76.97 (0.90)729Dyspepsia6.91 (1.42)76.81 (1.00)630Jaundice^a^ 6.91 (1.47)76.78 (1.16)731Mild fever^a^ 6.88 (1.31)77.09 (0.59)732Stomach reflux^a^ 6.78 (1.24)86.84 (0.81)833Gastric stuffiness^a^ 6.75 (1.46)77.06 (0.76)734Vaginal discharge^a^ 6.75 (1.46)87.06(0.76)835A lot of clear and white phlegm^a^ 6.75 (1.34)77.00 (0.51)736Aches and pains in joints^a^ 6.72 (1.35)77.03 (0.47)737White fur^a^ 6.66 (1.49)76.91 (0.78)738Vomiting^a^ 6.59 (1.24)76.56 (0.98)739Ache in limbs^a^ 6.50 (1.32)76.72 (0.58)740Generalized pain^a^ 6.44 (1.48)66.75 (0.50)7 Zao (dryness) syndrome1Dry throat^a^ 8.16 (0.72)88.17 (0.66)82Dry nasal cavity^a^ 8.06 (0.84)77.90 (0.49)63Dry lips^a^ 8.06 (0.88)87.79 (0.49)84Dry skin^a^ 7.84 (0.92)87.83 (0.54)85Dry tongue with little fluid^a^ 7.75 (1.05)87.66 (0.55)86Cough, nonproductive^a^ 756 (1.08)67.62 (0.62)67Thirsty^a^ 7.38 (1.43)87.24 (0.83)7.58Hard bound or dry stool^a^ 7.31 (1.28)77.14 (0.49)79Sticky phlegm^a^ 7.31 (1.03)77.14 (0.52)710Dry, thin and white fur^a^ 7.25 (1.34)77.17 (0.80)711Dry, yellow and white fur^a^ 7.25 (1.16)87.00 (0.89)812Dry and yellow fur^a^ 7.06 (1.29)76.79 (0.73)713Desire to drink^a^ 7.00 (1.37)77.10 (0.86)714Red tongue6.97 (1.58)66.90 (0.62)615Hoarseness^a^ 6.88 (1.21)77.00 (0.53)716Pruritus^a^ 6.81 (1.38)77.10 (0.41)717Dyschezia^a^ 6.50 (1.34)76.59 (0.95)718Cough, productive^a^ 6.28 (1.17)76.59 (0.82)7 Huo (fire) syndrome1High fever^a^ 7.97 (0.82)88.00 (0.57)82Fever^a^ 7.94 (1.08)87.97 (0.54)83Rapid pulse^a^ 7.94 (1.19)87.84 (0.68)84Heat intolerance^a^ 7.91 (0.86)77.94 (0.72)75Thirsty^a^ 7.91 (1.06)77.78 (0.61)76Red tongue^a^ 7.88 (1.01)77.75 (0.67)77Preference for cold drinks^a^ 7.69 (1.00)67.63 (0.66)68Surging pulse^a^ 7.66 (1.18)77.56 (0.72)79Reddish yellow urine^a^ 7.63 (1.01)77.59 (0.56)710Sore throat^a^ 7.56 (1.11)57.69 (0.69)511Reddish eye^a^ 7.56 (1.01)77.56 (0.80)712Desire to drink^a^ 7.56 (1.11)77.53 (0.57)713Reddened complexion^a^ 7.56 (0.84)77.50 (0.72)614Erythema, blister or ulcer^a^ 7.53 (0.72)77.47 (0.98)715Hard bound or dry stool^a^ 7.50 (1.19)77.44 (0.67)716Agitation^a^ 7.50 (1.11)67.38 (0.71)617Red lips^a^ 7.47 (1.02)67.63 (0.71)618Sore swollen gum^a^ 7.47 (1.02)77.44 (0.76)619Dry and yellow fur^a^ 7.44 (0.56)77.47 (0.62)820Hotness in chest^a^ 7.44 (1.01)77.38 (0.55)721Red tip of tongue^a^ 7.44 (1.05)77.38 (0.71)722Red tip and margin of tongue^a^ 7.44 (1.05)77.38 (0.71)723Red dot on tongue^a^ 7.41 (1.07)87.41 (0.67)824Floating and rapid pulse^a^ 7.38 (1.18)77.41 (0.67)725Dry tongue with little fluid^a^ 7.38 (1.01)77.31 (0.64)726Dry, yellow and white fur^a^ 7.38 (0.61)77.28 (0.63)7 Huo (fire) syndrome27Ulcer on tongue^a^ 7.34 (1.26)67.31 (0.74)628Aphtha^a^ 7.34 (1.15)87.28 (0.68)829Hot feeling around anus^a^ 7.31 (1.09)77.28 (1.02)730Dry lips^a^ 7.31 (1.38)77.16 (0.57)731Profuse sweating^a^ 7.31 (1.00)87.06 (0.88)832Purpura^a^ 7.31 (1.28)77.06 (0.76)733String-like and rapid pulse^a^ 7.28 (1.14)87.16 (0.63)734Stinky diarrhea^a^ 7.28 (1.16)76.97 (0.61)735Slippery and rapid pulse^a^ 7.22 (1.16)77.22 (0.61)736Hotness in abdomen^a^ 7.22 (1.21)77.19 (0.54)737Dry throat^a^ 7.22 (1.29)77.16 (0.57)638Decreased urination^a^ 7.22 (1.04)67.09 (0.69)639Dysuria^a^ 7.22 (0.97)76.91 (0.93)740Skin wheal^a^ 7.16 (0.92)87.16 (0.72)841Yellow phlegm^a^ 7.13 (1.24)77.22 (0.55)742Epistaxis^a^ 7.13 (1.36)77.22 (0.66)743Sudden and watery diarrhea^a^ 7.13 (1.01)76.97 (1.12)744Yellow snivel^a^ 7.06 (1.37)87.16 (0.63)745Dyschezia^a^ 7.06 (1.22)6.57.09 (0.64)646Anguish in heart^a^ 7.03 (1.26)7.57.19 (0.64)747Dry nasal cavity^a^ 7.00 (1.30)77.09 (0.53)748Bitter taste in mouth^a^ 7.00 (1.34)77.06 (0.80)749Rash^a^ 6.97 (1.40)77.03 (0.69)750Bloody stool with pus^a^ 6.97 (0.93)76.97 (1.09)751Difficulty falling asleep^a^ 6.94 (1.32)77.09 (0.69)752Delirious speech^a^ 6.84 (1.42)86.72 (0.99)853Gingival bleeding^a^ 6.81 (1.40)76.91 (1.03)754Nasal flaring^a^ 6.75 (1.46)76.81 (1.06)755Difficulty maintaining sleep^a^ 6.72 (1.30)76.91 (0.59)756Hemoptysis^a^ 6.69 (1.40)76.84 (0.85)757Hematuria^a^ 6.69 (1.49)76.66 (1.10)758Headache^a^ 6.56 (1.32)86.41 (0.87)759Hematemesis^a^ 6.44 (1.26)86.44 (0.94)860Breathless^a^ 6.34 (1.26)7.56.13 (0.94)761Lethargy^a^ 6.31 (1.60)76.31 (1.12)762Tinnitus^a^ 5.84 (1.65)75.94 (0.91)7The translations were mainly according to “WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region [70]” SD standard deviation ^a^The 178 diagnostic items graded as 7.0 and above
The total number of retained items in each of the Liu Yin (six excesses) syndromes varied from 15 items in Feng (wind) syndrome to 62 items in Huo (fire) syndrome. All syndromes comprised two kinds of diagnostic items: subjective discomfort factors and objective examinations by the patients themselves or by clinicians. The diagnostic items for subjective discomfort included the following: items regarding sleeping, appetite, eyesight, and hearing; items regarding behavioral adjustments such as aversion, preference, anguish, and agitation; items regarding sensations of coldness, hotness, dryness, and bitterness; and items regarding feelings of pain, itch, ache, congestion, thirst, viscousness, oppression, fullness, stuffiness, heaviness, and tiredness. The diagnostic items for objective examinations included the following: general symptoms regarding complexion, eyes, lips, tongue, skin, snivel, stool, urine, phlegm, and awareness; physical responses such as breathlessness, coughing, shivering, sweating, sneezing, and vomiting; and appearance changes such as hemiplegia, deviated eyes and mouth, opisthotonos, trismus, and edema. In addition to the two kinds of diagnostic items, 4, 2, 3, 4, and 5 items of pulse examination were retained in Feng (wind), Han (coldness), Shu (summer heat), Shi (dampness), and Huo (fire) syndromes, respectively.
Some items were retained in more than one syndrome because of their overlapping contributions, as follows: “headache”, “generalized pain”, “clear snivel”, and “headache and painful stiffness in nape” in Feng (wind) and Han (coldness) syndromes; “floating and rapid pulse” in Feng (wind) and Huo (fire) syndromes; “aches and pains in joints” and “a lot of clear and white phlegm” in Han (coldness) and Shi (dampness) syndromes; “fatigue”, “heavy or tired limbs”, and “unclear head and eyesight” in Shu (summer heat) and Shi (dampness) syndromes; “thirsty”, “desire to drink”, and “dry tongue with little saliva” in Shu (summer heat), Zao (dryness), and Huo (fire) syndromes; “dry nasal cavity”, “dry lips”, “dry throat”, “hard bound or dry stool”, and “dry, yellow and white fur” in Zao (dryness) and Huo (fire) syndromes; and “aversion to heat”, “fever”, “high fever”, “profuse sweating”, “red lips”, “preference for cold drinks”, “agitation”, “shortness of urine”, “reddish yellow urine”, “red tongue”, “surging pulse”, and “rapid pulse” in Shu (summer heat) and Huo (fire) syndromes. Including these overlapping items, the SEED scale for infectious diseases, which captured the Liu Yin (six excesses) syndromes, was created and formatted as follows: Feng (wind), 15 items; Han (coldness), 22 items; Shu (summer heat), 25 items; Shi (dampness), 37 items; Zao (dryness), 17 items; and Huo (fire), 62 items. Following the integration of common items, a total of 102 diagnostic criteria conformed to the Liu Yin (six excesses) and covered the manifestations of the Liu Yin (six excesses) syndromes.
Discussion
This study codified the Liu Yin (six excesses) syndromes by the Delphi method with a panel of 32 CM experts. The 178 diagnostic items derived from the two-stage Delphi method combined information gleaned from CM classic textbooks, journal articles, and opinions of CM experts. All six syndromes encompassed diagnostic criteria regarding subjective discomfort and objective examinations, both were deemed essential for diagnostic judgment. Subjective discomfort was important for medical care considerations, while objective examinations were crucial for disease progress evaluations.
Common diagnostic items were present in different syndromes as a result of the same body responses to different Yin (excess). For example, “generalized pain” in Feng (wind) and Shi (dampness) syndromes results from obstructed circulation of Qi and Xue (blood) [65]. Common items combined with different signs or symptoms imply different body responses [66, 67]. “Fatigue” combined with “thirsty” was attributed to Shu Xie (summer heat excess), while “fatigue” combined with “not thirsty” was attributed to Shi Xie (dampness excess).
Five syndromes, except for Feng (wind) syndrome, comprised diagnostic items of tongue examinations for detecting the Qi and Xue (blood) status. Five syndromes, except for Zao (dryness) syndrome, comprised pulse examinations for instant diagnostic judgment in CM practice [68]. Clinical skills in pulse and tongue examinations were important for accurate assessment of signs and symptoms in the SEED scale [69], just as in CM clinical practice.
The 102 diagnostic criteria were checked by inquiry, inspection, olfaction, audition, percussion, palpation, and pulse examination to ensure complete consideration in medical care. Arrangement of these diagnostic items in a more systematic manner along with a designed record format for tongue and pulse examinations would be necessary for clinical practice. Practice manuals proposing the definition, description, and standardized process for each diagnostic criterion have also been developed for correct implementation.
The limitation of homogeneous education backgrounds is inevitable, since we excluded CM clinicians who had only practicing experience, but no postgraduate degrees from participating in the Delphi panel, as some research background would be required for understanding of the Delphi method and the statistical results circulated during the processes. The panelists’ average practicing experience of 11.7 years was considered to be a good representation of their clinical experience.
Because the Liu Yin (six excesses) syndromes were general categories, exploratory and confirmatory factor analyses were conducted to derive and validate the underlying structures of the SEED scale and to reveal the correlations among signs and symptoms. Future studies, including clinical observations to avoid item redundancy and to confirm the clinical practice of the SEED scale in infectious diseases, are required.
It’s the first scale based on the six excesses (Liu Yin) and constructed by the Delphi method; the CM experts epitomized the contents of CM literature and journal articles via the process. Future applications of the SEED scale in clinical practice, research and CM education are expected.
Conclusion
A CM-based SEED scale was developed for the evaluation and diagnosis of infectious diseases based on only signs and symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic Influenza Clinical aspects of pandemic 2009 influenza A (H 1N 1) virus infection N Engl J Med 2010362181708171910.1056/NEJ Mra 100044920445182 · doi ↗ · pubmed ↗
- 2Miller E Hoschler K Hardelid P Stanford E Andrews N Zambon M Incidence of 2009 pandemic influenza A H 1N 1 infection in England: a cross-sectional serological study Lancet 201037597201100110810.1016/S 0140-6736(09)62126-720096450 · doi ↗ · pubmed ↗
- 3Baden LR Drazen JM Kritek PA Curfman GD Morrissey S Campion EWH 1N 1 Influenza A disease—information for health professionals N Engl J Med 2009360252666266710.1056/NEJ Me 090399219423873 · doi ↗ · pubmed ↗
- 4Echevarría-Zuno S Mejía-AranguréJM Mar-Obeso AJ Grajales-Muñiz C Robles-Pérez E González-León M Infection and death from influenza A H 1N 1 virus in Mexico: a retrospective analysis The Lancet 200937497072072207910.1016/S 0140-6736(09)61638-X 19913290 · doi ↗ · pubmed ↗
- 5Gambotto A Barratt-Boyes S Mde Jong MD Neumann G Kawaoka Y Human infection with highly pathogenic H 5N 1 influenza virus Lancet 200837196221464147510.1016/S 0140-6736(08)60627-318440429 · doi ↗ · pubmed ↗
- 6Webster RG Govorkova EAH 5N 1 influenza-continuing evolution and spread N Engl J Med 2006355212174217710.1056/NEJ Mp 06820517124014 · doi ↗ · pubmed ↗
- 7Blyth CC Iredell JR Dwyer DE Rapid-test sensitivity for novel swine-origin influenza A (H 1N 1) virus in humans N Engl J Med 200936125249310.1056/NEJ Mc 090904919923563 · doi ↗ · pubmed ↗
- 8Oner AF Bay A Arslan S Akdeniz H Sahin HA Cesur Y Avian influenza A (H 5N 1) infection in eastern Turkey in 2006 N Engl J Med 2006355212179218510.1056/NEJ Moa 06060117124015 · doi ↗ · pubmed ↗