An action research approach to facilitating the adoption of a foot health assessment tool in India
Michael Harrison-Blount, Michelle Cullen, Christopher J. Nester, Anita E. Williams

TL;DR
This paper describes the development of a locally adapted foot health assessment tool in India to better address diabetes-related foot problems.
Contribution
The study introduces a locally developed and culturally appropriate foot health assessment tool called SIFT for the Indian context.
Findings
A locally developed foot health assessment tool (SIFT) was created through an action research approach.
The SIFT tool integrates evidence-based guidelines with local cultural and professional needs.
A training program was delivered to support the implementation of the SIFT in clinical practice.
Abstract
India has a diabetes population that is growing and alongside this, the incidence of limb threatening foot problems is increasing. Foot health care provision does not yet meet this demand. In one locality in India, clinicians had an unstructured approach to foot health assessments resulting in poor adoption of evidence based guidelines from the West and a persistence of serious foot complications. There was the perception that existing assessment tools did not take into account the local cultural, organizational and professional needs and there was a lack of ownership of any potential solution to the problem. Therefore, the aim of this work was to facilitate the ownership and development of a foot health assessment tool for use in the Indian context. In order to achieve this an action research approach was chosen. Participants were facilitated through the action and implementation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
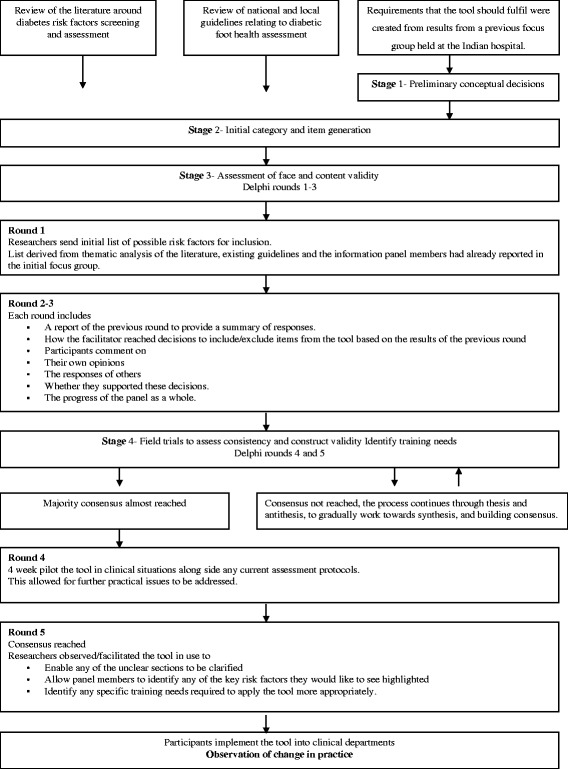 Figure 1
Figure 1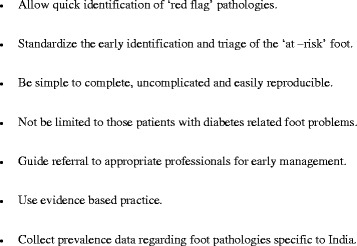 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetic Foot Ulcer Assessment and Management · Delphi Technique in Research · Musculoskeletal pain and rehabilitation
Background
India is second only to China in terms of the size of its diabetes population (65.1 million and 98 million respectively [1]), and incidence is 5.73 % higher than in Europe. The complications of diabetes for the foot are preventable but can only be achieved if the complications are identified early enough and strategies provided in a timely way. With the Indian diabetes population growing it is important to support development of foot health care services by transferring evidence based guidelines from those health care contexts with established experience. However, for this to be effective and have lasting effect, the adoption of best practice must reflect health and social contexts within India and tailored to meet the needs of the local patients and organizations.
Evidence based assessment tools for the identification of foot health complications and their associated risk factors should be the cornerstone of an effective strategy for diabetes foot care in India. However, there are multiple barriers to the implementation of these assessments. It is known that there are insufficient treatment facilities, a lack of structured education programmes and there are cultural and religious influences on behaviors’ related to health. These factors can often explain the late presentation of foot ulcers, walking barefoot, poor footwear, traditional healing techniques and dangerous aesthetic foot treatments [2].
Effective implementation of change in foot care services, such as the use of new assessment tools, requires a tailored approach that is sensitive to the local factors affecting change. Previous work has identified the need to use different approaches, methods and therapeutic strategies in the Eastern (or Indian) context to achieve the goal of transferring evidence based guidelines [3–5]. Furthermore research has explored the need for understanding the values required to successfully embed evidence based practice [6–8]. These values include a clear understanding of the skills and awareness of the person adopting the evidence based practice (the adopter) and the need for ensuring that the research is accessible (the innovation) and matches professional consensus (the organization) [6]. Furthermore that any education provision to support the embedding of evidence based practice must involve active participation of the adopter, with the ultimate aim of increasing knowledge and changing professional behavior [6–8]. Thus, the process through which evidence based guidelines are transferred must embrace these values.
Several authors [6, 9, 10] advise that the characteristics of the specific context, the new knowledge, the clinicians involved and their possible interactions need to be taken into account when implementing change. An action research approach embraces these points and is carried out in collaboration “with” stakeholders within their natural context rather than them being subjects ‘in’ research.
In the first paper of this series [5] researchers used an action research approach to illustrate the importance of process and engagement in driving change and the adoption of evidence based practices by those associated with foot health management in India. The work utilized the problem identification and action-planning phases of the action research process [5] in order to support change in foot care in one locality in India. This was successful in achieving local ownership and identification of the clinicians own problems and, specifically, a desire to develop and implement a foot health screening/assessment tool as a potential solution.
This paper is the second part of the action research approach and uses the need for an agreed foot health assessment tool as an opportunity to facilitate local ownership of health care solutions which have evidence based practices embedded. We use the phases of action, reflection and evaluation required to complete the action research cycle. The aim of this work was to drive consensus among local health care professionals in the details of the foot assessment tool in order to create a locally agreed and owned tool for assessment of foot health status in the Indian context. Aligned with the development of the tool was the need to ensure the adoption of evidence based guidelines, whilst being aware of cultural, organizational and professional needs.
Methods
Approval for the study was obtained from the University of Salford Research, Innovation and Academic Engagement Ethical Approval Panel (Approval number HSCR12-22) and the hospital governance team at a major university hospital situated in Chennai, India.
An action research approach was adopted to ensure that the assessment tool was based on evidence based guidelines [11], whilst being culturally sensitive and applicable to local need. The foundation phase of the action research cycle has been achieved [5] and the focus of this paper is the action, reflection and evaluation phases.
Within the framework of action research processes, a consensus building approach (a modified Delphi technique) was used to facilitate definition of the foot health assessment tool. The participants were facilitated through an iterative process that used five rounds of questions, data collection and analysis techniques interspersed with feedback. It was a process through which ownership was given to the clinicians, with the results being used to define the components of a draft assessment tool that was then checked for face and construct validity. Several authors recommend a staged approach to developing an assessment tool and this was utilized during the process, [12–14].
Stage 1 – Preliminary conceptual decisions
To guide the development process, a list of prerequisites was created from the results of the action planning phase of the action research cycle in which the clinicians had participated and is reported in a previous paper [5]. This list of prerequisites highlights the standards that the participants feel any subsequent tool should achieve. The list can be viewed in the results section.
Stage 2 – Initial category and Item generation
A list of items were presented to participants in Round 1, relating to factors associated with diabetes foot complications, and these were generated from a focused search of the literature that used a thematic framework approach to identify content cross referenced with a review of clinical guidelines. The literature search identified 392 articles, of which 295 were excluded. Sixty one further articles were excluded because they were duplicates, did not report foot related complaints, reported on screening/assessment tools for non-foot related conditions or reported complaints or risk factors not highlighted in best practice guidelines [11]. Thirty-six studies were included in the final qualitative synthesis and were cross-referenced with national and local UK guidelines. This thematic analysis produced a list of 20 risk factors and 40 screening tests/checks for possible inclusion in the assessment tool.
Stage 3 – Assessment of face and content validity
In the context of the diabetic foot, validity refers to the degree to which the assessment measures the risk factors presenting in the lower limb. Face validity is the lowest level of validity and based upon the personal opinions of the observer. Content validity is determined by theoretical reasoning that a foot health assessment tool adequately measures selected foot health variables. When a foot health assessment tool is believed to include the domains that are required to adequately assess the foot its content is considered valid (content validity). We achieved consensus on the items to be included in the tool as well as the phrasing of such items and this process also enhanced the ownership of the assessment tool.
Stage 4 – Field trials to assess consistency and construct validity
The assessment tool created by the clinicians (Salford Indian Foot Health Assessment Tool (SIFT)) was piloted to begin the process of assessing consistency, to achieve construct validity and to allow clinicians to test local implementation of their own solution. This process will continue following completion of the Delphi and will be reported in a follow up paper.
An overview of the Delphi process can be seen in Fig. 1.Fig. 1. The Delphi procedure-overview of the process
Selection of Delphi panel members
The authors recruited to the Delphi panel those participants who had taken part in the first phase of the action research model [5], as it would be these clinicians who would be embedding the evidence base into clinical practice. This provided continuity through the subsequent action and implementation phases. Although not experts in the assessment and triage of foot health, this was not necessary, since they were all experts within their chosen disciplines and in the Indian health care context. This knowledge was the foundation of their role in the Delphi process, since what is ‘evidence based’ in clinical terms was established through the literature and existing guidelines search in the initial category and item generation phases.
The term item is used to mean both the risk factors and tests/assessments used. Previous authors have stated that consensus is reached when a positive response level of 75 % or greater from the participants is reached [12–17].
Round 1
Information about the aim of their participation, the methods used and invitation to be part of the change process was sent to the participants. The researchers sent the initial list of possible risk factors for inclusion in the foot health assessment tool to the participants. This was the list derived from the initial literature search and the information participants had already reported as list of criteria they would deem important in a foot assessment tool from a previous focus group [5]. This provided early ownership of the knowledge to be discussed, free from the influence of peers and the dynamics of group discussions. The aim was to collect information on each participant’s opinion regarding the importance of each risk factor. To help the decision making process the authors also included a summary of the evidence that supported each risk factor. Participants were asked to rate the importance of inclusion of each risk factor using a Likert scale (5 being essential to include and 1 being essential to remove). The authors also gave participants the opportunity to comment on any of the risk factors included in the tool. Responses were accumulated to devise an agreed criteria list, which was then sent out for comments and amendments in round 2.
Round 2
The researchers used the results of round 1 to select risk factors for which there were high levels of agreement for inclusion/exclusion from the final tool. Risk factors that rated as 5 and 4 by at least 75 % (6 participants) were included. Risk factors rated, as 3 by at least 75 % of the members were included in this round to allow for re consideration and those rated as 2 and 1 were excluded.
For round 2 the participants were asked to review the comments or amendments made to the risk factors in round 1 and re-evaluate any of those risks. At this stage panel members were provided with the tests/assessments to be used to evaluate each risk factor and again asked to rate their inclusions on a Likert scale (5 being essential to include and 1 to be removed). Again panel members were given the opportunity to provide comments and additionally participants were asked: Would you like to see a number of key Risk factors highlighted on the final assessment tool? And do you endorse the Delphi procedure so far? If no please give details of the aspects of the procedure which you do not support and list any suggestions you have for improvement. This latter question challenged participants to acknowledge their participation in a group exercise and reaffirm their belief in its progress. This was important to bolster confidence in the process in which they were engaged and to validate their contributions as ‘valued’.
Round 3
The results of round 2 were used to select the final risk factors, tests and assessments for inclusion in the final tool. Risk factors rated 3 at round 2 that had been re-rated as 5 and 4 by at least 75 % of the participants who replied in this round were selected for inclusion in the final tool. Items that remained rated as 3 or had been re-rated as 2 or 1 were excluded.
Tests/assessments that rated as 5 and 4 by at least 75 % of the participants who replied in this round were selected for inclusion in the tool. Tests/assessments rated, as 3 by at least 75 % of the members were included for the next round to allow for re consideration and those rated as 2 and 1 were excluded.
This third round asked the panelists to review the inclusion and exclusion results for both items and to indicate whether they thought that an item should be included or excluded. Participants were also asked to comment on any item that they would like to rephrase or whether they wished to add an item to the tool and to provide suggestions of such changes.
Round 4 (Pilot)
The results of round 3 were used to select any rephrased or additional items to be included in the foot health assessment tool. Risk factors and tests/assessments selected for inclusion at this stage were presented to the participants for them to indicate whether they agreed with the proposed rephrasing or additional items, and if not to suggest alternatives. Risk factors and tests/assessments that rated as 5 and 4 by at least 75 % of the participants who replied in this round were selected for inclusion in the tool. Risk factors and tests/assessments rated as 3 by at least 75 % of the members were included for the next round to allow for re consideration and those rated as 2 and 1 were excluded.
This provided a new level of contribution by participants, such as rewording specific items, and thus provided ownership of the precise details and language used.
The clinicians who had been part of the process were asked to pilot the tool over a 4-week period on patients presenting with foot health problems within their own specific disciplines. This brought to life their own efforts in practical terms, in front of their colleagues and patients, and thus reinforced the productivity of the exercise in which they had participated. They were asked to consider, the practicalities of the risk factors and tests/assessments for suggested inclusion in the final tool, how the test and assessments would be recorded, any further additions they may want to make to the tool and to suggest solutions and alternatives to any comments made. Participants were asked to record their decision using either yes, no or unclear with consensus reached at a level of 75 % agreement as with previous rounds. Additionally participants were asked to record any further items they would like to have considered for inclusion in the tool following the pilot. These were recorded as a list and distributed to the participants.
Round 5 (Visit) modification of the Delphi procedure
This modification allowed the researchers to see the tool being used in a clinical setting in order to influence the development stages thereby improving face validity and overcoming the potential interpretation difficulties. The results of round 4 were used to select the content of the final foot health assessment tool. All current and additional items rated as ‘yes’ by at least 75 % of the participants who replied in this round were selected for inclusion in the final tool. All current and additional items rated as ‘no’ by at least 75 % of the participants who replied in this round were excluded. We considered responses regarding items marked as ‘unclear’ by at least 75 % and asked the respondents to revisit the guidelines for clarification.
In round 5 the final version of the Salford Indian Foot Health Assessment Tool (SIFT) and the guidelines were presented to the panel members for use. The researchers spent one week with participants in order to provide support and to identify any specific training needs.
Results
Eight of the eleven clinicians invited to take part consented to participate in the Delphi procedure. The specialties of the clinicians are listed in Table 1.Table 1. Participants involvement and clinical specialtiesParticipant (P) codeRoleAgreement to take part in the processP1Consultant General Physician (Head of service)AgreedP2Consultant General PhysicianRequested not to take partP3Consultant DermatologistAgreedP4Orthopaedic surgeon (Lead member of staff, key contact)AgreedP5General surgeon (Head of service)AgreedP6Consultant Sports MedicineAgreedP7Consultant Diabetologist (Lead member of staff, key contact)AgreedP8Head of PhysiotherapyAgreedP9Head orthotistAgreedP10Consultant Vascular Surgeon (Head of service)Requested not to take partP11Consultant endocrinologist (Head of service)Requested not to take part
Preliminary conceptual decisions
The researchers and participants of the focus group in the problem identification and action planning stages decided that the foot health assessment tool should have the following prerequisites (Fig. 2).Fig. 2. List of prerequisites to be met by a foot health assessment tool designed for this locality
Delphi rounds 1–3: Assessment of face and content validity
The result of this study was the design of a foot health assessment tool (SIFT) developed by those who would use it in clinical practice. This was achieved using a modified Delphi method embedded in an action research process, which aims to facilitate change through ownership.
Delphi Round 1
All eight of the participants who agreed to take part in the procedure returned completed questionnaires. Following the results of this round, ten risk factors were selected for inclusion, eight risk factors were removed from the tool as they were rerated at 1 or 2 on the likert scale by >75 % of the participants and 2 risk factors were put forward to be rerated as part of round 2 (Table 2).Table 2. Delphi results: Round 1Original 20 risk factors identified for possible inclusion% expert acceptanceLikert ratingFeedback put forward for round 2Infection1004-5To be includedIschemia100Neuropathy88Ulceration current88Deformity88Dermatological75Amputation88Smoking100Footwear88Charcot88Vascular surgery883To be reratedUlceration previous88Trauma751–2To be excluded from processEducation88Age socioeconomic100Plantar pressures88Self care88Retinopathy/visual impairment100Nephropathy88Glycaemia88
Delphi round 2
Of the eight practitioners involved with the process seven returned completed questionnaires. The eighth member of the panel had reported being too busy this time to take part, but still wished to be part of further rounds.
Following the results of this round, the ten risk factors selected for inclusion were not challenged and would therefore be included in the final tool. The eight risk factors removed from the tool were all agreed and therefore excluded from the process. The two risk factors where consensus had not been reached had been rerated, one to be included in the final tool and the other to be amended, and then added to the final tool (Table 3).Table 3. Delphi results: Round 2 Consensus for risk factors and tests/assessmentsRound 2 consensus for risk factorsRound 2 consensus for tests/assessmentsRisk factors confirmed for inclusion in the final tool% expert acceptanceLikert ratingComments or amendments on previous roundOriginal list of Tests/assessments for possible inclusion% expert acceptanceLikert ratingFeedback put forward for round 3Infection1004–5Not challengedVisual assessment of Redness, warmth, Pus, odor, swelling1004–5To be includedIschemia100DP/TP pulses1004–5To be includedTemp touch86ABPI861–2To be excludedDoppler86CRT86TBI100Duplex100TcPO2100Neuropathy100Monofilament1004–5To be includedTuning fork100Vibratip1001–2To be excludedIpswitch touch test100Ankle reflex100Neurotip86Biothesiometer100Ulceration current100Yes/no1004–5To be includedDeformity100Charcot1004–5To be includedClaw/hammer toes1003To be reratedHAV86Flat foot100Prom Met heads100Dermatological100Corns and Callus864–5To be includedDry86Cracked100Fungal86Blisters100Extravasation tissue86Maceration86Nail problems863To be reratedAtrophy861–2To be excludedAmputation100Yes/no1004–5To be includedSmoking100Yes/no1004–5To be includedFootwear100Style1004–5To be includedToe box1003To be reratedWear100Insoles100Fit100Condition86Charcot100Visual assessment of redness, unilateral temp difference, swelling1004–5To be includedVascular surgery864–5Vascular surgery altered to Significant surgical historyYes/no1004–5To be includedUlceration previous86IncludedYes/no1004–5To be includedTrauma861–2Not challengedEducation86Age socioeconomic100Plantar pressures86Self care86Retinopathy/visual impairment100Nephropathy86Glycaemia86
The results following this round found that 5 risk factors would be assessed by a yes or no option, fifteen further tests/methods of assessment were selected for inclusion, fourteen tests/assessment methods were removed from the tool, including two that had not been sent to participants as the risk factor they assessed had already been excluded in a previous round. Ten tests/assessment methods were put forward to be rerated in round 3 (Table 3).
In this round six of the seven participants were in favor of seeing a number of key risk factors highlighted on the final assessment tool. The member of the panel who stated they were ‘unclear’ about highlighting certain risk factors went on to explain that they felt this could only be done if ’it did not over complicate the tool and make it difficult for all staff to use and make sense of’ as the majority of members were in favor of this, the researchers decided to investigate highlighting the risk factors in round five during observation of its use in practice. At this stage all seven of the panel members reported that they endorsed the Delphi procedure so far and were happy to continue with the process.
Delphi round 3
All eight of the practitioners involved with the process returned completed questionnaires.
Following the results of this round the twenty tests/assessment methods selected for inclusion were not challenged and would therefore is included in the final tool. The twelve tests/assessment methods removed from the tool were all agreed and therefore excluded from the process. Of the ten tests/assessment methods where consensus had not been reached and had been rerated, one was included into the final assessment tool and the remaining nine were excluded from the process (Table 4).Table 4. Delphi results: Round 3Original 20 tests/assessments identified for possible inclusion% expert acceptanceLikert ratingComments or amendments on previous roundInfection - Visual assessment1004–5Not challenged and therefore includedDP/TP pulses100Temp touch100Monofilament100Tuning fork100Ulceration current – yes/no100Ulceration previous – yes no100Deformity – Charcot100Corns and Callus100Dry100Cracked100Fungal100Blisters100Extravasation tissue100Maceration100Amputation – yes/no100Smoking – yes/no100Footwear - style100Charcot - Visual assessment100Significant Surgical History– yes/no100Nail problems884–5IncludedABPI881–2Not challenged and therefore excluded from the processDoppler75CRT88TBI100Duplex100TcPO2100Vibratip100Ipswitch touch test100Ankle reflex100Neurotip88Biothesiometer100Atrophy100
The additional results in this round report those items that the panel wished to rephrase or add. During this round no additional risk factors were added, four risk factors were rephrased, one was subdivided into two, and four were categorized under one of the other existing risk factors and therefore were moved into the tests/assessment methods section. In addition twelve further test/methods of assessment were added, two of which had further subdivisions, four were rephrased and three were subdivided (Table 5).Table 5. Delphi results: Round 3Risk factors put forward for rephrasing or subdivisionSuggested rephrasing or subdivisionTests/assessments put forward for rephrasing recategorizing or subdivisionSuggested rephrasing, recategorizing or subdivisionSuggested tests/assessments to be added to current listInfectionCellulitisVisual assessment of Redness, warmth, Pus, odor, swellingYes/no Move to skin conditionsDeformityAmputationForefootRear footOtherIschemiaPeripheral vascular assessmentDP/TP pulsesPalpable - Yes/noIntermittent claudicationOedemaRest painTemp touchNormal /AbnormalNeuropathyNeurological assessmentMonofilament10 sites for monofilamentTuning forkHypo pigmented skin lesionsUlceration currentYes/noMove to skin conditionsUlceration previousYes/noDermatologicalSkin conditionsMacerationHyperhydroticNormalDryHypohydroticInterdigital rashCrackedFissureCellulitisNail conditionsonychauxisonychomycosisparonychiaonychocryptosisotherAmputationYes/noMove to deformityFootwearStyleTypeHabitsWorn alwaysOutdoors onlyneverIndoors onlyCharcotVisual assessment of Redness, unilateral temp difference, swellingYes/no Move to deformity
Panel members were also asked in this round if they agreed with the procedure of being asked whether they would support the instructions issued in round 4 and whether they would be willing to comment on any changes. All eight panel members agreed to this process.
Delphi rounds 4 & 5: Field trials to assess consistency and construct validity
Field trials to assess consistency and construct validity are ongoing, as at this stage we have not undertaken any formal quantitative analysis. The first stages of the validation process have begun by piloting the tool in clinical practice.
Delphi round 4
All eight of the practitioners involved with the process returned completed questionnaires and took part in the pilot of the tool over a four week period, on patients presenting with foot health problems within their own specific disciplines, where they were asked to consider the practicalities of the tool in a clinical setting.
Following the results of the completed questionnaires the eight risk factors chosen and where rephrased were not challenged and therefore included in the pilot tool. Of the thirty one tests/assessment methods chosen, none of the rephrased or additional items were challenged and therefore included in the pilot tool. No alternatives were suggested for any of the current items (Table 6).Table 6. Delphi results – Round four consensus on rephrased items and additional tests/assessmentsRound four consensus on rephrased itemsRound four consensus on additional assessments/testsRisk factors for inclusionSuggested risk factors to be rephrased or subdivided% expert consensusTests/assessments for inclusionSuggested tests/assessments to be rephrased or subdivided% expert consensusSuggested tests assessments to be added% expert consensusInfectionCellulitis100Visual assessment of Redness, warmth, Pus, odor, swellingYes/no Move to skin conditions100IschemiaPeripheral vascular assessment100DP/TP pulsesPalpable - Yes/no100Intermittent claudication100Temp touchNormal/Abnormal100Oedema100Rest pain86DeformityAmputation100Forefoot75Rear foot75Other75NeuropathyNeurological assessment100Monofilament10 sites for monofilament86Tuning forkHypo pigmented skin lesions100Ulceration currentYes/noMove to skin conditions86Ulceration previousYes/noDermatologicalSkin conditions86MacerationHyperhydrotic100Normal100DryHypohydrotic100Interdigital rash75CrackedFissure75Cellulitis86Nail conditionsonychauxis75onychomycosis75paronychia75onychocryptosis75other75AmputationYes/noMove to deformity100FootwearStyleType100Habits86Worn always100Outdoors only100never100Indoors only100CharcotVisual assessment of redness, unilateral temp difference, swellingYes/no Move to deformity100
All of the proposed risk factors were marked ‘yes’ by the panelists in response to the question of practicality. Panelists marked 3 methods of recording risk factors as ‘No’ and 1 was marked as unclear. It was felt by the panelists that previous amputation should be recorded as a yes/no followed by the site and whether it was traumatic, surgical or auto amputation. It was further felt that the recording of skin and nail conditions should also be done by circling yes or no, and that location of lesions should be recorded on pictures of both a left and right foot. Other lesions to be recorded here include amputations and current ulcers. Smoking was marked as unclear by 6 (75 %) of the panelists as they felt that this was not specific enough due to the differing methods of tobacco use in India which include smoking, chewing and snuff (Table 7).Table 7. Delphi results: Round 4-Pilot of the toolRisk factors confirmed for inclusion in the Pilot toolPracticality of proposed risk factor% expert consensusTests and assessment methods confirmed for inclusion in the Pilot toolMethod of recording tests and assessment methodsPracticality of proposed test/assessment and method of recording% expert consensusPeripheral vascular assessmentYes100DP/TP pulses palpableYes/noYes100Temp touchNormal/AbnormalYes100Intermittent claudicationYes/noYes100Oedema PresentYes/noYes100Rest painYes/noYes100Neurological assessmentYes100Monofilament10 sites Hypopigmented skin lesionsYes86VibrationLeft/Right Normal/Absent/reducedYes100DeformityYes100CharcotYes/noYes100AmputationSite and Surgical/traumatic/autoNo75ForefootSpecific toe/site Left and rightYes100Rear footFoot posture RCSP Normal/pronated/supinatedYes75Skin conditionsYes100FungalTick boxNo75CellulitisState siteCurrent ulcerLeft or right footPrevious ulcerFor Other state conditionNormalInterdigital rashHyperhydroticHypohydroticFissureCorns and CallusExtravasation tissueBlistersOtherNail conditionsYes100OnychauxisTick box State siteNo100OnychomycosisLeft or right footParonychiaFor Other state conditionOnychocryptosisOtherSmokingYes100Yes/noUnclear75FootwearYes100TypeTick boxYes100State TypeHabitsWorn alwaysYes100Outdoors onlyIndoors onlyNeverSignificant Surgical HistoryYes100Location, DetailsYes100
The panelists also suggested that a number of sections be added to the final assessment tool which had not been considered until the tool had been used in practice (Table 8).Table 8. Delphi results: Round 4-Additional suggested items to be added to final toolProposed additions to the assessment toolFurther detailsSocial to be added to the demographics sectionThis will include smoking and additionally alcohol due to the high reported incidence of alcoholism by the panel membersFilarial to the medical history sectionPatient complains of (in relation to the foot condition)To record patients chief complaintClassification and stage of diabetic footTo aid putting patients onto the correct management planManagement planThis would includeInitial Return periodNext screeningTreatment (interventions to circle)Referral (departments to circle)As a quick reference to past treatmentsDiagnosis/summaryA small section at the end of the tool to allow some notes to be written about the patients diagnosis
At this stage all eight of the panel members reported that they endorsed the Delphi procedure following a review of the aims and purpose. Additionally all eight panel members reported use of the evidence provided and the feedback from the previous rounds. Two members stated that although they had read the evidence initially they used the feedback predominantly to inform and support their decisions as the evidence document took time to read in what were already busy clinics for them to manage.
Delphi round 5
All eight of the practitioners involved with the process agreed to being observed using the tool within their own departments.
At this stage the panel members used the tool and the researchers observed it in use for one week within the hospital. All panel members agreed on the alterations to the way in which amputations, skin and nail conditions were recorded via a yes/no structure and the recording of the sites of the skin and nail conditions onto pictures. No panel members recorded any items as ‘unclear’ (Table 9). Six of the items proposed for additional inclusion were accepted by all of the panel members and therefore added to the final tool. The item Diagnosis/summary however was felt by seven members of the panel (88 %) to be unnecessary. It was argued that as the tool collects multiple pieces of data it would also produce many possible diagnoses, which would be, prioritized differently depending on the specialist using the tool. It was further expressed that this was not required as the additional classification category provided enough information about risk, to guide the management steps appropriately. The diagnosis/summary section was therefore excluded from the final tool (Table 10).Table 9. Delphi results: Round 5-Alterations to methods of recordingRisk factors confirmed for inclusion in the Pilot toolTests and assessment methods confirmed for inclusion in the Pilot toolMethod of recording tests and assessment methodsPracticality of proposed test/assessment and method of recordingSuggested alternative% expert consensusComments or amendments on previous roundAmputationSite and Surgical/traumatic/autoNoYes/no + recorded on foot picture100Not challenged and therefore includedSkin conditionsFungalTick boxNoYes/no + recorded on foot picture100State siteCellulitisLeft or right footCurrent ulcerFor Other state conditionPrevious ulcerNormalInterdigital rashHyperhydroticHypohydroticFissureCorns and CallusExtravasation tissueBlistersOtherNail conditionsOnychauxisTick boxNoYes/no + recorded on foot picture100OnychomycosisState siteParonychiaLeft or right footOnychocryptosisFor Other state conditionOtherSmokingYes/noUnclearInclude smoking, snuff, Chewing100Table 10Delphi results: Round 5-Additional items to be added to final toolProposed additions to the assessment toolFurther detailsAcceptance of additional item% expert consensusComments or amendments on previous roundSocial to be added to the demographics sectionThis will include smoking and additionally alcohol due to the high reported incidence of alcoholism by the panel membersYes100Not challenged and therefore includedFilarial to the medical history sectionYes100Patient complains of (in relation to the foot condition)To record patients chief complaintYes100Classification and stage of diabetic footTo aid putting patients onto the correct management planYes100Management planThis would includeYes88Initial Return periodNext screeningTreatment (interventions to circle)Referral (departments to circle)As a quick reference to past treatmentsDiagnosis/summaryA small section at the end of the tool to allow some notes to be written about the patients diagnosisNo88Not challenged and therefore excluded
The tool is structured as a list of thirteen sections made up of the risk factors identified during this investigation. Each of those sections contains subsections made up of the relevant tests, assessment methods and visual checks used to identify foot pathologies. The participants agreed that the following items (Table 11) were to be highlighted as ‘red flags’ and should therefore alert a rapid referral to the appropriate department. Participants requested that these items were highlighted on the tool with a capital letter R. The final tool is presented in Additional file 1. The clinical content of tool itself is not greatly dissimilar to foot health assessment tools developed in the West, this however is not surprising as the guidelines on which SIFT was based were mostly developed in the West. More importantly the opportunity for the clinicians to be participatory in the process has developed a tool where the structure and format are born out of the Indian health care system and subsequent adoption has taken place as a result of the participation in its development. A more detailed description of each section together with the corresponding evidence base were issued to the participants to support implementation and to act as a reference once the researchers had withdrawn from the location on completion. The guidelines and use of the tool in round 5 identified possible training needs for the participants and potentially for others who may also wish to use the tool at this site. Therefore in conjunction with the guidelines the researchers also developed and delivered a short foot health assessment and management training program entitled ‘Principles of lower limb assessment and management’ (Additional file 2). The SIFT was subsequently adopted by the hospital and used in practice. To date the tool has been used 2,622 times.Table 11. Items to be highlighted as red flags in final toolMedical conditionsDiabetesLeprosyBuergers diseasePVDVenous insufficiencyRheumatoid arthritis/SLEFilarialSkin conditionsCurrent UlcerPrevious UlcerCellulitisDeformityCharcotPrevious amputationPVDICRest painNeurological systemLess than 8 sitesHypo pigmented lesions
Discussion
Through the action research approach researchers facilitated the process whereby clinicians took local ownership of a clinical problem, developed their own solution i.e. the Salford Indian Foot health assessment Tool (SIFT) and embedded it into their practice. Through this approach researchers identified the knowledge and skills of the adopters, made the research evidence accessible and using Delphi ensured the adopters actively participated in reaching professional consensus on how that research evidence was embraced and embedded into practice [18]. This is the first time an action research approach has been used to drive change in Indian foot health care services
The Delphi process has been a useful method for both data collection and to achieve consensus with the participants [19, 20]. Delphi was employed as a tool embedded within the ethos of action research. Active participation of the adopters in this process has proven to be effective as a vehicle to embed evidence into practice, facilitate ownership of the solutions thereby sustaining change within their clinical practice [21].
It is generally considered that the Delphi technique requires ‘experts’ to be the participants, however, it can still be used where no experts exist [23]. In the west, podiatrists are considered the experts in the care of foot problems [3, 11] but in India there are no locally trained podiatrists within its healthcare system. However, although the participants were not experts in the area of foot health assessment they were experts in how foot health problems present in their clinics and in India on a daily basis. Critically, it was this expertise, not expertise in best practice of foot health, that was needed to drive creation of shared solutions for the foot assessment tool [22–25].
The Delphi has the further advantage of offering anonymity [26]. This helped prevent domination of some over others due to caste, gender, authority or personality. It is recognized that this culture and environment may influence the success of a change management process [27].
According to the institutional theory [27], the institutional environment can be defined by its structure and culture. Hofstede [28] identifies ‘power distance’ (PDI) as the extent to which the less powerful members of institutions accept and expect that power be distributed unequally, in this context it is the caste system [29]. Hofstede [28] also identified that gender inequality influences the culture of an institution and in India the male gender is viewed as superior with the role of decision makers [30, 31, 32]. Hence, we considered the anonymity of the Delphi method would overcome some of these influences in order to achieve completion of the action research cycle.
There are limitations to the use of the Delphi method [33]. There is no reported standard for the size and selection of panel members, with studies using a range of 4–171 experts, [34–36]. Further, there is no “typical” Delphi method, rather that the method is modified to suit the context and the research question. Additionally, there is no evidence of reliability of the method and as a result it cannot be certain that if the same task were given to two or more different panels, would the same results be obtained. Furthermore the lack of opportunity to clarify responses can create interpretation difficulties for both the researchers and participants [37], especially when working with participants whose first language is not English. The Delphi method has been used successfully to develop data collection tools previously [38–43] but to date, this is the first time that a delphi has been used within an action research approach to bring about local ownership of a clinical problem and produce a solution which was the development of the Salford Indian Foot health assessment.
However, the SIFT is not without its limitations and clearly focuses on the medical and podiatric presentations of patients following a biomedical model of health care. Although it collects some data in relation to alcohol, tobacco use and footwear practices, the wider bio psychosocial aspects [44, 45] are absent. It is important to handle the three together, as literature suggests that patient perceptions of health, threat of disease and barriers to good health in a patient's social or cultural environment influences the likelihood that they will engage in good health behaviors [46]. The dominance of the biomedical model may reflect wider cultural approaches to health care.
Use of the tool in clinical practice to assess consistency and construct validity are ongoing, as at this stage we have not undertaken any formal quantitative analysis of the SIFT. However, the first stages of the validation process have included a pilot of the tool in clinical practice. This has shown variation among some clinicians where there is subjectivity in the assessment decision which is similar to what Thompson et al. 2004 found. [47]. The pilot also identified that there was a training need for objective clinical testing. The use of ‘objective’ diagnostic equipment has been shown to reduce variability in the conduct of clinical tests [48–50]. It has also been reported that the opportunity to make modifications based upon reflections in practice can be useful in improving validity and reliability when generalists use structured screening tools [51]. Further testing is required to measure the reliability of the instrument and thereby determine the degree of consistency between the scores obtained at two or more independent times of testing by measuring inter rater reliability [52].
The participants reflected on the final tool and it components and this highlighted the need for training to support its use [53, 54]. Hence, as well as the tool being the vehicle for assessing foot health, it aided identification of training needs in foot health assessment and management including an increased awareness of the importance of simple lesions, the importance of regular screening including vascular, neurological, wound and offloading principles in the high risk foot. Further, the participants identified a need for sustainable training [55] and to meet this requirement a ‘train the trainer’ programme was delivered. The combination of the action research approach to develop the SIFT and the training programme aligned with the recommendation for multiple strategies to achieve improved knowledge and change in behavior made by Halfens and van Linge (2003) [6] and when combined with the education of the local ‘opinion leader’, both the need and the process of change was optimized [56, 57].
This research has facilitated the action research cycle that initially identified the need for change [5]. Through the phases of action and implementation the authors have facilitated the development of a locally defined, context specific assessment tool to aid identification of foot problems and hence the implementation of appropriate and timely management for individual patients. Further, the information gathered from this tool can be used to identify areas for service improvement.
Conclusion
The action research process has given local ownership of the solution to practitioners and produced the first systematically developed evidence based foot health assessment tool to be used in India. The first step identified by the participating practitioners [5], as being pivotal to achieving better outcomes for patients. Engagement in the action research process has given practitioners the opportunity to reflect on current practice and bring about change within their service and individual clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Diabetes Federation, IDF Diabetes Atlas 6th ed. 2013, Retrieved from http://www.idf.org/diabetesatlas.
- 2Bakker K Abbas ZG Pendsey S Step by Step, improving diabetic foot care in the developing world. A pilot study for India, Bangladesh, Sri Lanka and Tanzania Practical Diabetes Int 200623365910.1002/pdi.1012 · doi ↗
- 3Apelqvist J Diabetic foot ulcers: evidence, cost and management The diabetic Foot J 20071068
- 4Harrison-Blount M, Cullen M, Nester CJ, Williams AE. The assessment and management of diabetes related lower limb problems in India-an action research approach to integrating best practice. Journal of foot and ankle research., 2014. doi:10.1186/1757-1146-7-30.10.1186/1757-1146-7-30PMC 403238624862010 · doi ↗ · pubmed ↗
- 5Halfens R Van Linghe R Dissemination and implementation of knowledge. State of the art studies 2003 The Netherlands LEVV
- 6Funk G Champagne MT Wiese RA Tornquist EM Barriers to using research findings in practice. The clinician’s perspective Applied Nursing Res 199142909510.1016/S 0897-1897(05)80062-X 1741642 · doi ↗ · pubmed ↗
- 7Kitson A Harvey G Mc Cormack B Enabling the implementation of evidence based practice: a conceptual framework Quality in Health Care 1998714915810.1136/qshc.7.3.14910185141 PMC 2483604 · doi ↗ · pubmed ↗
- 8Denis JL Hebert Y Langley A Lozeau D Trottier LH Explaining diffusion patterns for complex health care innovations Health Care Management Re- view 2002273607310.1097/00004010-200207000-0000712146784 · doi ↗ · pubmed ↗