Sex Differences in Dose Escalation and Overdose Death during Chronic Opioid Therapy: A Population-Based Cohort Study
Eric Kaplovitch, Tara Gomes, Ximena Camacho, Irfan A. Dhalla, Muhammad M. Mamdani, David N. Juurlink

TL;DR
Men are more likely than women to escalate to high-dose opioid therapy and die from opioid-related causes during chronic treatment for noncancer pain.
Contribution
This study identifies sex differences in opioid dose escalation and overdose mortality in a large population-based cohort.
Findings
Men were 44% more likely than women to escalate to high-dose opioid therapy.
Men were twice as likely as women to die from opioid-related causes.
The findings were consistent in a broader analysis of over 285,000 individuals receiving any opioid.
Abstract
The use of opioids for noncancer pain is widespread, and more than 16,000 die of opioid-related causes in the United States annually. The patients at greatest risk of death are those receiving high doses of opioids. Whether sex influences the risk of dose escalation or opioid-related mortality is unknown. We conducted a cohort study using healthcare records of 32,499 individuals aged 15 to 64 who commenced chronic opioid therapy for noncancer pain between April 1, 1997 and December 31, 2010 in Ontario, Canada. Patients were followed from their first opioid prescription until discontinuation of therapy, death from any cause or the end of the study period. Among patients receiving chronic opioid therapy, 589 (1.8%) escalated to high dose therapy and n = 59 (0.2%) died of opioid-related causes while on treatment. After multivariable adjustment, men were more likely than women to escalate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
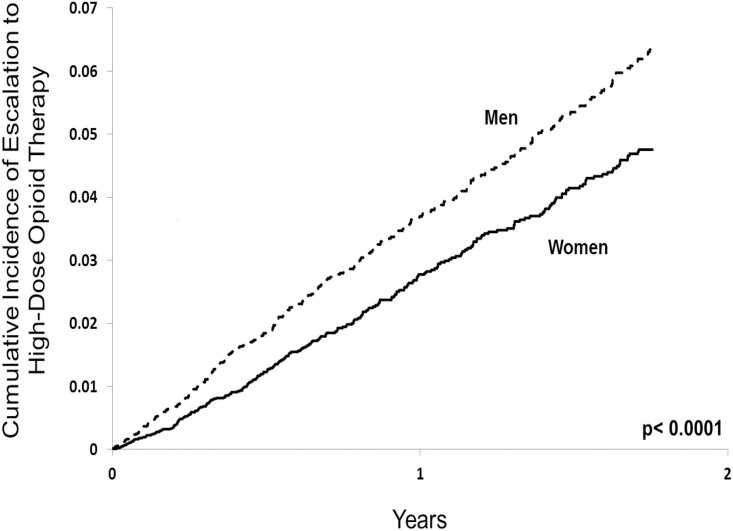 Fig 1
Fig 1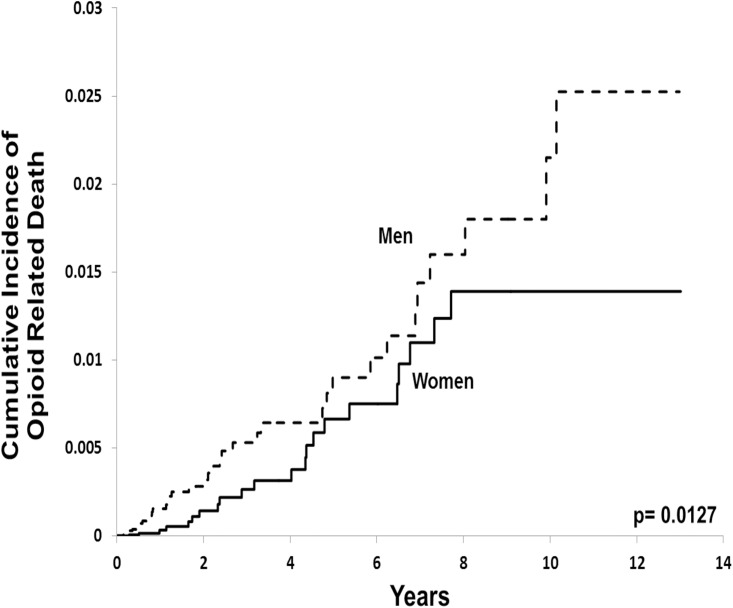 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOpioid Use Disorder Treatment · Opioid Use Disorder Treatment · Pain Management and Opioid Use
Introduction
Over the past twenty years, the use of opioids for chronic noncancer pain has increased markedly in North America [1,2,3,4,5], with patients often receiving doses far in excess of those originally suggested for treatment [6]. The increasing use of opioids has been paralleled by a dramatic rise in opioid-related mortality.[7,8,9] More than 16,000 people now die annually of opioid-related causes in the United States alone, and similar trends have emerged in Canada, Australia, and Europe [10]. Many of these deaths could be avoided by more judicious prescribing of opioids in patients with chronic pain [10,11,12].
To minimize the risk of addiction and its attendant harms, clinical practice guidelines advocate various decision tools to stratify individual risk before initiating opioid therapy [5,13]. However, subjectivity remains in many aspects of opioid therapy [5,13,14]. This is supported by the observation that social and demographic factors, such as age, race and socioeconomic status, influence opioid prescribing patterns [15,16,17].
Few studies have explored the role of biological sex as it pertains to the safe prescribing of opioids in patients with chronic pain. There are several reasons why opioids might be prescribed differently to men and women, including differences in pain perception [18] and drug-seeking behaviour[19], as well as physician bias in the assessment of pain and formulation of a treatment plan [20]. Previous research suggests that women are more likely to be prescribed opioids, but men tend to receive more potent agents [1,15,21,22]. However, the majority of these studies are descriptive and focus only on initial prescriptions. [1,15,21,22] One small cohort study [23] examined the relationship between sex and dose escalation but had limited statistical power and did not examine mortality.
We sought to formally explore the relationship between sex, dose escalation and death due to overdose in a large cohort of patients receiving chronic opioid therapy for noncancer pain.
Methods
Setting
We performed a population-based cohort study among Ontarians between 15 and 64 years of age who received publicly funded opioid prescriptions between April 1^st^ 1997 and December 31^st^ 2010. These individuals have universal access to prescription drug coverage, hospital care and physicians’ services. All analyses were performed at the Institute for Clinical Evaluative Sciences (ICES), where various healthcare administrative databases are linked and analyzed in an anonymous fashion using encrypted, 10-digit health card numbers. This project was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre, Toronto, Canada.
Data Sources
We identified prescription records using the Ontario Drug Benefit Database, which contains comprehensive and highly accurate data of prescriptions dispensed to Ontarians eligible for public drug coverage [24]. Eligibility criteria for drug coverage among people younger than 65 years include disability, receipt of social assistance, high prescription drug costs relative to net household income, receipt of home care services and residence in a long-term care facility. We obtained demographic information from the Registered Persons Database, which contains one record for every Ontarian issued a health card number. We used the Ontario Cancer Registry to identify any previous diagnosis of cancer[25]. We used the Ontario Diabetes Database to ascertain the presence of diabetes [26], for inclusion in the Charlson Comorbidity Index. Inpatient hospitalization records were identified from the Canadian Institute for Health Information’s Discharge Abstract Database, and physician billing claims were obtained from the Ontario Health Insurance Plan Database.
Opioid-related deaths were identified by manual abstraction of records from the Office of the Chief Coroner for Ontario, as done previously [7,27]. These data are complete until December 31, 2011. By law, all deaths that do not arise from natural causes or are sudden and unexpected must be reported to the coroner. For this study, opioid-related deaths were defined as those in which the coroner’s investigation concluded so, based either on postmortem toxicology revealing opioid concentrations sufficiently high to cause death, or the coroner’s determination that a combination of drugs, including at least one opioid present at a clinically significant concentration, resulted in death. Deaths were considered unrelated to opioid use if another drug was present at a concentration high enough to cause death, even when one or more opioids were detected at levels that could be associated with therapeutic use[7].
Study Design
We identified cohorts of men and women who commenced treatment with an opioid, based upon prescriptions for oral codeine, morphine, oxycodone, hydromorphone or transdermal fentanyl. We restricted the analysis to patients newly treated with opioids by excluding those with any other opioid prescription in the preceding year. We did not include prescriptions for hydrocodone, which is available in Canada only as a liquid antitussive, or for methadone, which is almost exclusively prescribed for opioid addiction rather than for pain in Ontario.
Each patient’s observation began on the date of their first opioid prescription. Patients were followed from their first opioid prescription until discontinuation of opioid treatment (defined as an interval of more than 120 days between successive prescriptions), death from any cause, or the end of study period (December 31^st^, 2010), whichever occurred first. The maximum duration of publically-funded prescriptions in Ontario is 100 days. For patients with more than one eligible cohort entry date (by virtue of intervals greater than 120 days between successive prescriptions), we studied only the first course of therapy. To restrict the analysis to patients with noncancer pain, we excluded from the analysis individuals with any evidence of cancer prior to cohort entry, as well as patients with any physician claim or inpatient hospitalization for palliative care services in the 180 days preceding cohort entry.
In the primary analysis we studied patients receiving chronic opioid therapy, which we defined as three or more months of opioid treatment. These patients had one or more opioid prescriptions at least 91 days following their first prescription, with no interval of 120 days or more between successive prescriptions. In a secondary analysis, we examined all patients who commenced opioid therapy, regardless of the overall duration of treatment. While most such prescriptions represent short-term treatment for pain and do not progress to chronic therapy, we conducted this analysis because dose escalation and opioid-related death do sometimes occur in the first 3 months of therapy.
The primary outcome was defined as escalation to a daily opioid dose of more than 200 milligrams of morphine or equivalent. We chose this dose because it has been identified as a threshold in both American [5] and Canadian guidelines [13] and because higher doses confer increasing risk of adverse outcomes while lower doses are sufficient for pain control in the vast majority of patients. Our previous work demonstrates that doses exceeding 200 mg of morphine or equivalent increase the risk of motor vehicle collisions [28] and opioid-related mortality [27].
Dose was ascertained as described previously [27,28], incorporating the strength and number of tablets dispensed, the days supplied by the prescription and the potency of the opioid relative to morphine, defined using equivalence ratios published by the National Opioid Use Guideline Group [13]. The secondary outcome examined death from opioid-related causes, defined using provincial coroner’s data.
Statistical Analysis
We used standardized differences to compare baseline characteristics of men and women who commenced opioid therapy. Unlike significance testing, standardized differences are not influenced by sample size; values lower than 0.10 suggest negligible differences in the mean value of the characteristic between groups [29]. We therefore used Cox proportional hazards regression to estimate the risks of dose escalation and opioid-related mortality for men relative to women, after adjusting for all variables with a standardized difference greater or equal to 0.10, including age, documented alcohol-related disorder in the preceding 5 years, number of distinct non-opioid medications prescribed in the past 6 months and use of serotonergic antidepressants. We also adjusted for receipt of benzodiazepines, antipsychotic drugs and other psychotropic drugs or central nervous system (CNS) depressants in the preceding 180 days, as well as comorbidity defined using the Charlson comorbidity index [30].
The proportional hazards assumption was verified using a time-dependent exposure covariate and by inspection of log-log survival curves. We constructed Kaplan-Meier curves to characterize the incidence of both outcomes over time. All analyses were performed with SAS version 9.2 (SAS institute Cary N.C.) and used a two-tailed type I error rate of 0.05 as the threshold for statistical significance.
Results
During the 13-year study period, we identified 285,520 individuals who commenced treatment with an opioid. Within this cohort, 32,449 (11.4%) continued opioid therapy for 3 months or more, including 13,640 (42.0%) men and 18,809 (58.0%) women. Overall, 589 patients (1.8%) escalated to high dose therapy over a median follow-up of 186 days (interquartile range 117 to 442 days), while 59 patients (0.2%) died of opioid-related causes at a median of 2.6 years (interquartile range 1.1 to 5.2 years) from their first opioid prescription.
Compared to women, men receiving opioids were slightly older, more likely to have a documented alcohol use disorder, and less likely to receive antidepressants (Table 1). Men and women were otherwise similar with regard to demographics, comorbidity measures, physician utilization and medication use at baseline.
Table 1: Baseline characteristics of men and women receiving chronic opioid therapy.
Among patients receiving chronic opioid therapy, 319 (2.3%) men and 270 (1.4%) women escalated to high dose therapy, representing roughly 1 out of every 45 men and 1 out of every 70 women in our sample. In total, 37 (0.3%) men and 22 (0.1%) women died of opioid-related causes, representing 1 out of every 350 men and 1 out of every 850 women receiving chronic opioid therapy, respectively. After multivariable adjustment, men were almost 50% more likely to escalate to high-dose opioids (adjusted hazard ratio 1.44; 95% confidence interval, 1.21 to 1.70; Table 2 and Fig 1) and twice as likely to experience an opioid-related death (adjusted hazard ratio 2.04; 95% confidence interval 1.18 to 3.53; Table 3 and Fig 2) compared to women. Those who escalated to high dose opioid therapy were nearly 24 times as likely to die as those who did not escalate (3.1% vs. 0.1%, respectively).
Table 2: Escalation to high dose opioid therapy among men and women a .
Table 3: Opioid-related death during chronic opioid therapy in men and women.
Escalation to high dose opioid therapy among men and women.Kaplan-Meier curves of opioid dose escalation to an average daily dose exceeding 200 mg of morphine (or equivalent) among men and women with at least 91 days of continuous opioid therapy. P values were determined by Cox proportional hazards regression.
Opioid-related death among men and women.Kaplan-Meier curves of opioid-related mortality among men and women with at least 91 days of continuous opioid therapy. P values were determined by Cox proportional hazards regression.
We found similar results in the analysis of all 285,520 subjects who received any opioid prescription, regardless of the duration of therapy. Overall, 814 patients (0.3%) escalated to high-dose therapy and 91 patients (0.03%) died of opioid overdose. In this analysis, men also faced an increased risk of escalation to high-dose opioid therapy (adjusted hazard ratio 1.52; 95% confidence interval 1.32 to 1.76; Table 2) and opioid-related death (adjusted hazard ratio 2.18; 95% confidence interval 1.40 to 3.38; Table 3) compared to women.
Discussion
In this population-based cohort study spanning 13 years, we found that men prescribed opioids for chronic noncancer pain were more likely than women to escalate to high-dose therapy and die of opioid overdose, even after adjustment for age, comorbidity, documented alcohol-related disorder and medication use. Moreover, both outcomes were more common than anticipated, with 1 of every 55 patients escalating to high-dose opioid therapy and 1 of every 550 dying of an opioid-related cause.
The importance of these findings is highlighted by the fact that tens of millions of patients worldwide receive chronic opioid therapy each year. Sales of opioids have quadrupled in the last decade[8], and more than 238 million opioid prescriptions were issued in the United States in 2011 alone, making them the third most widely prescribed drug class after lipid-lowering drugs and antidepressants[31].
Determining which patients are at risk of opioid dose escalation, addiction or opioid-related death is challenging, and clinical practice guidelines [5,13] advocate various decision tools to stratify individual risk before initiating or up-titrating opioid therapy. Despite these efforts, opioid deaths have continued to increase [9]. Opioid-related deaths represent more than 40% of all mortality from poisoning [9] and now outnumber deaths from alcoholic liver disease and HIV in North America[10].
Our findings underscore the importance of revisiting the indications for chronic opioid therapy, particularly at high doses. This is especially true in light of the paucity of good evidence regarding the safety and effectiveness of long term opioid therapy [14,32,33], as well as the lack of evidence demonstrating their superiority to other analgesics in treating chronic noncancer pain[14,34]. It is important to recognize that, as our findings indicate, more than 10% of patients treated anew with opioids progress to chronic therapy. Moreover, by identifying males to be at greater risk for escalation and opioid-related mortality, physicians can exercise particular caution when considering opioids for chronic noncancer pain in men.
Ultimately, further studies are required both to elucidate the role of opioids in chronic noncancer pain and to discern which patients can tolerate opioids safely.
Our study represents the first population-based study to document biological sex as a significant predictor of opioid dose escalation and opioid-related death among patients commencing chronic opioid therapy. However, some limitations of our work merit emphasis. The study’s findings derive from subjects receiving publicly funded prescription coverage and may not be generalizable to all patients. However, this is a particularly relevant population because social disadvantage is associated with higher rates of both opioid prescribing and opioid misuse [3,35]. Second, we cannot determine with confidence why men face an increased risk of dose escalation and death during chronic opioid therapy. Although a propensity for high risk behaviours surrounding opioids among men may partly explain our findings [36,37], the explanation is likely complex and multifactorial. Third, the nature of our data makes it difficult to ascertain the appropriateness of diagnoses and treatment as well as adherence to prescribed medication. Similarly, we have no reliable data on recreational drug use, save for alcohol use disorder. Additional research on the role of other illnesses, particularly mental health disorders, is needed to better identify those at particular risk of opioid-related harms. Finally, it merits note that no female deaths occurred in the final 6 years of study. This most likely represents depletion of susceptible individuals [38] and competing mortality from other causes of death.
Importantly, our methods necessarily underestimate both the amount of opioids consumed by patients and the number of deaths occurring during chronic therapy. We have no information about receipt of opioids from other sources, including illicit sources or prescriptions paid in cash or by other insurers. We purposefully excluded patients with long intervals between prescriptions, as well as those who received methadone. Considering the extent of diversion [39] and the high opioid-related mortality attributed to methadone [40], the true risks of opioid therapy are likely greater than our findings suggest.
In summary, in a large population of patients initiating opioid therapy for chronic noncancer pain, we found that men were more likely than women to escalate to high-dose opioid therapy and more than twice as likely to die of an opioid overdose. Moreover, both outcomes were much more common than anticipated. Although our findings underscore the importance of judicious opioid use in both men and women, they suggest that particular vigilance be applied to men, especially as doses begin to escalate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gomes T, Juurlink DN, Dhalla IA, Mailis-Gagnon A, Paterson JM, Mamdani MM. Trends in opioid use and dosing among socio-economically disadvantaged patients. Open Med 2011;5:e 13–e 22. 22046214 PMC 3205807 · pubmed ↗
- 2Caudill-Slosberg MA, Schwartz LM, Woloshin S. Office visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs. 2000. Pain 2004;109:514–9. 1515771410.1016/j.pain.2004.03.006 · doi ↗ · pubmed ↗
- 3Sullivan MD, Edlund MJ, Fan MY, Devries A, Brennan Braden J, Martin BC. Trends in use of opioids for non-cancer pain conditions 2000–2005 in commercial and medicaid insurance plans: The TROUP study. Pain 2008;138:440–9. 10.1016/j.pain.2008.04.027 18547726 PMC 2668925 · doi ↗ · pubmed ↗
- 4Boudreau D, Von Korff M, Rutter CM, Saunders K, Ray GT, Sullivan MD, et al Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol Drug Saf 2009;18:1166–75. 10.1002/pds.1833 19718704 PMC 3280087 · doi ↗ · pubmed ↗
- 5Chou R, Fanciullo GJ, Fine PG, Adler JA, Ballantyne JC, Davies P, et al Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain 2009;10:113–30. 10.1016/j.jpain.2008.10.008 19187889 PMC 4043401 · doi ↗ · pubmed ↗
- 6Portenoy RK, Foley KM. Chronic use of opioid analgesics in non-malignant pain: report of 38 cases. Pain 1986;25:171–86. 287355010.1016/0304-3959(86)90091-6 · doi ↗ · pubmed ↗
- 7Dhalla IA, Mamdani MM, Sivilotti ML, Kopp A, Qureshi O, Juurlink DN. Prescribing of opioid analgesics and related mortality before and after the introduction of long-acting oxycodone. CMAJ 2009;181:891–6. 10.1503/cmaj.090784 19969578 PMC 2789126 · doi ↗ · pubmed ↗
- 8Centers for Disease Control and Prevention (CDC). Vital signs: Overdoses of prescription opioid pain relievers---united states, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60:1487–92. 22048730 · pubmed ↗