Prospective clinical study of R-CMD therapy for indolent B cell lymphoma and mantle cell lymphoma from the Hokuriku Hematology Oncology Study Group
Tomoyuki Sakai, Yasufumi Masaki, Nozomi Otsuki, Ippei Sakamaki, Shinji Kishi, Takayoshi Miyazono, Yoshimasa Urasaki, Jun Murakami, Tomomi Satoh, Takuji Nakamura, Haruka Iwao, Akio Nakajima, Takafumi Kawanami, Miyuki Miki, Yoshimasa Fujita, Masao Tanaka, Toshihiro Fukushima

TL;DR
This study evaluated the effectiveness and safety of R-CMD therapy for treating indolent B cell lymphoma and mantle cell lymphoma, showing promising results with high response rates.
Contribution
The study provides new evidence on the efficacy of R-CMD therapy for indolent B cell lymphoma and mantle cell lymphoma in a prospective clinical setting.
Findings
26 out of 33 patients achieved complete or unconfirmed complete response to R-CMD therapy.
R-CMD therapy was found to be relatively convenient and effective for treating indolent B cell lymphoma and mantle cell lymphoma.
Four patients relapsed after remission, highlighting the need for continued monitoring and infection prevention.
Abstract
Standardized treatments for indolent B cell lymphoma primarily consisting of follicular lymphoma (FL) and for mantle cell lymphoma (MCL) have yet to be established. Here the Hokuriku Hematology Oncology Study Group conducted a multicenter prospective study to investigate the efficacy and safety of a combination regimen of rituximab, cladribine, mitoxantrone, and dexamethasone (R-CMD) in indolent B cell lymphoma and MCL. A total of 33 CD20-positive patients who received care between January 2008 and August 2011 were investigated. These patients’ illnesses were FL (n = 21), nodal marginal zone B cell lymphoma (NMZB, n = 3), MCL (n = 3), splenic marginal zone B cell lymphoma (n = 2), hairy cell leukemia (n = 1), Waldenstrom macroglobulinemia (WM, n = 1), and lymphoplasmacytic lymphoma (LPL, n = 2). Patients received four 21-day cycles of rituximab 375 mg/m2 (day 1), cladribine 0.10 mg/kg…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
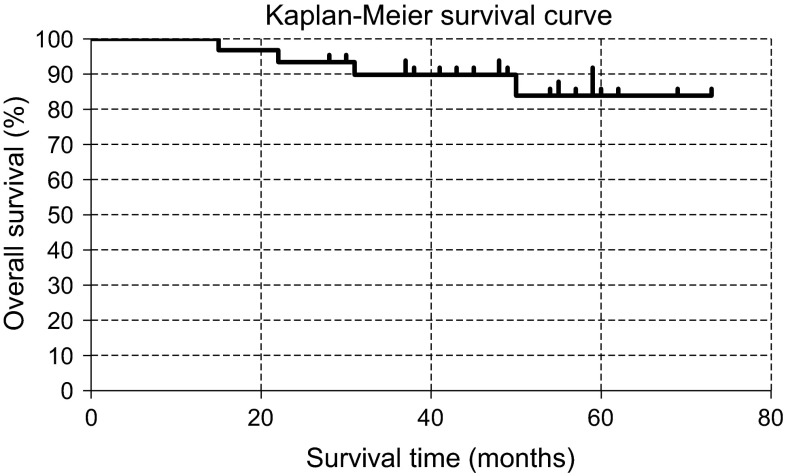 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Viral-associated cancers and disorders · Chronic Lymphocytic Leukemia Research
Introduction
Standardized treatments have yet to be established for indolent B cell lymphoma, which predominantly consists of follicular lymphoma (FL). Although a temporary effect is observed with the conventional CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine, and prednisolone) regimen, this regimen does not achieve curein indolent B cell lymphoma, and rather, indolent B cell lymphoma is known to have a worse long-term prognosis than aggressive lymphoma. In addition, standardized treatments have yet to be established for mantle cell lymphoma (MCL), a disease with poor prognosis that most commonly affects the elderly. Purine nucleoside derivatives such as fludarabine and cladribine block the adenosine metabolic pathway where adenosine deaminase is involved, and are known to be effective in indolent B cell lymphoma due to their treatment effects on cells in the quiescent state. The FMD regimen (fludarabine, mitoxantrone, and dexamethasone) [1–4] has been studied relatively frequently in recent years and has been shown to result in favorable treatment outcomes in indolent B cell lymphoma. However, currently in Japan, there is limited health insurance coverage for fludarabine injections, and using them for treating lymphoma is problematic at the present time. Because the mechanism of action and effects of fludarabine and cladribine are considered to be nearly equivalent, the CMD regimen, which is the FMD regimen but with fludarabine changed to cladribine, is considered to have nearly equivalent treatment effects as FMD. For this reason, the effects of CMD [5] and treatments that are similar to CMD [6–9] have been studied. Furthermore, rituximab is known to have a long blood half-life in in vivo kinetics, and its effects are sustained for a long time; thus, by adding rituximab to CMD (R-CMD), an enhancement in treatment effect can be anticipated. In a pilot study in our department, we confirmed the treatment effect and safety in patients who received R-CMD therapy. We therefore considered that it is necessary to verify its efficacy and safety in a phase II trial. Here, we report the results from this multicenter prospective clinical study.
Patients and methods
Patients
Adult (≥20 years old) patients with initial or recurrent (up to first recurrence) indolent B cell lymphoma [FL, MALT lymphoma, nodal and splenic marginal zone B cell lymphomas (NMZB, SMZB), lymphoplasmacytic lymphoma (LPL) ≈ Waldenstrom macroglobulinemia (WM), hairy cell leukemia (HCL), etc.] or MCL, who were pathologically diagnosed with Ann Arbor stages II–IV and confirmed to be CD20 positive with pathology or flow cytometry, were selected. Exclusion criteria were as follows: CD20 negative, severe infection, prior history of receiving similar chemotherapy for treating malignant lymphoma, HIV positive, HTLV1 positive, HBV-Ag positive, high titer of HBc-Ab, scheduled to undergo autologous or allogeneic hematopoietic stem cell transplantation and determined as unsuitable for the study by a physician. A total of 33 patients who received care between January 2008 and August 2011 at one of the four centers were enrolled. The disease types were as follows: FL (n = 21), NMZB (n = 3), MCL (n = 3), SMZB (n = 2), HCL (n = 1), WM (n = 1), and LPL (n = 2). There were 17 men and 16 women, with a median age of 65 years (range 45–81 years). Nine patients had previously undergone treatment (Table 1). In addition, all patients enrolled in the study gave written consent themselves. This study was approved by the IRB of each center.Table 1. Patient characteristicsNo. (%)Patients33Sex Male17 (52) Female16 (48)Age, years Median65 Range45–81Histopathology Follicular lymphoma21 (64) Nodal marginal zone lymphoma3 (9) Mantle cell lymphoma3 (9) Splenic marginal zone lymphoma2 (6) Hairy cell leukemia1 (3) Waldenstrom macroglobulinemia1 (3) Lymphoplasmacytic lymphoma2 (6) Prior therapy9 (27)Stage 10 (0) 28 (24) 310 (30) 415 (46)B symptoms2 (6)B symptoms: fever, weight loss, night sweats; prior therapy: R-CHOP, rituximab, splenectomy, plasma exchange, prednisolone, VP16, auto-peripheral blood stem cell transplantationStage I was not included
Methods
Patients received four 21-day cycles of rituximab 375 mg/m^2^ (day 1), cladribine 0.10 mg/kg (days 1–3), mitoxantrone 8 mg/m^2^ (day 1), and dexamethasone 8 mg/body (days 1–3) and additionally received four times of rituximab at 4-week intervals (Table 2). For prophylaxis, sulfamethoxazole/trimethoprim combination was given at a dose of 800 mg of sulfamethoxazole/day twice a week to prevent pneumocystis infection, and an antifungal agent was given from the start of the treatment to 2 months after its completion to prevent mycosis. Preventative administration of common antibiotics was not specified. Vaccinations for influenza and other diseases were avoided from the start of the treatment to 3 months after its completion.Table 2R-CMD regimenDrugsDoseDay 1Day 2Day 3Rituximab375 mg/m^2^ ↓Cladribine0.10 mg/kg↓↓↓Mitoxantrone8 mg/m^2^ ↓Dexamethasone8 mg/body↓↓↓R-CMD, rituximab plus cladribine, mitoxantrone, and dexamethasone; R-CMD regimen: four 3-week R-CMD regimen + four 4-week rituximab monotherapy regimen
The complete response (CR) rate and adverse events were determined in accordance with the standardized response criteria for non-Hodgkin’s lymphoma from an international workshop report by Cheson et al. [10] and CTCAGv4.0 (UMIN trial ID: 1341), respectively. The primary end point was the CR rate, and the secondary end points were the frequency of adverse events, overall survival (OS), and overall response rate (ORR). Patients were followed until death or 10 years after treatment completion, whichever occurred first. OS curves were estimated using the Kaplan–Meier method.
Results
Response
A complete response/unconfirmed complete response (CR/CRu) was achieved in 26 out of 33 patients (79 %), and a partial response (PR) was achieved in six patients (18 %). The ORR was 97 %, with one patient whose condition progressed (3 %). Moreover, excluding patients with MCL, 24 patients (80 %) had CR, five patients (17 %) had PR, and one patient (3 %) had disease progression. There were only three patients with MCL, and two of these patients achieved CR/Cru, whereas the remaining one patient achieved PR (Table 3). In newly diagnosed patients alone, CR/CRu, PR, and progressive disease (PD) were observed in 83, 16, and 0 %, respectively. In addition, recurrence was observed in one patient with FL, two patients with MCL, and one patient with LPL. CR/CRu was 67 %, PR was 22 %, and PD was 11 % in patients with previous treatment history.Table 3. ResponseAllNon-MCLMCL N = 33 N = 30 N = 3CR/Cru (%)26 (79)24 (80)2 (67)PR (%)6 (18)5 (17)1 (33)SD (%)0 (0)0 (0)0 (0)PD (%)1 (3)1 (3)0 (0)ORR (%)32 (97)29 (97)3 (100) CR complete response, CRu unconfirmed CR, PR partial response, SD stable disease, PD progressive disease, ORR overall response rate, which includes CR + CRu + PR, All All enrolled patients, MCL mantle cell lymphoma
Disease-free survival and OS
At the present time, recurrence has been observed in 12 % of the patients (1 patient with FL, 2 patients with MCL, and 1 patient with LPL). No other recurrences have been observed, and the maximum disease-free survival thus far has been 5 years and 4 months. With a median follow-up of 4 years, the cumulative survival rate was 84 % with four deaths at the 73-month time point (Fig. 1). These deaths were due to progression in lymphoma combined with pancreatic cancer that developed later (n = 1), metastatic liver cancer (n = 1), cirrhosis type C (n = 1), or pneumocystis pneumonia (n = 1).Fig. 1. Overall survival for all patients after R-CMD therapy
Toxicity
Grade 3 or greater hematological toxicity was observed in 30 out of 33 patients. Specifically, ≥grade 3 leukopenia,neutropenia,lymphopenia, and thrombocytopenia were observed in 73, 76, 71, and 6 % of the patients, respectively. None of the patients exhibited ≥grade 3 anemia (Table 4). Advanced neutropenia and lymphopenia were observed, but all cases were transient. Non-hematological toxicity included grade 2 constipation in 27 % and alopecia in 6 % of the patients. Additionally, five patients (15 %) developed an infection (one patient each with sepsis + herpes labialis, pyothorax + bacterial fasciitis, urinary tract infection, herpes zoster, and pneumocystis pneumonia). Although the patient with pneumocystis pneumonia died without showing any improvements, other infections did not become serious and improved with treatment. However, treatment continuation was determined to be difficult in the patients who developed pyothorax + bacterial fasciitis and urinary tract infection, and these patients subsequently discontinued the regimen. Although pancreatic cancer developed in one patient after the completion of treatment, secondary cancers such as myelodysplastic syndrome or leukemia have not been confirmed at the present time.Table 4. Adverse eventsGrade 1Grade 2Grade 3Grade 4 N (%) N (%) N (%) N (%)Hematological Leukopenia1 (3)8 (24)19 (58)5 (15) Neutropenia1 (3)6 (18)15 (46)10 (30) Lymphopenia1 (4)5 (18)16 (57)4 (14) Anemia16 (49)8 (24)0 (0)0 (0) Thrombocytopenia8 (24)3 (9)2 (6)0 (0)Non-hematological Constipation10 (30)9 (27)00 Alopecia9 (27)2 (6)–– Infections2 (6)1 (3)120 Infusion-related reaction01 (3)00 Rash02 (6)00 Other2 (6)Other non-hematological toxicities included two patients with hand stiffnessOne patient died due to pneumocystis pneumonia (grade 5)Two patients discontinued treatment due to adverse events (one patient with pyothorax + necrotizing bacterial fasciitis and one patient with urinary tract infection)
Discussion
Due to the slow disease progression of indolent B cell lymphomas, which primarily consist of FL, it is rare for sudden exacerbations to occur after its onset. Nonetheless, standardized treatments have yet to be established for this disease. Although temporary effects of the conventional CHOP regimen are observed in indolent B cell lymphoma, this particular therapy does not achieve cure, and the long-term prognosis is known to be rather worse than that of aggressive lymphoma. In addition, standardized treatments for MCL, a disease with poor prognosis that most commonly affects the elderly, have yet to be established as well. With the recent introduction of bendamustine and ibritumomab tiuxetan, an improvement in survival and prognosis is anticipated; however, it is unknown whether or not either of these drugs alone can achieve a complete cure in a monotherapy regimen [11–13]. Rummel et al. [14] conducted a phase III multicenter randomized controlled trial to compare the efficacy of the bendamustine plus rituximab (RB) regimen versus the R-CHOP regimen in patients with indolent B cell lymphoma and MCL and reported that the RB regimen may be more beneficial. In this trial, progression-free survival (PFS) was significantly better in the RB group compared to the R-CHOP group in the overall study population inclusive of all disease types (p < 0.0001). In the analysis by disease type, the authors found that PFS was significantly longer in FL, MCL, and primary WM, but a significant difference was not observed in marginal-cell lymphoma. There was no significant difference in ORR (93 % in the RB group and 91 % in the R-CHOP group); however, the CR rate was 40 % in the RB group and 30 % in the R-CHOP group, indicating a superiority of the RB regimen (p = 0.021). OS was not significantly different between the two groups. Sinha et al. conducted a phase I trial of the combined regimen with bortezomib and R-CHOP in previously untreated patients with indolent B cell lymphoma [15] and found favorable outcomes with an ORR of 100 %, CR of 68 %, and 3-year PFS of 89.5 %. Furthermore, Fowler et al. [16] reported the results a phase II trial of the combination regimen of bortezomib, bendamustine, and rituximab (VERTICAL trial) in 73 patients with relapsed or refractory FL and concluded that ORR was 88 %, CR was 53 %, and the median PFS was 14.9 months. Leonard et al. [17] evaluated the combination regimen of lenalidomide and rituximab in recurrent and refractory FL (CALGB trial) and reported that the ORR was 75 % with a CR of 32 % and event-free survival of 24 months.
In the present study, 26 out of 33 patients achieved complete remission (CR rate, 79 %). At the present time, with the exception of the recurrence that occurred in 12 % of the patients (1 with FL, 2 with MCL, and 1 with LPL) and PD in 3 % of the patients (1 with FL), recurrence has not been observed for a maximum of 5 years and 4 months. The cumulative survival rate at the 73-month time point was 84 %, indicating results that are comparable to similar regimens that have been reported previously (Table 5) [1, 18–22]. Therefore, we consider that R-CMD therapy is a relatively convenient and effective treatment method for indolent B cell lymphoma. In addition, although ≥grade 3 leukopenia, neutropenia, and lymphopenia were observed at high frequencies, all cases were transient and none of them worsened. Serious non-hematological toxicities were rare in patients who received treatment for the first time, and alopecia, which is highly common in R-CHOP, was also rarely observed. In addition, although a combination regimen with multiple drugs that include cladribine is known to cause adverse events at high frequencies in recurrent and refractory lymphomas, toxicity is considered to be within the tolerable range in newly diagnosed patients. Nonetheless, thorough infection prevention is necessary to suppress the number and function of both B cells and T cells.Table 5. Similar clinical trialsStudy n RegimenORR (%)CR (%)Response timeOS (years)Apostolia et al. [1] (untreated indolent NHL maintenance therapy+)73FND977941 % (FFS)84 (5)Velasquez et al. [18] (untreated indolent NHL)78FM944438 % (PFS)88 (4)McLaughlin et al. [19] (untreated SLL or follicular lymphoma)149FND-R1009277 % (FFS)95 (3)Bordonaro et al. [20] (newly diagnosed indolent NHL)18FND947252 % (PFS)67 (2)Montoto et al. [21] (untreated follicular lymphoma)120FCM948358 % (PFS)89 %Tomasz et al. [22] (relapse or refractory indolent NHL)28FPD-R896374 % (TTP)92 (3)This study, 2013 (untreated or first relapse indolent NHL)33R-CMD9778–84 (4) ORR overall response rate; CR complete response; PFS progression-free survival; OS overall survival; FFS failure-free survival; TTP time to tumor progression; FND fludarabine, mitoxantrone, and dexamethasone; FM fludarabine and mitoxantrone; FND-R FND plus rituximab; FCM fludarabine, cyclophosphamide, and mitoxantrone; FPD-R pixantrone, fludarabine, and dexamethasone plus rituximab; R-CMD rituximab plus cladribine, mitoxantrone, and dexamethasone; SLL small lymphocytic lymphoma; NHL non-Hodgkin lymphoma
Conclusion
R-CMD therapy, a regimen with rituximab added to the FMD regimen in which fludarabine is switched to cladribine, showed effects that were comparable to FMD and a favorable complete remission induction rate. However, the observation time is still short, and further follow-up is necessary in the future to assess long-term prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tsimberidou AM Mc Laughlin P Younes A Rodriguez MA Hagemeister FB Sarris A Fludarabine, mitoxantrone, dexamethasone (FND) compared with an alternating triple therapy (ATT) regimen in patients with stage IV indolent lymphoma Blood 20021004351435710.1182/blood-2001-12-026912393618 · doi ↗ · pubmed ↗
- 2Keating MJ Mc Laughlin P Cabanillas F Low-grade non-Hodgkin’s lymphoma-development of a new effective combination regimen (fludarabine, mitoxantrone and dexamethasone; FND)Eur J Cancer Care 199764 Suppl 212610.1111/j.1365-2354.1997.tb 00321.x 9460339 · doi ↗ · pubmed ↗
- 3Mc Laughlin P Hagemeister FB Romaguera JE Sarris AH Pate O Younes A Fludarabine, mitoxantrone, and dexamethasone: an effective new regimen for indolent lymphoma J Clin Oncol 19961412621268864838210.1200/JCO.1996.14.4.1262 · doi ↗ · pubmed ↗
- 4Tsimberidou AM Younes A Romaguera J Hagemeister FB Rodriguez MA Feng L Immunosuppression and infectious complications in patients with stage IV indolent lymphoma treated with a fludarabine, mitoxantrone, and dexamethasone regimen Cancer 200510434535310.1002/cncr.2115115948158 · doi ↗ · pubmed ↗
- 5Robak T Gora-Tybor J Urbańska-RyśH Krykowski E Combination regimen of 2-chlorodeoxyadenosine (cladribine), mitoxantrone and dexamethasone (CMD) in the treatment of refractory and recurrent low grade non-Hodgkin’s lymphoma Leuk Lymphoma 1999323593631003703410.3109/10428199909167397 · doi ↗ · pubmed ↗
- 6Flinn IW Byrd JC Morrison C Jamison J Diehl LF Murphy T Fludarabine and cyclophosphamide with filgrastim support in patients with previously untreated indolent lymphoid malignancies Blood 200096717510891432 · pubmed ↗
- 7Rummel MJ Chow KU Karakas TJäger E Mezger Jvon Grünhagen U Reduced-dose cladribine (2-Cd A) plus mitoxantrone is effective in the treatment of mantle-cell and low-grade non-Hodgkin’s lymphoma Eur J Cancer 2002381739174610.1016/S 0959-8049(02)00143-012175690 · doi ↗ · pubmed ↗
- 8Robak T Smolewski P Urbanska-Rys H Gora-Tybor J Blonski JZ Kasznicki M Rituximab followed by cladribine in the treatment of heavily pretreated patients with indolent lymphoid malignancies Leuk Lymphoma 20044593794410.1080/104281903200015982515291352 · doi ↗ · pubmed ↗