Esophageal Intubation of an Infant
Jana L. Anderson, Kharmene Sunga, Annie Sadosty

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
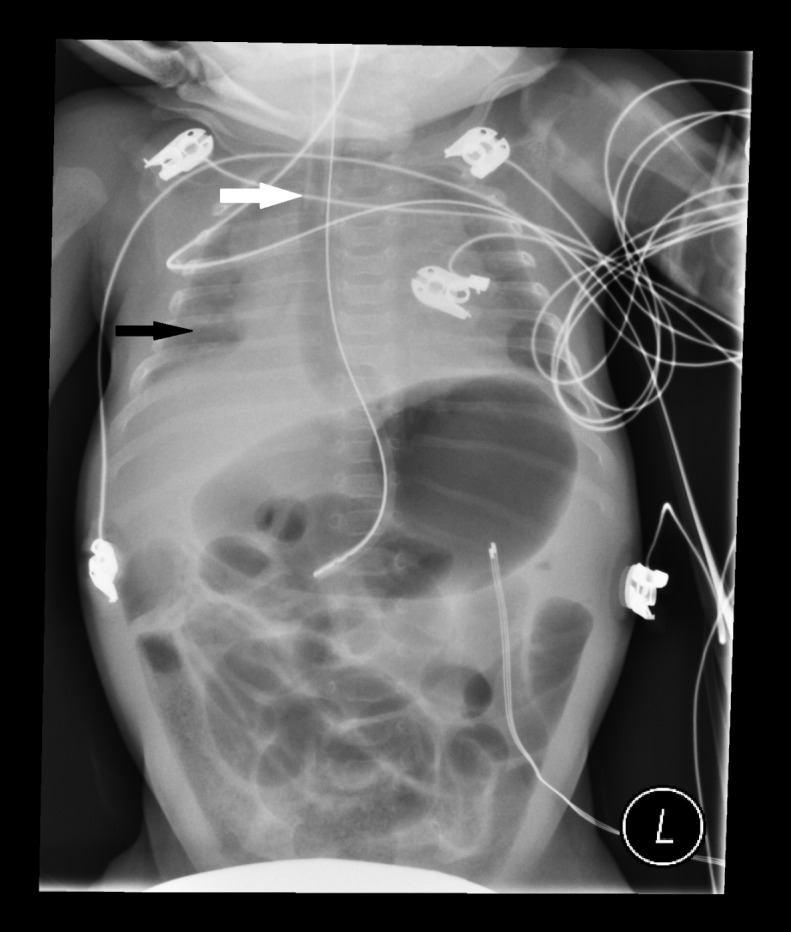 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Tracheal and airway disorders · Respiratory Support and Mechanisms
A 68-day-old former 30-week infant presented with listlessness, apnea and bradycardia. The patient was intubated for airway protection. After intubation, breath sounds were auscultated bilaterally and a Pedi-Cap carbon dioxide detector had color change from purple to yellow. A nasogastric tube (NGT) was placed and a post-procedural chest radiograph was obtained (Figure).
There are several features of esophageal intubation: low lung volumes, esophageal and gastric distention despite NGT placement and juxtaposition of the endotracheal tube (ETT) relative to the NGT.1–2 Other findings of esophageal intubation not seen here are identification of the ETT distal to the carina or outside of the tracheal-bronchial air column.3 Due to high success rates of endotracheal intubation in the emergency department,4–5 these findings are rare and may be overlooked. In this case, misleading clinical evidence was obtained through auscultation of bilateral breath sounds, visualization of endotracheal tube condensation, positive change on the carbon dioxide colorimeter and post-procedural hemodynamic and oxygenation stability. Previous literature, however, has demonstrated false-positive colorimetric change from swallowed air with pre-intubation positive pressure ventilation,6–7 hence the importance of radiographic identification of ETT location. In this patient, esophageal intubation was recognized after continuous capnography revealed absence of waveform.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bagshaw O Gillis J Schell D Delayed recognition of esophageal intubation in a neonate: role of radiologic diagnosis Crit Care Med 19942212202020237988144 · pubmed ↗
- 2Dittrich KC Delayed recognition of esophageal intubation CJEM 20024141441763714710.1017/s 1481803500006047 · doi ↗ · pubmed ↗
- 3Salem MR Baraka AS Confirmation of endotracheal intubation Hagberg CA Benumof and Hagberg’s Airway Management Third Edition Philadelphia Saunders 2013657682
- 4Sagarin MJ Barton ED Chng YM National Emergency Airway Registry Investigators Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts Ann Emerg Med 20054643283361618746610.1016/j.annemergmed.2005.01.009 · doi ↗ · pubmed ↗
- 5Walls RM Brown CA 3rd Bair AENEAR II Investigators Emergency airway management: a multi-center report of 8937 emergency department intubations J Emerg Med 20114143473542043428910.1016/j.jemermed.2010.02.024 · doi ↗ · pubmed ↗
- 6Gomes SB Mychaskiw G 2nd Failure of the Easy Cap II CO 2 detector to indicate esophageal intubation J Clin Anesth 20122443523532260859810.1016/j.jclinane.2011.06.026 · doi ↗ · pubmed ↗
- 7Hughes SM Blake BL Woods SL False-positive results on colorimetric carbon dioxide analysis in neonatal resuscitation: potential for serious patient harm J Perinatol 200727128008011803416610.1038/sj.jp.7211831 · doi ↗ · pubmed ↗