Borderline Lepromatous Leprosy with Type 1 (Reversal) Reactions in a Chinese Man
Xi’an Fu, Hong Liu, Furen Zhang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
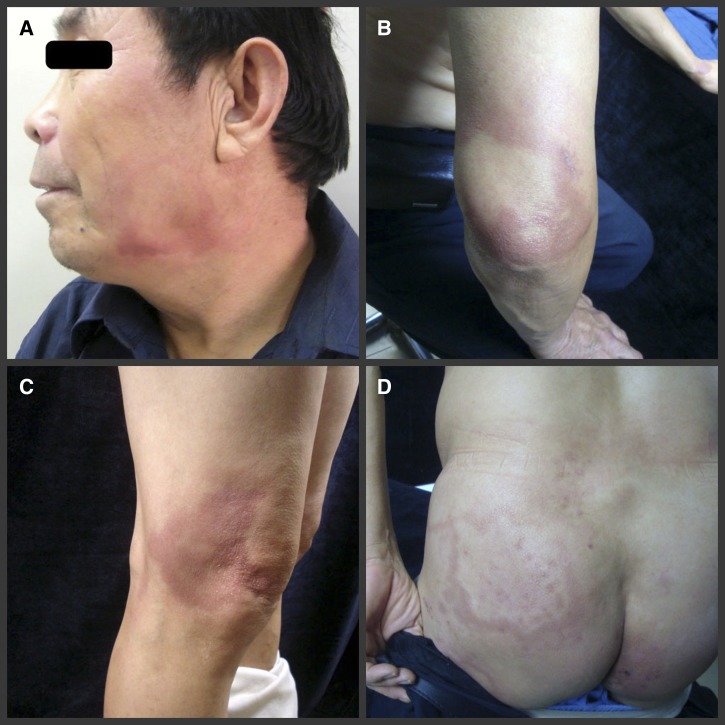 Figure 1
Figure 1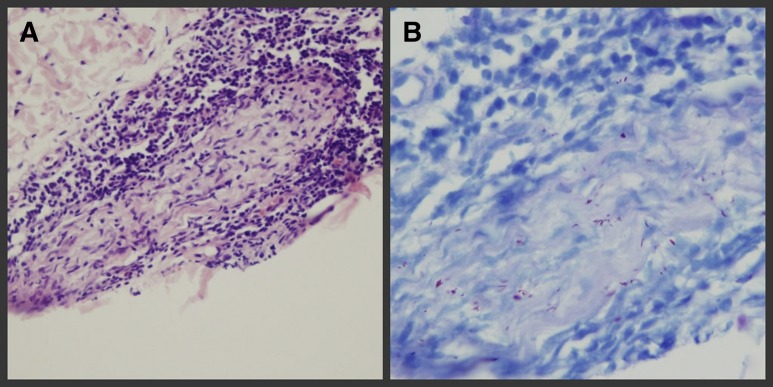 Figure 2
Figure 2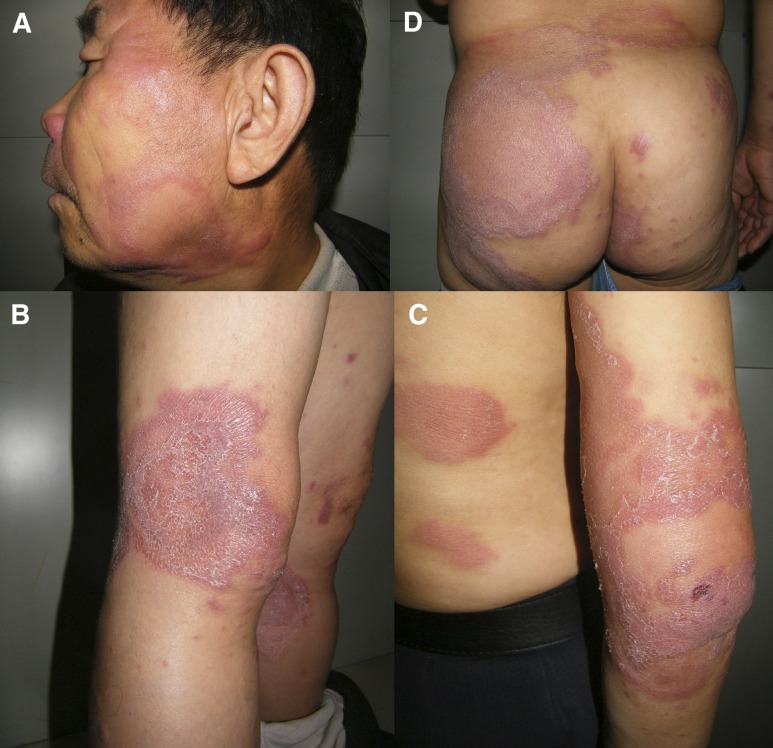 Figure 3
Figure 3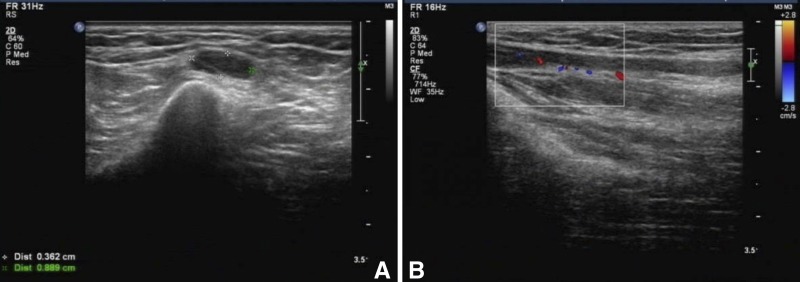 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeprosy Research and Treatment · Mycobacterium research and diagnosis · Infectious Diseases and Tuberculosis
A 59-year-old man diagnosed with borderline lepromatous leprosy developed reddish patches and plaques on the face, which progressively enlarged and spread to the trunk and limbs (Figure 1A–D Figure 1.Pre-therapy clinical photograph showing reddish patches and plaques appeared on the patient’s face (A), elbow (B), knee (C), and buttock (D).). Other superficial nerves appeared normal. Biopsy showed plasmocytic and lymphocytic infiltration in the nerve tract, and was 4+ acid-fast bacilli (AFB)–stain positive suggesting Mycobacterium leprae (Figure 2A and B Figure 2.Pre-therapy histopathologic analysis showing (left leg): (A) plasmocytic and lymphocytic infiltration surrounding dermal nerve and Schwann cells and inflammatory cell infiltrated into nerve tract (Hematoxylin and Eeosin [H&E] staining ×400), and (B) positive staining for lepra bacilli (4+) (acid-fast bacilli [AFB] stain).); this was confirmed by real-time polymerase chain reaction (PCR). The HLA-B*13:01 test was negative. Two weeks after rifampin, dapsone, and clofazimine (World Health Organization multidrug therapy [WHO MDT] regimen) were started, the skin lesions (hypochromic macules) became red, edematous, and enlarged (Figure 3A–D Figure 3.Post-therapy clinical photograph (2 weeks after initiation of multidrug therapy [MDT]). The preexisting lesions in the form of hypochromic macules turned red, edematous, squamous, enlarged, and the inflammatory infiltration aggravated, face (A), knee (B), elbow (C), and buttock (D).). Both ulnar nerves became tender and thickened; ultrasonography showed reduction of blood flow (Figure 4A and B Figure 4.Post-therapy (2 weeks after initiation of multidrug therapy [MDT]) ultrasonography and color Doppler images of peripheral nerve of the patient. (A) Cross-section scan of the right side ulnar nerve with hypoechoic fascicles: 0.889 cm at its widest point and (B) abnormal blood flow signals around the right ulnar nerve.). Collectively these findings indicated a type 1 conversion reaction (T1R) (Figure 2C). One year after prednisone was started (40 mg/day for 3 months with progressive tapering), the T1R was found to be completely resolved.
In leprosy, type 1 and type 2 reactions—whether spontaneous or related to treatment—are the main causes of morbidity. T1Rs result from cell-mediated immunity affecting up to 30% of susceptible individuals.1 Nonpolar forms of leprosy are the primary risk factor for the occurrence of T1Rs.2 Systemic corticosteroids remain the mainstay of treatment of T1Rs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Walker SL Lockwood DN 2008 Leprosy type 1 (reversal) reactions and their management Lepr Rev 7937238619274984 · pubmed ↗
- 2Nery JA Bernardes Filho F Quintanilha J Machado AM Oliveira Sde S Sales AM 2013 Understanding the type 1 reactional state for early diagnosis and treatment: a way to avoid disability in leprosy An Bras Dermatol 887877922417318510.1590/abd 1806-4841.20132004 PMC 3798356 · doi ↗ · pubmed ↗