Posterior Chamber Hemorrhage during Fluorescein Angiography
Manuel A. P. Vilela

TL;DR
This paper reports a rare case of eye bleeding during a routine eye imaging procedure in a patient with an artificial lens.
Contribution
The first documented case of posterior chamber hemorrhage during fluorescein angiography without a clear triggering event.
Findings
A 76-year-old patient experienced dense posterior chamber hemorrhage during fluorescein angiography.
The hemorrhage was linked to contact between the intraocular lens and the iris, worsened by mydriatics.
No prior literature describes this type of bleeding without detectable ocular trauma.
Abstract
This paper provides the first reported case of acute posterior chamber hemorrhage during fluorescein angiography (FA). This is a case review with serial color photographs of the anterior segment. A 76-year-old male was referred for angiographic control of age-related macular degeneration. He was pseudophakic OU, BCVA 20/40 OU. He had mild hypertension, but not diabetes. He had had two previous angiograms without adverse effects. Difficulty was experienced in obtaining the images owing to a progressive reduction in the transparency of the media. A dense hemorrhage in the posterior chamber of the right eye was found, involving the visual axis. Thorough biomicroscopy, gonioscopy, and ultrasonic biomicroscopy showed that part of one of the haptics of the right intraocular lens (IOL) was touching and tearing the posterior face of the iris, without any visible synechiae, iris, or angle…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
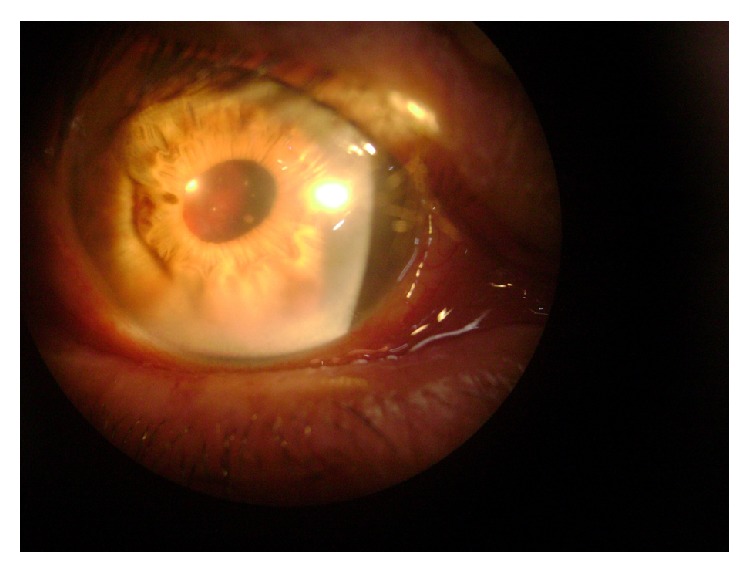 Figure 1
Figure 1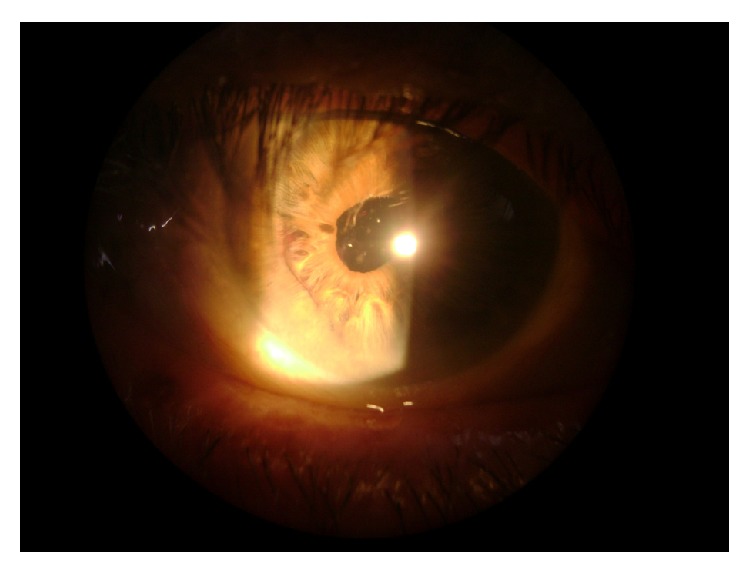 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Intraocular Surgery and Lenses · Retinal and Macular Surgery
1. Introduction
Fluorescein angiography (FA) is a very safe procedure, with infrequent complications and low morbidity [1–4]. Besides the expected effects of fluorescein injection (e.g., impregnation of the skin and urine, sneezing, and metallic taste), other reactions that require immediate treatment may occur. The most common ones are mild nausea (0.8%–15%) and vomiting (1%–4%); moderate reactions include urticaria (1.2%) and syncope (0.29%); severe reactions like anaphylactic shock, hypotension, respiratory failure, pulmonary edema, seizures, cardiovascular collapse, and arrhythmias are reported in 0.02 to 0.007% of cases. Death due to the procedure is estimated to happen in 0.00045% of cases (1 : 49557–221781). There are no reports in the literature of severe ocular adverse effects related to this procedure. We report a case of atypical posterior chamber hemorrhage immediately following FA.
2. Case Report
A 76-year-old male was referred for angiographic control of age-related macular degeneration. He was pseudophakic in both eyes (OU) (since 2007—phacoemulsification with foldable implant, “clear cornea” technique), having best corrected visual acuity (BCVA) 20/40 OU and intraocular pressure (IOP) 11 mmHg OU. He had mild hypertension. He had had two previous angiograms without complications. In November 2009 he underwent FA at our clinic, following pupil dilation using tropicamide 1% plus 2.5% phenylephrine solution (3 instillations 30 minutes before the procedure). Before the photos were taken, he complained of floaters in the right eye (RE). Difficulty was experienced in obtaining the images owing to a progressive reduction in the transparency of the media. The images obtained during the procedure showed great confluence of drusen in the posterior pole of the right eye, with no signs of papillary, retinal, or choroidal neovascularization. Owing to the worsening of symptoms he was reexamined before leaving the clinic. A dense hemorrhage in the posterior chamber of the right eye was found, enveloping the visual axis (Figure 1). Bed rest with raised head, bilateral eye occlusion, and topical corticosteroids were prescribed. He was seen 48 hours later, when eye examination showed reabsorption of most of the blood, thus releasing the optical axis (Figure 2). His visual acuity had returned to prior values. He was submitted to thorough biomicroscopy, gonioscopy, and ultrasonic biomicroscopy (UBM), which showed that part of one of the haptics of the right intraocular lens (IOL) was touching and tearing the iris, without any visible synechiae, iris, ciliary body lesion, or angle neovascularization. The corneal incision had no abnormal vessels either. It was impossible to rule out any adhesive focus between the lens capsular bag and the posterior iris. Anterior segment FA and posterior ultrasonography were normal.
3. Discussion
We found no similar case in the literature involving dense progressive bleeding located in the capsular bag and posterior chamber, without any detectable triggering ocular event other than mydriasis and fluorescein injection. Intraocular hemorrhage months or years after cataract surgery has been described as SWAN syndrome, in which stromal vascular growth is detectable and produces recurrent bleeding approximately 36–48 months after surgery [5]. However, this does not seem to be the case here. Another possibility is that it may have originated in the ciliary body [6, 7], but gonioscopy and UBM were entirely normal. We suppose that the ocular hemorrhage this patient presented was due to pharmacologic mydriasis and not to fluorescein, but its cause remains uncertain, considering that the patient had had his pupils dilated many times before with no adverse effects. Contact of the posterior face of the iris or sulcus with a portion of the intraocular lens, aggravated by the intense use of mydriatics during the FA procedure, probably caused bleeding rather than this being related to fluorescein injection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Butner R. W.Mc Pherson A. R.Adverse reactions in intravenous fluorescein angiography Annals of Ophthalmology 19831511108410862-s 2.0-00210597136651146 · pubmed ↗
- 2Yannuzzi L. A.Rohrer K. T.Tindel L. J.Fluorescein angiography complication survey Ophthalmology 198693561161710.1016/S 0161-6420(86)33697-22-s 2.0-00224819673523356 · doi ↗ · pubmed ↗
- 3Kwiterovich K. A.Maguire M. G.Murphy R. P.Frequency of adverse systemic reactions after fluorescein angiography: results of a prospective study Ophthalmology 19919871139114210.1016/s 0161-6420(91)32165-12-s 2.0-00260029051891225 · doi ↗ · pubmed ↗
- 4Kwan A. S. L.Barry C.Mc Allister I. L.Constable I.Fluorescein angiography and adverse drug reactions revisited: the Lions Eye experience Clinical and Experimental Ophthalmology 2006341333810.1111/j.1442-9071.2006.01136.x 2-s 2.0-3364492671216451256 · doi ↗ · pubmed ↗
- 5Swan K. C.Late hyphema due to wound vascularization Transactions. Section on Ophthalmology. American Academy of Ophthalmology and Otolaryngology 1976811 OP 138OP 1441274035 · pubmed ↗
- 6Foroozan R.Tabas J. G.Moster M. L.Recurrent microhyphema despite intracapsular fixation of a posterior chamber intraocular lens Journal of Cataract and Refractive Surgery 20032981632163510.1016/S 0886-3350(03)00122-62-s 2.0-004285811612954319 · doi ↗ · pubmed ↗
- 7Magargal L. E.Goldberg R. E.Uram M.Gonder J. R.Brown G. C.Recurrent microhyphema in the pseudophakic eye Ophthalmology 198390101231123410.1016/s 0161-6420(83)34396-72-s 2.0-00206166666686317 · doi ↗ · pubmed ↗