Giant Cervicothoracic Madelung Disease Presenting with Airway Compromise: A Case Report from Ethiopia
Amanuel Mesfin Oljira, Obsa Biratu Negasa, Diriba Gebeyehu Wakesa, Sinbona Ararsa Keneni, Berhanu Nigusse Bikila, Chala Abdo Dammesa, Tesfaye Hurgesa Bayisa, Rabirra Waktola Gonfa, Osman Aman Hamido, Dereje Gurmessa Geleta

TL;DR
A rare case of Madelung disease in Ethiopia caused severe breathing issues, and a two-stage surgery helped manage the condition safely.
Contribution
A reproducible peri-operative strategy for managing giant cervicothoracic Madelung disease in resource-limited settings is introduced.
Findings
Awake fiberoptic intubation and staged debulking surgery safely managed airway compromise.
The patient showed significant improvement in breathing and daily functioning with no early recurrence.
Long-term follow-up is essential due to the risk of postoperative recurrence.
Abstract
To describe a rare (airway-threatening) cervicothoracic presentation of Madelung disease (multiple symmetric lipomatosis) with upper mediastinal extension and to introduce a reproducible peri-operative strategy in a resource-limited setting. We report a case of a 40-year-old Oromo Ethiopian male who presented with progressive cervicothoracic adipose masses resulting in dyspnea and venous congestion. Awake fiberoptic intubation, staged resection, early extubation, and close airway management were the hallmarks of peri-operative management. Contrast-enhanced CT showed non-encapsulated, diffuse adipose infiltration from the neck into the upper mediastinum with effacement of the trachea. Because extensive bilateral cervical dissection posed a high risk of postoperative airway compromise (edema/hematoma) and prolonged anesthesia, a pre-planned two-stage surgical strategy was chosen. Stage 1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1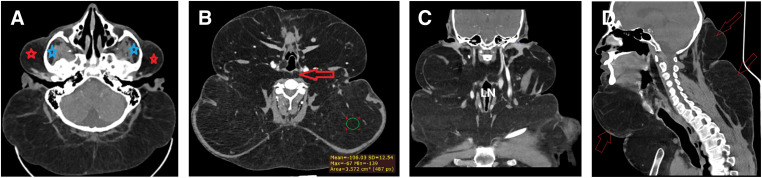 Fig. 2
Fig. 2 Fig. 3
Fig. 3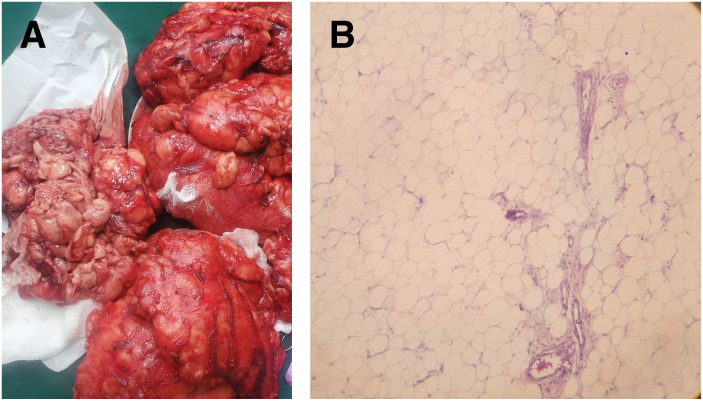 Fig. 4
Fig. 4 Fig. 5
Fig. 5| Timepoint | Symptoms & signs | Key clinical events | Management | Outcome/notes |
|---|---|---|---|---|
| 20 years before admission | Regular alcohol consumption; no MD symptoms | Risk factor acknowledged; later counseled to stop alcohol | ||
| 10 years before admission | Gradual neck enlargement; no dyspnea initially | Slow progression | ||
| 3–2 years before admission | Increasing bulk; cosmetic concerns; exertional breathlessness | Functional impact emerges | ||
| 6–3 months before admission | Worsening dyspnea (supine), reduced neck mobility, venous fullness | Preoperative surgical and anesthesia evaluation | Preoperative planning for anticipated difficult airway and staged surgery | Supine intolerance noted |
| Admission | Marked cervicothoracic enlargement; positional dyspnea | CT confirmed diffuse non-encapsulated fat with upper mediastinal extension and tracheal effacement; ASA III | Planned awake fiberoptic nasotracheal intubation and staged debulking | Anticipated difficult airway |
| D0 | Dyspnea and compressive symptoms | Awake fiberoptic nasotracheal intubation; anterior debulking | Excision ~3.5 kg; EBL 500 mL; 1 unit PRBC transfused intraoperatively; Penrose drain | Mild transient stridor treated with nebulization; ICU/HDU monitoring |
| D+1 to D+2 | Improving breathing | Postoperative monitoring | Penrose drain output ~80 mL hemorrhagic over 2 days | Drain removed on POD 2 |
| D+7 | Residual posterolateral/posterior bulk | Second-stage debulking | Additional ~2.0 kg excised; EBL 300 mL; Penrose drain | Uneventful recovery |
| Post-op day 1–2 | Stable | Postoperative monitoring | Penrose drain output ~50 mL over 2 days | Drain removed on POD 2 |
| Discharge | Improved breathing and function | Discharged one week after Stage 2 | Counseling on recurrence and strict alcohol cessation | Stable |
| 1 month | Marked functional and cosmetic improvement | Outpatient review | Continued counseling | No early recurrence |
| 3 months | No symptoms | Clinical + US follow-up | Surveillance | No recurrence/complications |
| 6 months | No symptoms | Clinical + US follow-up | Surveillance | No recurrence/complications |
| 9 months | No symptoms | Clinical + US follow-up | Surveillance | No recurrence/complications |
| 1 year | No symptoms | Clinical + US follow-up | Surveillance | No recurrence/complications; patient remained abstinent from alcohol |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBody Contouring and Surgery · Lymphatic Disorders and Treatments · Diagnosis and Treatment of Venous Diseases
Abbreviations
ASA American Society of Anesthesiologists EBL estimated blood loss ETT endotracheal tube HDU high-dependency unit IHC immunohistochemistry IV intravenous PRBC packed red blood cells
INTRODUCTION
Madelung disease (multiple symmetric lipomatosis; Launois–Bensaude syndrome) is a rare form of lipodystrophy characterized by diffuse, symmetric, non-encapsulated fatty deposits involving mainly the neck, shoulders, and upper trunk. It predominantly affects middle-aged men, and chronic alcohol consumption is frequently associated.^1–3)^
CT and MRI play a central role in diagnosis and pre-operative planning by delineating the extent, symmetry, and relationship to aerodigestive structures.^4,5)^ Cervicothoracic involvement can cause airway, esophageal, or venous compression requiring multispecialty management and sometimes urgent airway intervention.^6)^
We present a case of a giant cervicothoracic presentation with airway compromise successfully managed with awake fiberoptic intubation and staged surgical debulking, focusing on peri-operative steps practical in resource-limited settings.
CASE PRESENTATION
A 40-year-old Ethiopian male presented with a 10-year history of progressive neck mass extending anteriorly and posteriorly to the chest wall. Associated symptoms included dyspnea, functional limitation, and cosmetic deformity. The patient has admitted to habitual intake of alcohol over the past 20 years. Examination documented a giant circumferential cervicothoracic mass with a maximum neck circumference of 105 cm and venous congestion suggestive of superior mediastinal extension (Fig. 1A; Table 1).
Giant circumferential cervicothoracic mass. (A) Lateral view. (B) Supine anteroposterior view with a nasotracheal tube in place.
Contrast-enhanced CT of the neck and upper chest showed large, non-encapsulated fat tissue filling the cervicothoracic region and spreading to the retrosternal/upper mediastinal spaces with tracheal effacement (Fig. 2). Imaging findings were consistent with Madelung disease and guided surgical planning.
Neck CT scan. (A) Axial view at the level of the posterior fossa showing extensive non-encapsulated subcutaneous fat deposition extending bilaterally to parotid (red asterisks) and masticator spaces (blue asterisks). (B) Axial view at the level of the larynx showing fat deposition deep to sternocleidomastoid muscles bilaterally and in the prevertebral space (red arrow). (C) Post-contrast coronal view showing extensive non-encapsulated subcutaneous fat deposition. (D) Sagittal view showing anterior and posterior neck involvement with posterior “buffalo hump” appearance (red arrows).
Given the anticipated difficult airway due to the cervicothoracic mass effect, the patient was classified as ASA III. After counseling and written informed consent, awake fiberoptic intubation was planned.
The patient was placed sitting due to dyspnea in the supine position. Standard monitoring and supplemental oxygen were provided. Airway topicalization included nebulized lidocaine (4 mL of 2%), gargling of viscous lidocaine, nasal mucosa desensitization using lidocaine–adrenaline spray, and 0.2 mg of glycopyrrolate IV to reduce secretions. Sedation consisted of 1 mg of midazolam IV. A flexible fiberoptic bronchoscope guided placement of a 6.5-mm ETT via the nasal cavity under direct visualization (Fig. 1B). After securing the airway, the patient was repositioned supine with a shoulder roll and neck extension for surgery. General anesthesia was initiated with propofol (2 mg/kg) and fentanyl (2 μg/kg), maintained with isoflurane and IV analgesics.
Surgical management (two-stage strategy)
The procedure was pre-planned as two stages to reduce postoperative airway risk (edema/hematoma) after extensive bilateral cervical dissection, avoid prolonged anesthesia, improve hemostatic control, and address multi-compartment disease systematically. A 1-week interval was chosen to permit edema resolution, confirm airway stability, and allow recovery before the second stage.
Stage 1 (anterior debulking): A transverse cervical collar (apron-type) incision was used. Dissection proceeded in the subplatysmal plane and along cervical fascial planes with early identification and protection of the carotid sheath; the trachea and esophagus were visualized and preserved using careful blunt and sharp dissection. Hemostasis used monopolar cautery (superficial), bipolar cautery (near vital structures), and suture ligatures for larger vessels, with frequent hemostatic checks; diluted adrenaline-containing local anesthetic infiltration was used to reduce bleeding.
Meticulous debulking removed approximately 3.5 kg of lipomatous tissue invading the strap muscles and surrounding the carotid sheath, trachea, and esophagus (Fig. 3). EBL was 500 mL, and 1 unit of PRBC was transfused intraoperatively during stage 1. A Penrose drain was placed; drain output was hemorrhagic, totaling ~80 mL over 2 days, and it was removed on POD 2. Extubation was performed after full awakening and reversal; 6 mg of dexamethasone IV was administered prior to extubation, and airway equipment was prepared for reintubation. The patient developed a mild transient stridor, was treated with nebulization (dexamethasone 6 mg + adrenaline 1 mg), and was monitored in ICU/HDU, remaining stable.
Intraoperative picture showing adipose tissue dissection in the anterior neck with preservation of vital structures.
Stage 2 (posterolateral/posterior debulking; 1 week later): A further 2.0 kg of adipose tissue was removed from the lateral and posterior compartments of the neck. EBL was 300 mL. A Penrose drain was used again; output totaled ~50 mL over 2 days and was removed on POD 2. Recovery was smooth, and the patient was discharged 1 week after the second procedure.
Pathology
The final biopsy showed lobules of mature adipose tissue with benign mature adipocytes and areas of fibrous tissue with a well-delineated margin but without a capsule. No nuclear atypia, lipoblasts, or necrosis were identified, and IHC was not available (Fig. 4).
Histology of the resected adipose tissue. (A) Gross specimen showing non-encapsulated adipose tissue. (B) Microscopy showing lobules of mature adipose tissue composed of benign mature adipocytes.
Follow-up
At 1 month, the patient reported significant improvement in breathing and ADL with marked cosmetic improvement and no early recurrence (Table 1; Fig. 5). He was explicitly counseled about recurrence risk and counseled to stop alcohol; he stopped alcohol consumption postoperatively. Follow-up at 3, 6, and 9 months and 1 year (clinical and US-based) demonstrated no recurrence or complications.
Postoperative picture showing reduced neck mass.
DISCUSSION
Madelung disease involves symmetric, non-encapsulated adipose deposition classically in the cervicothoracic distribution (Type I/Enzi pattern). Long-term alcohol use is frequently associated, although causality is uncertain.^1–3)^ A systematic review highlights hypotheses including catecholamine-related lipolytic pathway defects and mitochondrial dysfunction and recommends alcohol cessation as part of comprehensive management because alcohol may aggravate progression.^1)^ In our patient, alcohol cessation was achieved postoperatively, and recurrence counseling was explicitly provided.
CT/MRI defines the extent and relationship to airway/vascular structures and helps distinguish Madelung disease from liposarcoma, Dercum disease, familial multiple lipomatosis, and other lipodystrophies.^4,5)^
Surgery (open debulking or liposuction) remains the mainstay when compression or disfigurement is significant. Recurrence after surgery is reported; a systematic review found an overall recurrence of approximately 18%.^1)^ A recent case series advocates staged excision and careful intraoperative management to optimize outcomes and reduce bleeding/complications.^7)^ In our patient, the two-stage plan was pre-planned to mitigate airway/hematoma risk and limit operative stress per session, with structured follow-up to 1 year showing no recurrence.
For airway-threatening cervicothoracic disease, awake fiberoptic intubation preserves spontaneous ventilation and visualization, reducing induction risk. ASA guidance emphasizes preoxygenation, continuous oxygen delivery, and extubation planning with readiness for reintubation.^8)^ In resource-limited settings without advanced rescue devices, explicit backup planning and multidisciplinary readiness are critical. Feasibility protocols and training-based approaches support consistent performance of awake fiberoptic techniques.^9,10)^
Pathologic differentiation: The benign histology (mature adipocytes without atypia, lipoblasts, or necrosis) supports Madelung disease rather than well-differentiated liposarcoma; in settings where available, IHC (e.g., MDM2/CDK4) may help exclude malignancy when morphology is equivocal. IHC was not available in our setting.
CONCLUSION
Giant cervicothoracic Madelung disease may result in life-threatening airway compromise. In this patient, an approach of awake fiberoptic intubation with staged debulking achieved excellent early functional improvement and sustained benefit. Detailed reporting of airway and operative steps may help teams in resource-constrained environments manage rare high-risk cervicothoracic lipomatosis. Long-term surveillance (≥12 months) is recommended given documented recurrence risk, and our patient remained recurrence-free at 1 year with clinical and US follow-up.
Patient perspective
“I am happy with the cosmetic result and the breathing and daily activities have improved markedly.”
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu Q, Lyu H, Xu B, et al. Madelung disease epidemiology and clinical characteristics: a systemic review. Aesthetic Plast Surg 2021; 45: 977–86.33492475 10.1007/s 00266-020-02083-5 · doi ↗ · pubmed ↗
- 2Hu HH, Liu CC, Li JH. Madelung disease. JAMA Dermatol 2024; 160: 1355–6.39504012 10.1001/jamadermatol.2024.4217 · doi ↗ · pubmed ↗
- 3Di Muzio B, Walizai T, Baba Y, et al. Madelung disease. Radiopaedia.org 2010: 12161.
- 4Kang HJ, Lee IS, Cha WJ, et al. Imaging features of Madelung’s disease: case report. Investig Magn Reson Imaging 2015; 19: 122–6.
- 5Williams DW 3rd, Ginsberg LE, Moody DM, et al. Madelung disease: MR findings. AJNR Am J Neuroradiol 1993; 14: 1070–3. https://www.ajnr.org/content/14/5/1070.8237682 PMC 8332758 · pubmed ↗
- 6Gijón de la Santa L, Pérez Retortillo JA, Arroyo Pérez FJ. Madelung disease. Eurorad 2012: 10297.
- 7Łącka M, Wojciechowska J, Bernecka P, et al. Madelung’s disease -a case series from a single-center experience. Front Surg 2025; 12: 1636822.41113128 10.3389/fsurg.2025.1636822 PMC 12528106 · doi ↗ · pubmed ↗
- 8Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022; 136: 31–81.34762729 10.1097/ALN.0000000000004002 · doi ↗ · pubmed ↗