Consideration of spatial companion biomarkers for targeted therapeutics in cancer: depatuxizumab mafodotin in glioblastoma
Rimas V. Lukas, Ruochen Du, Harrshavasan Congivaram, Kathleen McCortney, Karan Dixit, Craig Horbinski, Margaret Schwartz, Raymond Lezon, Lauren Singer, Ditte Primdahl, Jigisha Thakkar, Amy B. Heimberger, Roger Stupp, Priya Kumthekar

TL;DR
This study investigates how EGFR expression in glioblastoma tumors affects treatment outcomes with depatuxizumab mafodotin.
Contribution
The study explores the use of EGFR as a spatial companion biomarker for targeted cancer therapy in glioblastoma.
Findings
The relationship between tumor EGFR expression and outcomes was explored in glioblastoma patients.
Depatuxizumab mafodotin was evaluated in an expanded access program for progressive glioblastoma.
Abstract
An expanded access program of depatuxizumab mafodotin for patients with progressive glioblastoma explores the relationship between tumor EGFR expression and outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
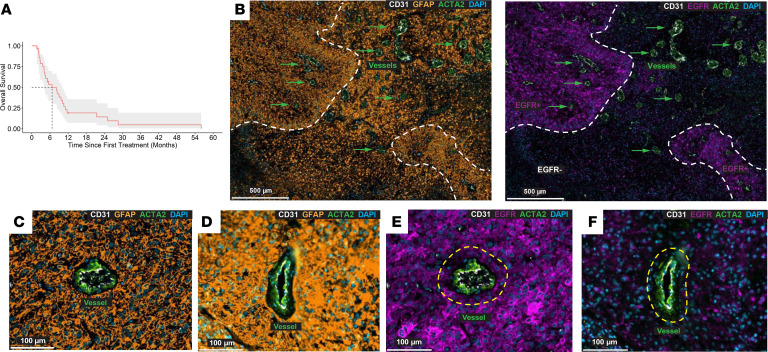 Figure 1
Figure 1- —National Cancer Institutehttps://doi.org/10.13039/100000054
- —AbbViehttps://doi.org/10.13039/100006483
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Cell Adhesion Molecules Research · Angiogenesis and VEGF in Cancer
To the Editor: Glioblastoma is a malignant primary central nervous system tumor with frequent epidermal growth factor receptor (EGFR) pathway aberrancies, including amplification and/or mutation of the EGFR gene and overexpression of the cell surface receptor, thereby serving as an enticing target in those tumors where these aberrancies are detected. In newly diagnosed glioblastoma, EGFR amplification is present in approximately 50% of glioblastomas, with concurrent expression of tumor-specific mutant EGFRvIII in approximately half of amplified cases (1), with a less clear understanding of its aberrations in progressive tumors. Unfortunately, targeting EGFR has been unsuccessful thus far (2). The EGFR-targeting antibody-drug conjugate, depatuxizumab mafodotin (ABT-414), is composed of a humanized chimeric recombinant IgG1 κ EGFR-specific antibody attached to the antimitotic cytotoxic monomethylauristatin F via a maleimidocaproyl linker. ABT-414 can toggle binding to activated, amplified wild-type EGFR or EGFRvIII, rendering it tumor preferential but not specific. A phase III trial for EGFR-amplified newly diagnosed glioblastoma added ABT-414 to radiotherapy and temozolomide. Progression-free survival (PFS) was longer, but with no increase in survival (3).
Spatial localization of EGFR relative to the site of vascular entry into the tumor has not been previously considered. There is marked tumor heterogeneity in vascular size and distribution within glioblastomas. Intravenously administered antibodies, as a function of molecular weight and tissue flow kinetics, have limited diffusion. Furthermore, longitudinal loss of EGFRvIII expression contributes to lack of therapeutic effects for peptide vaccines and chimeric antigen receptor T cell strategies.
Using a single institutional expanded access program (EAP) of ABT-414 approved by the IRB at Northwestern University (NU17CU02, NCT03123952; see the “Summarized inclusion criteria” and “Expanded Access Protocol” in the supplemental material; supplemental material available online with this article; https://doi.org/10.1172/jci.insight.198475DS1), analysis was conducted on spatial heterogeneity of EGFR relative to vasculature in progressive glioblastoma. ABT-414 (1.25 mg/kg i.v.) was administered every 2 weeks as long as tolerated and efficacious. The EAP allowed for ABT-414 in combination with additional FDA-approved glioblastoma treatments, providing real-world experience.
Twenty-nine heavily pretreated patients (Supplemental Table 1) were enrolled in the EAP with a median age of 55 years (36–68 years), majority male (n = 20, 69%) and White (n = 26, 90%). Patients were treated with ABT-414 monotherapy (n = 13), or in combination with temozolomide (n = 7), CCNU (n = 3), bevacizumab (n = 3), temozolomide plus bevacizumab (n = 2), and temozolomide plus tumor-treating fields (n = 1). Participants received between 1 (n = 10 patients) and 44 doses, with 24% receiving 20 or more doses of ABT-414. Most (n = 28, 97%) developed treatment-related adverse events (AEs). Grade 3/4 AEs were common (n = 22, 76%), and one grade 5 AE (3%) was observed. The most common treatment-related AEs were thrombocytopenia (66%) and blurred vision (35%), aligning with what has been previously reported. No new unexpected AEs were identified, indicating that the experience with ABT-414 for patients with recurrent glioblastoma within an EAP demonstrated toxicity similar to what has been observed in previously published trials.
Of 29 patients treated, 23 were evaluable for radiographic responses. No responses were observed. Approximately half (n = 11, 48%) demonstrated stable disease, while the other half (n = 12, 52%) had progressive disease. Median survival was 6.7 months (95% CI, 4.07–10.2 months) (Figure 1A) and median PFS was 2.4 months (95% CI, 1.9–5.6 months) (Supplemental Figure 1).
Ad hoc retrospective analysis of spatial EGFR expression was performed on a subset of patients for whom the original resection blocks could be obtained (Supplemental Dataset 1). Cell segmentation, background autofluorescence subtraction, and thresholding were conducted using an established bioinformatic pipeline analysis. EGFR expression was heterogeneous, including tumor regions devoid of expression (Figure 1B). Total expression at the time of the initial diagnosis was in the range of 11%–91% (n = 6) and did not associate with PFS. GFAP^+^ tumor cells abutted vasculature but also extended far into the parenchyma (Figure 1, C and D). In some instances, GFAP^+^ tumor cells surrounding the vasculature were EGFR^+^ (Figure 1E), whereas other perivascular regions lacked EGFR expression (Figure 1F), indicating tumor cells would persist even in the presence of an EGFR-targeting moiety administered intravenously. Presence of EGFR^+^ tumor cells adjacent to the vasculature was not associated with PFS (Supplemental Figure 2).
Antibody penetration distance is limited by clearance and antigen turnover rate. For a 70 kg patient with blood volume of 5.5 L, the circulating concentration of ABT-414 would be approximately 110 nM (roughly 1 × 10^–7^ mol/L), corresponding to an estimated penetration distance of approximately 15–40 μm, depending on EGFR turnover (4, 5). Spatial quantification analysis using a diffusion penetration distance of 40 μm indicates only 24%–68% of total cells would be in range of a vessel to have been exposed to ABT-414 (n = 6). This level of cytotoxicity is likely well below the threshold needed to impact survival for glioblastoma. These findings illustrate that dichotomized readouts for biomarkers are insufficient in heterogeneous diseases and that companion biomarkers should consider spatial target expression and antibody distribution. Selection of highly vascular tumors and/or delivery strategies, including blood-brain barrier opening ultrasound and convection-enhanced delivery, could address therapeutic tumor distribution. Additionally, antibody-drug conjugates developed with cleavable linkers (unlike ABT-414) could mediate bystander via release of payload, leading to improved penetration distance and potentially improved potency. However, uniform target expression remains a continued challenge for many solid cancers. Whether the resected tumor is reflective of the residual/progressive disease state during treatment is a significant knowledge gap needing to be addressed, especially for targeted therapy strategies.
Funding support
This work is the result of NIH funding, in whole or in part, and is subject to the NIH Public Access Policy. Through acceptance of this federal funding, the NIH has been given a right to make the work publicly available in PubMed Central.
Supplementary Material
Supplemental data
Supplemental data set 1
undefined
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heimberger AB et al Prognostic effect of epidermal growth factor receptor and EGF Rv III in glioblastoma multiforme patients Clin Cancer Res 20051141462146610.1158/1078-0432.CCR-04-173715746047 · doi ↗ · pubmed ↗
- 2Weller M et al Rindopepimut with temozolomide for patients with newly diagnosed, EGF Rv III-expressing glioblastoma (ACT IV): a randomised, double-blind, international phase 3 trial Lancet Oncol 201718101373138510.1016/S 1470-2045(17)30517-X 28844499 · doi ↗ · pubmed ↗
- 3Lassman AB et al Depatuxizumab mafodotin in EGFR-amplified newly diagnosed glioblastoma: a phase III randomized clinical trial Neuro Oncol 202325233935010.1093/neuonc/noac 17335849035 PMC 9925712 · doi ↗ · pubmed ↗
- 4Thurber GM et al Theoretic criteria for antibody penetration into solid tumors and micrometastases J Nucl Med 200748699599910.2967/jnumed.106.03706917504872 · doi ↗ · pubmed ↗
- 5Greig MJ et al Effects of activating mutations on EGFR cellular protein turnover and amino acid recycling determined using SILAC mass spectrometry Int J Cell Biol 2015 201579893610.1155/2015/79893626689952 PMC 4672139 · doi ↗ · pubmed ↗