Genetic evidence for GLP1R agonists in non-ischaemic heart failure
Nhu Ngoc Le, Dipender Gill, Sandosh Padmanabhan

TL;DR
Genetic evidence suggests that GLP1R agonists may protect against non-ischaemic heart failure, especially in preserved ejection fraction cases, beyond their effects on blood sugar and weight.
Contribution
This study provides genetic evidence that GLP1R activation reduces heart failure risk independently of glycaemic control and BMI reduction.
Findings
Genetically proxied GLP1R activation was associated with lower risk of non-ischaemic heart failure and HFpEF.
The protective effects of GLP1R activation were greater than those expected from glycaemic lowering alone.
Associations for ni-HFrEF were not significant, and AF showed a nominal association driven by BMI-related genetic variants.
Abstract
Glucagon-like peptide-1 receptor (GLP1R) agonists reduce cardiovascular events in patients with obesity and diabetes, and recent trials demonstrate symptomatic and functional benefits in heart failure with preserved ejection fraction (HFpEF). Whether these benefits reflect glycaemic control, weight reduction, or additional mechanisms remains uncertain. We performed drug-target Mendelian randomization (MR) using genetic variants in the GLP1R-locus to proxy GLP1R activation. MR estimates for GLP1R agonism were scaled to per 0.1 log-odds lower liability to type 2 diabetes (T2DM) and compared with general type 2 diabetes (T2DM) or body mass index (BMI) lowering effects. Summary statistics were obtained from the largest available GWAS of HF, non-ischaemic HF (ni-HF), ni-HFpEF, ni-HFrEF, and atrial fibrillation (AF). Primary inverse-variance weighted analysis was adjusted for multiple…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
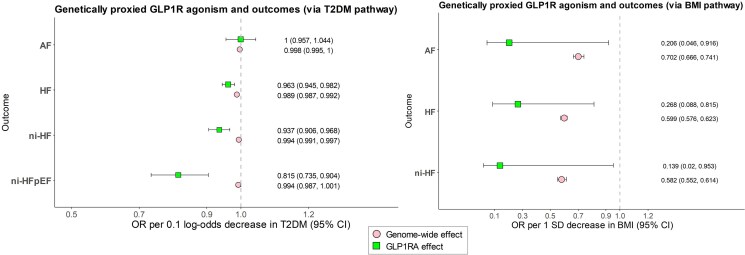 Figure 1
Figure 1- —British Heart Foundation Centre of Excellence
- —United Kingdom Research and Innovation Strength in Places Fund
- —Pontecorvo Chair of Pharmacogenomics endowment
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Diabetes, Cardiovascular Risks, and Lipoproteins · Pancreatic function and diabetes
Background
Heart failure (HF) is a major cause of morbidity and mortality, with limited therapies targeting HF with preserved ejection fraction (HFpEF), a major subtype that is frequently non-ischaemic. Glucagon-like peptide-1 receptor (GLP1R) agonists reduce cardiovascular events in obesity and diabetes, and recent trials demonstrate symptomatic and functional benefits in HFpEF.^1^ Whether these effects arise predominantly through glycaemic control, weight reduction, or additional mechanisms remains uncertain. Mendelian randomization (MR) provides an opportunity to test causal effects of genetically proxied GLP1R activation on HF outcomes. Prior MR studies reported protective associations but used scaling that limited clinical interpretability,^2^ highlighting the need for clarification.
Aims
We aimed to evaluate the causal relationship between GLP1R activation and HF, including aetiological subtypes (non-ischaemic HF, HFpEF, and HFrEF), using drug-target MR. By scaling genetic estimates to clinically interpretable units and benchmarking against glycaemia and BMI instruments, we sought to bridge genetic target validation with clinical trial outcomes, provide HF subtype specificity, and clarify mechanistic pathways.
Methods
We constructed two sets of genetic instruments to proxy GLP1R agonism through distinct metabolic pathways.^3^ The first set comprised single-nucleotide polymorphisms (SNPs) within 100 kb GLP1R (GRCh38 chr6: 39 048 781–39 091 303), in low linkage disequilibrium (r^2^ < 0.1), associated with T2DM liability at genome-wide significance (P < 5 × 10^−8^) in a GWAS meta-analysis including 242 283 cases and 1 327 447 controls of European ancestry.^4^ To ensure biological relevance, variants were directionally concordant and nominally associated with HbA1c (P < .05).^5^ These instruments were scaled to per 0.1 log-odds lower T2DM liability, a clinically interpretable unit that avoids inflation from per 1 mmol/mol HbA1c reporting.
The second set includes SNPs associated with BMI in a GWAS meta-analysis of around 806 834 individuals of European ancestry.^6,7^ Although these summary statistics were released alongside studies of fat distribution, the instrument used here reflects BMI rather than waist-hip ratio. Because no GLP1R-proximal variants reached P < 5 × 10^−8^, we applied a less stringent threshold (P < 1 × 10^−6^), yielding a single cis variant. This locus-specific BMI instrument was therefore considered exploratory. For comparison, we also generated genome-wide instruments for overall T2DM liability and BMI using standard clumping (r^2^ < 0.001) to provide robust benchmarks.
Outcome summary statistics were obtained from the largest publicly available GWAS, predominantly of European ancestry, with sample sizes of 1 946 349 for HF and 1 030 836 for AF.^8,9^ Analyses covered overall HF, non-ischaemic HF (ni-HF), non-ischaemic HF with preserved ejection fraction (ni-HFpEF), non-ischaemic HF with reduced ejection fraction (ni-HFrEF), and atrial fibrillation (AF). The overall HF phenotype was defined as any diagnosis of HF, ascertained through physician adjudication, hospital record review, or diagnostic coding.^9^ All contributing studies had ethical approval and participant consent.
MR analyses were performed using inverse variance weighted (IVW) regression as the primary MR method, complemented by weighted median and MR Egger.^10,11^ Multiple testing was controlled with Benjamini–Hochberg FDR. Associations were considered significant at IVW P < .05 and q < 0.05, with nominal associations defined as P < .05 with q ≥ 0.05. To compare MR estimates for GLP1R agonism with general T2DM- or BMI-lowering effects, we scaled all estimates to a standard reference (0.1-logOR T2DM or 1-SD BMI decrease). Differences between drug-target and general effects were assessed using the propagation-of-error method to determine if the resulting contrast significantly differed from zero.^12^
All analyses used the TwoSampleMR package in R 4.2.3.
Results
Using instruments scaled to per 0.1 log-odds lower T2DM liability, genetically proxied GLP1R activation was associated with lower HF risk. Significant associations were observed for overall HF (OR 0.96; 95% CI 0.95–0.98; q < 0.05) and ni-HF [OR 0.94 (0.91–0.96); q < 0.05]. The largest effect was evident for ni-HFpEF [OR 0.82 (0.74–0.90); q < 0.05] (Figure 1). MR sensitivity analyses produced estimates of similar direction and magnitude, with no evidence of horizontal pleiotropy. Associations for ni-HFrEF were directionally adverse (OR > 1) but not statistically significant. Given the risk of collider bias from excluding antecedent ischaemic, valvular, and congenital disease in the ni-HFrEF phenotype,^9^ we performed MVMR adjusting for CAD liability; the GLP1R—ni-HFrEF association was still directionally adverse but non-significant (P > .05). No significant associations were observed between GLP1R agonism and AF using T2DM instruments.
MR estimates for genetically proxied GLP1R agonism via BMI and T2DM pathway, compared with general BMI and T2DM reduction. The left forest plot presents (i) MR estimates for genetically proxied GLP1R agonism via the T2DM pathway across outcomes and (ii) corresponding MR estimates for general genetically proxied T2DM lowering across outcomes. The right forest plot presents (i) MR estimates for genetically proxied GLP1R agonism via the BMI pathway across outcomes and (ii) corresponding MR estimates for general genetically proxied BMI lowering across outcomes. Differences between GLP1R-proxied and general T2DM-/BMI-lowering effects were assessed using the propagation-of-error method (Results)
The GLP1R-locus BMI instrument comprised a single SNP identified using a relaxed significance threshold. This variant yielded nominal associations with overall HF and AF but lacked statistical power, precluding robust sensitivity analyses. These findings are therefore considered exploratory and presented in Figure 1.
To contextualize the findings, we compared effect sizes of drug-target perturbation with those derived from genome-wide T2DM liability and BMI instruments (Figure 1). GLP1R-proxied effects exceeded those expected from glycaemic lowering alone [overall HF, beta difference & 0.27 (0.07–0.46), P & .007; ni-HF, 0.6 (0.26–0.94), P & .0004; ni-HFpEF, 1.98 (0.94–3.01), P & .0001]. The GLP1R-proxied effects were of comparable magnitude to those from BMI reduction [HF, 0.81 (−0.31–1.92), P & .16; ni-HF, 1.43 (−0.49–3.35), P & .15]. For AF, the magnitude of association was similar to that observed for BMI lowering, although this finding should be interpreted cautiously, given the exploratory nature of the analysis.
Collectively, the results indicate that GLP1R activation reduces risk of HF—particularly ni-HFpEF—with effect sizes that are clinically plausible and consistent with recent GLP1R trials in obesity and HFpEF. The absence of significant benefit in ni-HFrEF and the modest, BMI-consistent association with AF highlights heterogeneity across outcomes.
Conclusion
This genetic analysis provides support for a protective association between GLP1R activation and heart failure, with the strongest effects observed for non-ischaemic HFpEF when estimates are scaled to clinically interpretable units. Expressing effects per 0.1 log-odds lower liability to type 2 diabetes yields magnitudes consistent with contemporary GLP1R agonist trials in obesity and HFpEF.^1,13^ Our results suggest that the benefits of GLP1R activation extend beyond glycaemic lowering and are comparable to those expected from BMI reduction, implying an integrated cardio-metabolic profile that includes weight loss, improved haemodynamic, and anti-inflammatory mechanisms.^14^ Associations for non-ischaemic HFrEF were not statistically significant, consistent with heterogeneous and largely neutral trial evidence in this phenotype.^15^
Key limitations include limited generalizability beyond European ancestry populations, the lifelong nature of genetic proxies compared with pharmacological treatment, and the exploratory nature of BMI-mediated analyses based on single-variant instrumentation.
Overall, these findings complement emerging clinical trial data and support further evaluation of GLP1R agonism in cardio-metabolic HFpEF, including in high-risk populations without diabetes.
Supplementary Material
xvag077_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kosiborod MN, Deanfield J, Pratley R, Borlaug BA, Butler J, Davies MJ, et al Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-H Fp EF, and STEP-H Fp EF DM randomised trials. Lancet 2024;404:949–61. 10.1016/S 0140-6736(24)01643-X 39222642 · doi ↗ · pubmed ↗
- 2Daghlas I, Karhunen V, Ray D, Zuber V, Burgess S, Tsao PS, et al Genetic evidence for repurposing of GLP 1R (Glucagon-Like Peptide-1 Receptor) agonists to prevent heart failure. J Am Heart Assoc 2021;10:e 020331. 10.1161/JAHA.120.02033134184541 PMC 8403330 · doi ↗ · pubmed ↗
- 3Gill D, Vujkovic M. The potential of genetic data for prioritizing drug repurposing efforts. Neurology 2022;99:267–8. 10.1212/WNL.000000000020080335654591 · doi ↗ · pubmed ↗
- 4Suzuki K, Hatzikotoulas K, Southam L, Taylor HJ, Yin X, Lorenz KM, et al Genetic drivers of heterogeneity in type 2 diabetes pathophysiology. Nature 2024;627:347–57. 10.1038/s 41586-024-07019-638374256 PMC 10937372 · doi ↗ · pubmed ↗
- 5Chen J, Spracklen CN, Marenne G, Varshney A, Corbin LJ, Luan J, et al The trans-ancestral genomic architecture of glycemic traits. Nat Genet 2021;53:840–60. 10.1038/s 41588-021-00852-934059833 PMC 7610958 · doi ↗ · pubmed ↗
- 6Pulit SL, Stoneman C, Morris AP, Wood AR, Glastonbury CA, Tyrrell J, et al Meta-analysis of genome-wide association studies for body fat distribution in 694 649 individuals of European ancestry. Hum Mol Genet 2019;28:166–74. 10.1093/hmg/ddy 32730239722 PMC 6298238 · doi ↗ · pubmed ↗
- 7Pulit SL . 2018. Summary-level data from meta-analysis of fat distribution phenotypes in UK Biobank and GIANT. Zenodo. 10.5281/zenodo.1251813 · doi ↗
- 8Nielsen JB, Thorolfsdottir RB, Fritsche LG, Zhou W, Skov MW, Graham SE, et al Biobank-driven genomic discovery yields new insight into atrial fibrillation biology. Nat Genet 2018;50:1234–9. 10.1038/s 41588-018-0171-330061737 PMC 6530775 · doi ↗ · pubmed ↗