Tumor and germline testing with next generation sequencing in epithelial ovarian cancer: a prospective paired comparison using an 18‐gene panel
Elisabeth Spenard, Cristina Mitric, Melanie Care, Tracy L. Stockley, Raymond H. Kim, Jeanna McCuaig, Blaise Clarke, Laura Ranich, Clare Sheen, Sarah E. Ferguson, Liat Hogen, Taymaa May, Marcus Q. Bernardini

TL;DR
This study shows that testing tumor tissue first with an 18-gene panel can effectively identify genetic variants in ovarian cancer patients, reducing the need for duplicate germline testing.
Contribution
The study demonstrates the feasibility and accuracy of tumor-first multigene testing for germline variant detection in epithelial ovarian cancer.
Findings
Tumor-first testing detected germline pathogenic variants in 59% of identified tumor variants.
Only 1% of patients had a false-negative result for germline variants using tumor-first testing.
28% of BRCA-negative patients were homologous recombination deficiency (HRD)-positive.
Abstract
Genetic testing in epithelial ovarian cancer (EOC) in Ontario includes germline next‐generation sequencing (NGS) for 19 genes. Additionally, tumor tissue undergoes reflex NGS testing for BRCA1/2 to assess eligibility for PARPi. Although parallel testing confers advantages, this model duplicates healthcare resources. Here, we prospectively assessed the feasibility of tumor‐first multigene testing by comparing tumor tissue with germline testing of peripheral blood. An 18‐gene NGS panel was used to test tumor and germline DNA (n = 106 patients). In 26 patients, 27 tumor Tier I or II variants were identified, with 16/27 (59%) being germline pathogenic variants (PV) (13 BRCA1/2; 3 other genes) and 11/27 (41%) somatic variants (9 BRCA1/2; 2 other). In 51/106 patients, there were no tumor variants (excluding TP53), of which one patient had a germline BRCA1 copy number variant deletion in exon…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
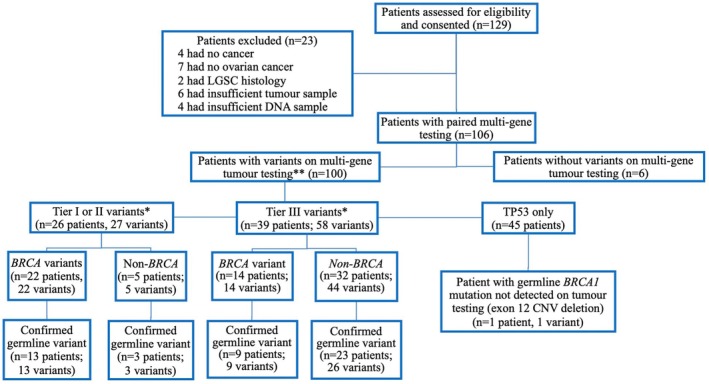 Fig. 1
Fig. 1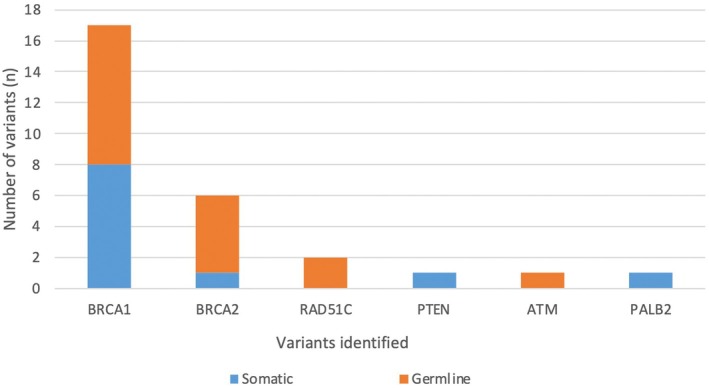 Fig. 2
Fig. 2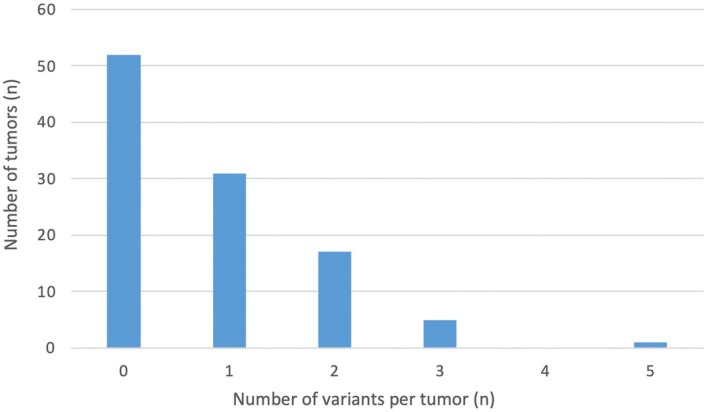 Fig. 3
Fig. 3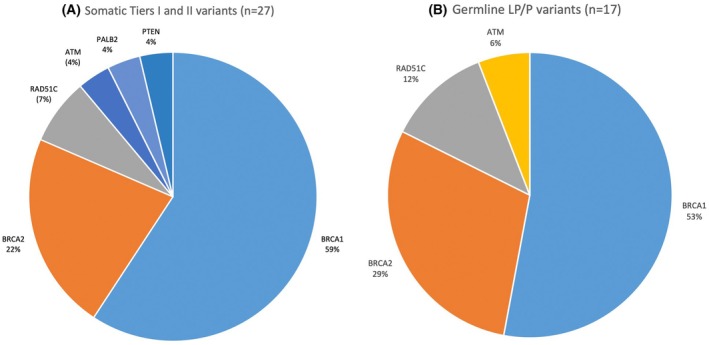 Fig. 4
Fig. 4| Patient characteristics |
|
|---|---|
| Age in years: median (range) | 63 (46–90) |
| Stage FIGO 2018: | |
| I–IIB | 5 (4.7%) |
| IIIB | 16 (15.1%) |
| IIIC | 49 (46.2%) |
| IVA | 14 (13.2%) |
| IVB | 22 (20.8%) |
| CA125 level: median (range) | 967 (20, 18 700) |
| ECOG status: | |
| 0 | 70 (66.7%) |
| 1 | 28 (26.7%) |
| 2 | 5 (4.7%) |
| 3 | 2 (1.9%) |
| First‐line treatment: | |
| Primary debulking surgery | 49 (46.2%) |
| Neoadjuvant chemotherapy, interval surgery | 33 (31.1%) |
| Neoadjuvant chemotherapy, no surgery | 22 (20.8) |
| Supportive care | 2 (1.9%) |
| Surgical outcome: | |
| Optimal (< 1 cm) | 72 (67.9%) |
| Suboptimal (> 1 cm) | 6 (5.7%) |
| Open and close | 4 (3.8%) |
| No surgery | 24 (22.6%) |
| Histology: | |
| High‐grade serous | 97 (91.5%) |
| Clear cell | 6 (5.7%) |
| Endometrioid | 2 (1.9%) |
| Other | 1 (0.9%) |
| Pathology sample: | |
| Biopsy | 74 (69.8%) |
| Primary debulking surgery | 28 (26.4%) |
| Interval debulking surgery | 4 (3.8%) |
| Family history of cancer: | 88 (83.0%) |
| Prior cancer history: | 17 (16.0%) |
| Patient # | HRD status | GIS score | NGS germline testing | NGS tumor‐testing (tier) | Variant (cDNA) | Variant (protein) | Tumor VAF (%) |
|---|---|---|---|---|---|---|---|
| 3 | Positive | 48 | Negative |
| c.388C>G | p. (Leu130Val) | 75.6 |
| 6 | Positive | 63 |
|
| c.53 T>C | p.(Ile18Thr) | 46.3 |
|
| c.517 T>C | p.(Val173Leu) | 61.4 | ||||
| 16 | Positive | 57 |
|
| c.976C>A | p. (Pro326Thr) | 51.4 |
|
| c.838delA | p.(Arg280Glufs*65) | 33.1 | ||||
| 23 | Positive | 51 |
|
| c.823C>T | p.(Arg275Trp) | 86.3 |
|
| c.2005 + 7A>T | p.(?) | 5.6 | ||||
|
| c.743G>A | p.(Arg248Gln) | 76.2 | ||||
| 26 | Positive | 72 |
|
| c.460A>C | p.(Asn154His) | 8.4 |
|
| NA | Full gene deletion | n/a | ||||
|
| NA | Full gene duplication | n/a | ||||
|
| 1025G>C | p.(Arg342Pro) | 77.5 | ||||
| 34 | Positive | 58 | Negative |
| c. 747G>T | p.(Arg249Ser) | 70.9 |
| 39 | Positive | 43 | Negative |
| NA | exon 1 deletion | n/a |
|
| NA | exon 2–15 duplication | n/a | ||||
|
| c.646G>A | p.(Val216Met) | 74.8 | ||||
| 50 | Positive | 75 |
|
| c.7435 + 1‐G>A | p.(?) | 47.9 |
|
|
| c.3760G>C | p.(Glu1254Gln) | 35.9 | |||
|
| c.714dupT | p.(Asn239 | 66.8 | ||||
| 57 | Positive | 59 | Negative |
| c.395A>G | p.(Lys132Arg) | 89.8 |
| 64 | Positive | 60 |
|
| c.2516A>G | p.(His839Arg) | 64.4 |
|
|
| c.107C>T | p.(Ala36Val) | 66.5 | |||
|
| c.375G>A | p.(Thr125Thr) | 57.2 | ||||
| 74 | Positive | 50 |
|
| c.421A>G | p.(Met141Val) | 58.4 |
|
| c.993 + 1G>A | p.(?) | 23.1 | ||||
| 79 | Positive | 55 | Negative |
| c.830G>T | p.(Cys277Phe) | 70.5 |
| 82 | Positive | 72 |
|
| c.571 + 4A>G | p.(?) | 56 |
|
| c.949C>T | p.(Gln317 | 17.5 | ||||
| 99 | Positive | 54 |
|
| c.706‐2A>G | p.(?) | 77.9 |
|
| c.920‐2A>G | p.(?) | 45.2 |
| Patient # | HRD status | GIS score | NGS germline testing | NGS tumor (tier) | Variant (cDNA) | Variant (protein) | Tumor VAF (%) |
|---|---|---|---|---|---|---|---|
| 4 | Negative | 1 | Negative |
| c.388C>G | p.(Arg273His) | 36.8 |
| 10 | Negative | 20 | Negative |
| c.4193A>T | p.(Asp1398Val) | 39.2 |
|
| NA | Whole gene deletion | n/a | ||||
| 13 | Negative | 12 |
|
| c.1127 T>G | p.(Phe376Cys) | 66 |
|
| c.488A>G | p.(Tyr163Cys) | 94 | ||||
| 14 | Negative | 21 | Negative |
| c.640delC | p.(His214Ilefs*33) | 36.1 |
| 19 | Negative | 40 |
|
| c.701C>G | p.(Ser234 | 83.9 |
|
| c.818G>A | p.(Arg273His) | 50.9 | ||||
| 22 | Negative | 9 | Negative |
| c.721dupT | p.(Ser241Phefs*23) | 62.8 |
| 37 | Negative | 23 |
|
| c.2296‐4A>G | c.2296‐4A>G | 9.7 |
|
| NA | Whole gene duplication | n/a | ||||
|
| c.713G>T | p.(Cys238Phe) | 80.3 | ||||
| 42 | Negative | 30 |
|
| c.9501 + 3A>T | p.(?) | 59.4 |
|
| NA | Whole gene duplication | n/a | ||||
|
| NA | Whole gene duplication | n/a | ||||
|
| NA | Whole gene deletion | n/a | ||||
|
| NA | Whole gene duplication | n/a | ||||
|
| c.734G>T | p.(Gly245Val) | 84.1 | ||||
| 43 | Negative | 34 | Negative |
| c.524G>A | p.(Arg175His) | 61.6 |
| 51 | Negative | 22 | Negative | Negative | — | — | — |
| 52 | Negative | 22 | Negative |
| c.524G>A | p.(Arg175His) | 94.7 |
| 61 | Negative | 41 | Negative |
| c.851_852delCA | p.(Thr284Argfs*21) | 53.3 |
| 63 | Negative | 10 | Negative |
| c.625A>T | p.(Arg209 | 35.2 |
| 65 | Negative | 21 |
|
| c.5278 T>G | p.(Ser1760Ala) | 45.2 |
| 68 | Negative | 17 | Negative |
| c.818G>A | p.(Arg273His) | 10.4 |
| 69 | Negative | 23 | Negative |
| c.841G>A | p.(Asp281Asn) | 78.7 |
| 80 | Negative | 21 | Negative |
| c.743G>A | p.(Arg248Gln) | 47.1 |
| 84 | Negative | 35 | Negative |
| c.818G>T | p.(Arg273Leu) | 38.3 |
| 87 | Negative | 22 | Negative | Negative | — | — | — |
| 88 | Negative | 29 | Negative |
| c.659A>G | p.(Tyr220Cys) | 73.3 |
| 90 | Negative | 12 | Negative |
| c.916C>T | p.(Arg306 | 58.5 |
| 92 | Negative | 15 | Negative |
| c.145delG | p.(Asp49Ilefs*74) | 56.5 |
| 95 | Negative | 15 |
|
| c.1567 T>A | p.(Ser523Thr) | 26.2 |
|
| c.723delC | p.(Cys242Alafs*5) | 31.1 | ||||
| 96 | Negative | 39 |
|
| c.6541G>C | p.(Gly2181Arg) | 56.4 |
|
| c.838A>G | p.(Arg280Gly) | 27.4 | ||||
| 97 | Negative | 12 |
|
| c.1903G>C | p.(Asp536His) | 6.8 |
|
| c.503A>G | p.(His168Arg) | 90.8 | ||||
| 98 | Negative | 16 | Negative |
| c.517G>T | p.(Val173Leu) | 13.1 |
| 101 | Negative | 24 | Negative |
| c.637C>T | p.(Arg213 | 52.4 |
| 102 | Negative | 36 | Negative |
| c.268delT | p.(Ser90Pro*33) | 24 |
| 103 | Negative | 22 | Negative |
| c.574C>T | p.(Gln192 | 54.2 |
| 105 | Negative | 10 | Negative |
| c.736A>G | p.(Met246Val) | 76.2 |
- —Surgical Oncology Innovations in Translational and Basic Science Research Grant from University Health Network, University of Toronto
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · PARP inhibition in cancer therapy · Cancer Genomics and Diagnostics
Introduction
1
Epithelial ovarian cancer (EOC) affects 1.5% of women and is the fifth leading cause of cancer death among females in North America [1, 2]. Genetic pathogenic variants (PV) are responsible for 20–30% of EOC, most commonly occurring in the BRCA1/2 genes [3, 4]. Other causative genes include those involved in mismatch repair (MLH1, MSH2, MSH6, PMS2, and EPCAM) or the Fanconi‐anemia pathway (RAD51C, RAD51D, BRIP1, and PALB2). Although PV in other genes such as ATM, CDH1, CHEK2, PTEN, and TP53 have been observed in families with ovarian cancer, this data remain controversial [5, 6].
Information about both somatic and germline status is relevant for patients and their families, as knowledge of BRCA1/2 status can impact treatment options. For instance, the use of poly ADP‐ribose polymerase inhibitors (PARPi) has been shown to significantly increase progression‐free and overall survival [7, 8, 9]. Similarly, knowledge about germline PV in EOC risk genes can provide cancer risk‐reduction and surveillance options for patients and their relatives [10, 11, 12]. Risk‐reducing bilateral salpingo‐oophorectomy can lead to a 90% decreased risk of EOC [11, 13]. Ovarian cancer patients with a germline BRCA1/2 mutation have a 50% chance of a first‐degree relative also having the mutation.
The current standard of care for genetic testing in EOC in Ontario includes germline next‐generation sequencing (NGS) genetic testing for 19 genes including ATM, BARD1, BRCA1, BRCA2, BRIP1, CDH1, CHEK2, EPCAM, MLH1, MSH2, MSH6, PALB2, PMS2, PTEN, RAD51C, RAD51D, HOXB13, STK11, and TP53 [14]. In addition, tumor tissue from all EOC patients undergoes reflex testing for BRCA1/2 to assess eligibility for PARPi [14]. For BRCA1/2, it is known that approximately 5–7% of EOC have acquired somatic PVs present only in tumor tissue, which cannot be detected through germline testing [7, 8]. To ensure optimal genetic testing and care for all EOC patients, the parallel approach of multigene germline testing and somatic BRCA gene testing is increasingly recommended by gynecologic oncology societies [8].
Although parallel germline and tumor‐testing confers advantages, the current model in Ontario duplicates healthcare resources by requiring NGS genetic testing of both germline and tumor tissue samples in EOC. At the same time, evidence from our center showed that a tumor‐first approach has a high sensitivity to detect both somatic and germline variants in BRCA1/2 [15]. The objective of this study was to expand on our BRCA1/2 evidence to a multigene panel and prospectively explore the feasibility of multigene tumor‐testing in EOC by comparing tumor tissue test results with results from germline testing of peripheral blood. We hypothesized that NGS multigene panel tumor‐testing can accurately identify germline variants, and a multigene panel tumor‐first triage model for EOC can be considered.
Methods
2
A single‐center prospective single‐arm cohort study was conducted between October 2021 and October 2023 at the Princess Margaret Cancer Center/University Health Network (UHN) in Toronto, Ontario, Canada. This study conformed to the standards of the Declaration of Helsinki. UHN Research Ethics Board approval was obtained (#20‐5852).
Participants
2.1
Patients with suspected advanced epithelial ovarian cancer (EOC) were approached to participate at their initial gynecologic oncology visit prior to initial surgery or chemotherapy treatment, and consent was obtained from all eligible patients by a research team member. The study inclusion criterion was histology‐confirmed EOC, incorporating serous, clear cell, endometrioid, mucinous, and mixed adenocarcinoma histology. Exclusion criteria were lack of informed consent, age under 18, lack of EOC or cancer confirmation, low‐grade serous histology, and patients receiving treatment at a different institution. Patients were also excluded if the tissue or DNA sample was insufficient or unavailable to perform testing. Patient demographics and clinical data (including age, tumor marker value, initial treatment, family history, pathological stage, and histological subtype), as well as testing results, were collected using the REDCap platform. All participants provided written informed consent prior to inclusion in the study.
Samples and DNA extraction
2.2
For tumor‐testing, a formalin‐fixed paraffin‐embedded (FFPE) sample was reviewed by a pathologist with expertise in gynecologic oncology at the time of initial surgery or biopsy to confirm an EOC diagnosis and ensure sufficient tumor cellularity for NGS (> 20%). Tumor enrichment prior to DNA extraction was performed by sampling 2 × 1 mm cores in a tumor‐rich region, or by microdissection of sections (8 slides at 7‐um thickness). FFPE samples were digested overnight in Proteinase K (20 mg·mL^−1^) and DNA extracted using a magnetic bead purification method (Maxwell FFPE Plus DNA Purification Kit; Promega, Madison, WI, USA) on an automatic extractor (Maxwell 16; Promega). As per institutional policy, if initial testing failed due to insufficient tumor cellularity or insufficient extracted DNA, a second attempt was undertaken on a surgical specimen or repeat biopsy.
For germline tissue, genomic DNA was extracted from peripheral blood samples using QIAsymphony DNA Midi kit (Qiagen, Germantown, MD, USA). DNA concentration for both tumor and germline DNA was evaluated using fluorometry (Qubit dsDNA Assay Kit on the Qubit 2.0 Fluorometer; Thermo Fisher Scientific, Waltham, MA, USA).
NGS testing
2.3
NGS testing was performed at our institutional clinical molecular pathology laboratory (UHN Genome Diagnostics) with experience in NGS multigene testing including BRCA1/2 and other EOC genes. DNA from tumor and germline tissues was analyzed on a custom NGS panel including 18 EOC genes (BRCA1, BRCA2, MLH1, MSH2, MSH6, PMS2, EPCAM, RAD51C, RAD51D, BRIP1, ATM, BARD1, CDH1, CHEK2, PALB2, PTEN, STK11, and TP53). NGS panel testing was clinically validated on DNA extracted from peripheral blood leukocytes (germline) and from tumor tissue (both FFPE and cytology specimens) [15]. Note that genes tested on tumor excluded the HOXB13 gene given the typical association of HOXB13 with prostate and lack of association with ovarian cancer [14, 15]. Testing was performed as previously described [15]. Briefly, hybridization capture libraries (SureSelect XT, Agilent Technologies, Santa Clara, CA, USA) were sequenced on the Illumina platform (NextSeq 500; Illumina, San Diego, CA, USA). To ensure appropriate variant detection, all samples had a minimum read depth of 100× (tumor) and 25× (germline) on target regions. Data analysis used custom bioinformatic analysis with Burrows‐Wheeler Aligner [16] and Genome Analysis Toolkit (GATK) tools. Variant calling used Varscan [17], and copy number variants (CNV) were assessed by CNVkit [18] and DECoN [19]. For any CNVs identified by NGS testing as a possible deletion (CNVkit log_2_ ratio less than −0.8, DECoN reads ratio less than 0.8) or duplication (CNVkit log_2_ ratio greater than 0.8, DECoN reads ratio greater than 1.2), verification was performed using the multiple ligation probe amplification (MLPA) kits P002, P087, and P090 (MRC‐Holland, Amsterdam, The Netherlands). The assay was previously demonstrated to detect single exon level deletions or duplications in BRCA1 and BRCA2 [15].
Variant classifications
2.4
Identified variants were filtered to remove technical artifacts, and benign or likely benign variants (Alissa Clinical Informatic Platform, Agilent). Tumor variants were classified using the Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists [20] and assigned to one of the following classifications: Tier I (variants with strong clinical significance), Tier II (variants with potential clinical significance), or Tier III (variants with unknown clinical significance). Tier IV benign or likely benign variants were removed by filtering as described.
Germline variants were classified using the 2015 guidelines from the American College of Medical Genetics and Genomics and the Association for Molecular Pathology [21]. Variants classified as pathogenic (P), likely pathogenic (LP), or of uncertain significance (VUS) were reported. Benign or likely benign variants were not reported.
Homologous recombination
2.5
Homologous recombination deficiency (HRD) analysis was performed on BRCA‐negative tumor tissue at the Myriad Genetic Laboratories using the Myriad myChoice HRD Plus assay [22] and standard protocol to obtain a genomic instability score (GIS). A GIS threshold of greater than or equal to 42 was used to define a positive HRD status [2].
Sample handling
2.6
A research coordinator ensured compliance with the screening pathway and dual somatic and germline testing being performed. Fig. S1 provides an overview of the patient care trajectory from study enrolment to follow‐up post treatment, and Table S1 provides an overview description of the testing strategies.
Statistical analysis
2.7
Descriptive statistics were used to summarize participant characteristics. Categorical variables were summarized using counts and percentages, whereas continuous variables were summarized using medians and ranges.
Results
3
A total of 129 patients with presumed advanced ovarian cancer were consented for the study, and 23 were excluded (Fig. 1), leaving 106 patients with EOC that completed paired tumor and germline 18‐gene NGS testing and were included in the final analysis. Their demographic characteristics are reported in Table 1. Among the 106 tumors tested, six (5.7%) had no variants identified. In the remaining 100 tumors (94.3%), there were a total of 185 variants identified: 100 TP53 variants (not classified), 27 Tier I/II variants, and 58 Tier III variants. Twenty‐two large deletions or duplications were identified on tumor, ranging in size from a single exon to whole gene; six of them were identified in BRCA1/2.
Enrollment and outcome diagram. LGSC, low‐grade serous carcinoma; LP, likely pathogenic variant; n, number; PV, pathogenic variant; VUS, variant of unknown significance. This Figure excluded TP53 tumor variants. Variants were classified according to scheme of Richards et al. 2015 [21].
For the 27 Tier I/II tumor variants, germline DNA testing confirmed 16/27 (59.3%) to be of germline origin (P or LP variants), while the remaining 11/27 (40.7%) were somatic variants. For the 58 Tier III tumor variants, germline DNA testing confirmed 35/58 (60.3%) to be of germline origin (all VUS), whereas the remaining 23/58 (39.7%) were somatic variants. Among the 106 total patients, 51/106 (48.1%) had no variant identified on tumor‐testing other than TP53, and 50/51 (98.0%) of these had confirmatory negative results on paired germline testing. One patient with TP53 as the sole somatic variant was found to have an exon 12 BRCA1 pathogenic deletion on subsequent germline testing. This patient's family history was significant for three second‐degree relatives diagnosed with cancer (liver, skin, and prostate). Fig. 1 illustrates the outcome and correlation for tumor‐testing followed by germline testing for all patients, highlighting the presence of BRCA 1/2 variants (n = 106). Tumor‐first testing correctly detected variant‐positive and variant‐negative germline cases in 105/106 (99.1%).
A total of 28 clinically significant variants were identified using germline and tumor‐testing: BRCA1 (17), BRCA2 (6), RAD51C (2), ATM (1), PALB2 (1), and PTEN (1). Fig. 2 illustrates the proportion of P/LP germline variants compared to Tier I/II somatic variants. Most patients were found to have one or two tumor variants after excluding TP53 (Fig. 3). P/LP (germline, n = 17) or Tier I/II (tumor, n = 27) variants were most frequently observed in BRCA1, with an incidence of 53% and 59%, respectively (Fig. 4A,B). Other common P/LP germline variants include BRCA2 (29%), RAD51C (12%), and ATM (6%). Other common Tier I/II somatic variants include BRCA2 (22%) and RAD51C (7%). For somatic Tier III variants, BRCA2 alterations were the most common (19%), followed by MSH6 (17%), and then STK11 (12%) (Fig. S2A). In the germline, VUS (n = 35) were most identified in BRCA2 and MSH6 (23% each), followed by PMS2, PALB2, and ATM (all 9%) (Fig. S2B).
Variants identified on paired tumor‐germline testing (excluding TP53 variants) (n = 106). n, number. This Figure included likely pathogenic and pathogenic germline variants, as well as Tiers I and II somatic variants.
Tumor variant burden (excluding TP53 variants) (n = 106). n, number. This Figure excluded TP53 tumor variants.
Variant description (A) Somatic Tiers I and II variants (n = 27). (B) Germline likely pathogenic and pathogenic (LP/P) variants (n = 17). LP, likely pathogenic variant; n, number; PV, pathogenic variant. This Figure included likely pathogenic and pathogenic germline variants, as well as Tiers I and II somatic variants. Variants were classified according to scheme of Richards et al. 2015 [21].
HRD testing was performed among 50 of 83 BRCA‐negative patients (60.2%). Reasons for not undergoing HRD testing are reported in Table S2. There were 14/50 (28%) patients with positive HRD testing (GIS ≥ 42), 30/50 (60%) with negative results, and 6/50 (12%) with inconclusive results. Among the 14 patients with positive HRD scores (Table 2), two (14.3%) had pathogenic variants: one with a RAD51C germline PV identified as a Tier II tumor variant, and one with a PALB2 Tier II somatic variant. Among the 30 patients with negative HRD scores (Table 3), one (3.3%) had a RAD51C LP variant identified as a Tier II tumor variant; this patient had a GIS of 40.
Discussion
4
The current prospective study performed paired germline‐tumor 18‐gene panel NGS testing for 106 patients with EOC. The results showed that tumor panel testing is both feasible and reliable in detecting germline variants, as tumor‐testing correctly identified variant‐positive and variant‐negative germline cases in 99.1% of cases. In terms of BRCA1/2 variants, the current study supports our previously reported retrospective data of matched tumor and germline samples from 200 EOC patients, where we demonstrated a 100% concordance rate between tumor and germline BRCA1/2 NGS testing [15]. For other EOC‐risk genes, specifically RAD51, ATM, PTEN, and PALB2, tumor‐testing correctly identified all germline variants in the current study. This prospective data support our previous retrospective study, which also identified 10 additional variants (BRIP1, MSH2, RAD51C, and RAD51D) in the tumor samples with subsequent germline confirmation [15]. Several studies in the literature looked at tumor and germline paired testing using a panel extending to other genes associated with EOC and showed promising results about the feasibility of multigene tumor‐testing in EOC [23, 24, 25, 26, 27, 28]. In other words, the current study provides important prospective ground for reinforcing evidence about the reliability of integrated tumor‐germline testing in EOC. A multigene tumor‐testing triage is important to consider, as it is recognized that a tumor‐first approach can help minimize patients lost to follow‐up for germline‐only testing [10].
The current study provides evidence that a tumor‐first approach for genetic panel testing in EOC can reduce duplicate testing. Broad gene panel tumor‐testing identified that 48.1% of patients had no variants (excluding TP53), and concurrent germline testing confirmed that no additional germline variants were present. This suggests that patients with tumor TP53 variants in isolation may not require genetic counseling and follow‐up germline testing, as the probability of identifying a relevant germline variant in any gene included on the tumor‐testing panel is low. The exception to this is the presence of a family history of ovarian cancer or Li‐Fraumeni syndrome, or patients younger than 30 years [29]. If a relevant tumor variant is identified, subsequent germline testing would be performed on this subgroup to provide information about variant origin (germline versus tumor) and need for genetic testing for at‐risk relatives in the event of germline confirmation. If no variant is identified, then this subgroup (i.e., approximately half of the EOC patients) would not require follow‐up germline analysis, substantially reducing duplicate testing. This model is expected to decrease workloads for both molecular genetics laboratories and hereditary cancer clinics. This is important given that wait times for genetics assessment are a recognized barrier to accessing genetic testing in Canada and across North America [30, 31]. Reflex tumor‐testing for BRCA1/2 in the ovarian cancer population has already been shown to increase access to genetic testing and decrease wait times [32]. Expanding a tumor‐testing program to include all potentially relevant hereditary genes would be expected to demonstrate a similar effect. In addition, expanded tumor‐testing could address raised concerns about high healthcare and societal costs associated with high‐volume duplicate genetic testing in EOC [33, 34, 35].
The current study had a < 1% false‐negative rate in terms of tumor panel ability to correctly categorize germline variant status. The one false negative involved a germline pathogenic single exon 12 deletion in BRCA1 that was not reported in testing of DNA from the FFPE‐matched tumor sample. Of note, this is a small deletion involving a single exon, which is recognized to be particularly challenging to detect using NGS performed on FFPE samples. The potential for false‐negative results in either tumor or germline testing is an important consideration. This has been of particular concern with respect to single exon copy number variation in tumor‐testing [36]. The results of this and our previous study [15] demonstrate that tumor NGS testing that is optimized for FFPE analysis has the capability to detect most germline variants including single and multi‐exon CNVs. In considering a tumor‐testing program, there may be additional strategies to further increase the detection of these challenging CNVs, for example ensuring optimal DNA quality from FFPE extraction used in NGS testing, performing a review of CNV data close to thresholds to detect potential CNVs, or using multiple CNV callers on NGS data. Concurrent tumor and germline testing for all patients is currently employed by many to maximize detection with the intent to ensure no clinically relevant variants remain undetected. However, there is increasing evidence that appropriately validated tumor‐testing performed in an experienced laboratory is highly sensitive for detecting germline variants [15, 37]. When considering future testing program development, the resources required to complete duplicate testing for every patient need to be carefully weighed against the low probability of false‐negative results.
PARPi treatment is key for improving survival outcomes in EOC [9, 38]. For patients with no detected BRCA germline or somatic variant, HRD testing is an important predictor of the PARPi treatment effect [38]. In this study, 50 BRCA‐negative patients were tested by HRD analysis (Myriad myChoice CDx HRD), and 14/50 (28%) patients were found to have a positive genomic instability score (GIS). Two of 14 patients were found to have pathogenic variants with our regional approved NGS EOC panel (1 germline PV in RAD51C; 1 somatic Tier II variant in PALB2), indicating that HRD analysis can possibly identify more patients suitable for PARPi than NGS gene‐level panels alone. However, the identification of one patient with a germline PV in RAD51C and a negative GIS (GIS = 40) indicates that multiple strategies remain important to maximize the benefit for patients. According to the PRIMA trial, patients with negative GISs derive less benefit from PARPi maintenance [38]. However, there is emerging evidence regarding the role of other genes involved in the homologous recombinant pathway, for instance ATM and RAD51 status in predicting PARPi efficacy and chemotherapy response [39, 40, 41]. In other words, a broader genetic panel for tumor‐testing can provide useful first‐step information for assessing hereditary risk; however, the immediate utility of identifying non‐BRCA tumor PVs is less clear.
The current study has several advantages. First, it describes evidence for paired comparisons between tumor and germline NGS panel genetic testing in EOC using a prospective approach, this allowing for real‐time comparisons and eliminating recall or selection bias. In addition, it provides a technical platform for tumor multigene NGS testing in EOC using standard methodology based on recommendations from the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists for the tumor variants, and the American College of Medical Genetics and Genomics and the Association for Molecular Pathology for the germline variant classification [20, 21].
The study does have several limitations. For instance, the sample size limits conclusions about rare histology EOC subtypes or non‐BRCA variants associated with EOC, which are less frequent. This could limit understanding and conclusions about rare pathogenic variants or low‐frequency genes. Similarly, further research focused on specific histological subtypes could further explore the understanding of paired tumor‐germline testing in these rarer subtypes. As well, HRD testing is performed on a subgroup of the sample, and BRCA somatic Tiers I and II did not undergo HRD testing. This limits the ability to generate hypotheses correlating HRD testing results and non‐BRCA tumor variants. Also, the study focused on the genes part of the Ontario current panel testing; no conclusions can be made regarding emerging or moderate‐penetrance genes not included. Finally, this study was not powered to assess the influence of PV on treatment strategy and survival. A recent study by Kim et al. showed that patients with stage III/IV BRCA mutated high‐grade serous ovarian cancers had improved survival with primary cytoreductive surgery compared with neoadjuvant chemotherapy, which would support the necessity of early genetic screening to streamline the primary management of advanced ovarian cancer [42].
Conclusion
5
In conclusion, the results of the current study provide further evidence for consideration of a tumor‐first approach in EOC as the sensitivity of molecular tumor test methods continues to improve. Tumor multigene NGS testing is a reliable method in EOC, as it is feasible, efficient in detecting BRCA and non‐BRCA variants, can be performed reflexively on biopsy or surgical specimens, and can decrease duplication of genetic testing. Our study illustrates that near half of the patients could potentially avoid germline testing and genetic counseling following negative tumor results, while also carefully considering other guidelines for testing, such as clinical indications (family history) or limitations of tumor‐testing (allele dropout, CNVs, tumor heterogeneity). For those with positive tumor results, subsequent germline testing is important to identify familial mutations and associated implications: secondary malignancy prevention strategies for EOC patients, identification of other affected family members, and implementation of risk‐reduction strategies for affected family members. In this current cohort, this approach identified germline variants with a < 1% false‐negative rate, which flags a need for vigilance in minimizing false‐negative results, for instance by initiating a “gray zone” analysis particularly designed to flag small CNVs and to ensure gray zone cases undergo germline testing for CNV confirmation. Further investigations are required to best optimize and refine the tumor‐first genetic testing approach.
Conflict of interest
Jeanna McCuaig is an employee of AstraZeneca since September 2023. She was not employed by them at any time during the development, initiation, or conduct of this study.
Author contributions
ES: study planning, data collection, data interpretation, manuscript draft, and review. CM: data collection, data interpretation, manuscript draft and review. MC: data collection, data interpretation, manuscript draft and review. TS: study planning, data interpretation, manuscript draft and review. RK: study planning, data interpretation, manuscript review. JM: study planning, manuscript review. BC: study planning, manuscript review. LR: data collection, manuscript review. CS: data collection, manuscript review. SF: study planning, data interpretation, manuscript review. LH: data interpretation, manuscript review. TM: data interpretation, manuscript review. MB: study planning, supervision, data interpretation, manuscript review.
Supporting information
Data S1. Overview of the Genetic Testing Performed.
Fig. S1. Overview of patient care trajectory from study enrolment to follow‐up period.
Fig. S2. Variant description (A) Somatic Tier III variants (n = 58) (B) Germline variants of uncertain significance (VUS) (n = 35).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torre LA , Trabert B , De Santis CE , Miller KD , Samimi G , Runowicz CD , et al. Ovarian cancer statistics, 2018. CA Cancer J Clin. 2018;68(4):284–296. 10.3322/caac.21456 29809280 PMC 6621554 · doi ↗ · pubmed ↗
- 2Liu J , Berchuck A , Backes FJ , Cohen J , Grisham R , Leath CA , et al. NCCN guidelines(R) insights: ovarian cancer/fallopian tube cancer/primary peritoneal cancer, version 3.2024. J Natl Compr Cancer Netw. 2024;22(8):512–519. 10.6004/jnccn.2024.0052 · doi ↗
- 3Zhang S , Royer R , Li S , Mc Laughlin JR , Rosen B , Risch HA , et al. Frequencies of BRCA 1 and BRCA 2 mutations among 1342 unselected patients with invasive ovarian cancer. Gynecol Oncol. 2011;121(2):353–357. 10.1016/j.ygyno.2011.01.020 21324516 · doi ↗ · pubmed ↗
- 4Norquist BM , Harrell MI , Brady MF , Walsh T , Lee MK , Gulsuner S , et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482–490.26720728 10.1001/jamaoncol.2015.5495 PMC 4845939 · doi ↗ · pubmed ↗
- 5Tung N , Domchek SM , Stadler Z , Nathanson KL , Couch F , Garber JE , et al. Counseling framework for moderate‐penetrance cancer‐susceptibility mutations. Nat Rev Clin Oncol. 2016;13:581–588.27296296 10.1038/nrclinonc.2016.90PMC 5513673 · doi ↗ · pubmed ↗
- 6Walsh T , Casadei S , Lee MK , Pennil CC , Nord AS , Thornton AM , et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc Natl Acad Sci USA. 2011;108:18032–18037.22006311 10.1073/pnas.1115052108 PMC 3207658 · doi ↗ · pubmed ↗
- 7Konstantinopoulos BNPA , Lacchetti C , Armstrong D , Grisham RN , Goodfellow PJ , Kohn EC , et al. Germline and somatic tumor testing in epithelial ovarian cancer: ASCO guideline. J Clin Oncol. 2020;38(11):1222–1245. 10.1200/JCO.19.02960 31986064 PMC 8842911 · doi ↗ · pubmed ↗
- 8Gressel GM , Frey MK , Norquist B , Senter L , Blank SV , Urban RR . Germline and somatic testing for ovarian cancer: an SGO clinical practice statement. Gynecol Oncol. 2024;181:170–178. 10.1016/j.ygyno.2023.12.010 38215513 · doi ↗ · pubmed ↗