Visual DAT‐SPECT Outperforms Semiquantitative Analysis in a “Pseudo‐SWEDD” Case of Benign Tremulous Parkinsonism
Daniele Birreci, Luca Angelini, Martina De Riggi, Simone Aloisio, Adriana Martini, Sofia A. Grandolfo, Luca Marsili, Roberto Cilia, Alberto J. Espay, Matteo Bologna

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
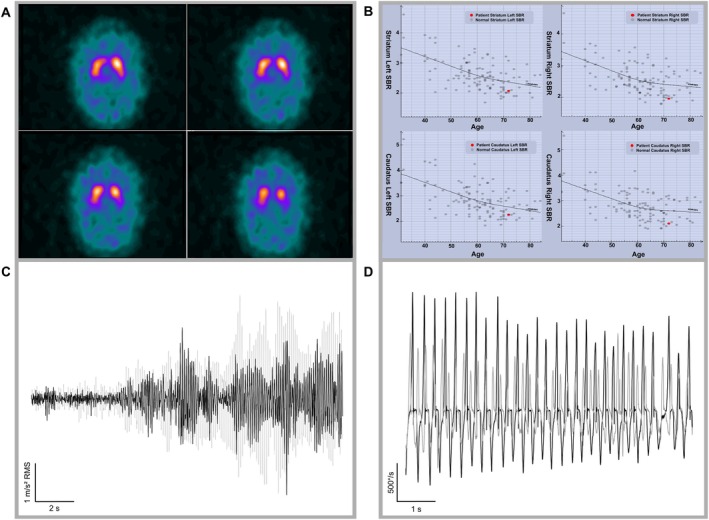 Figure 1
Figure 1- —Ministero della Salute10.13039/501100003196
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Parkinson's Disease Mechanisms and Treatments · Genetic Neurodegenerative Diseases
A subset of patients with a long‐standing history of hand tremor may eventually develop features of Parkinson's disease (PD). This monosymptomatic presentation, termed “benign tremulous parkinsonism” (BTP), may exhibit postural tremor reminiscent of essential tremor (ET) with a resting component.1 In such cases, dopamine transporter single‐photon emission computed tomography (DAT‐SPECT) may help distinguish ET from PD. We report a case in which clinical and neurophysiological findings supported PD, whereas quantitative DAT‐SPECT analysis did not.
A 73‐year‐old man, referred to the outpatient clinic at Sapienza University of Rome, had a 10‐year history of a slowly progressing right‐predominant bilateral action and rest hand tremor (Appendix S1). On examination, he showed a re‐emergent component of the hand tremor, head and voice tremor, hypomimia, subtle bradykinesia with rigidity on the right side associated with a sequence effect and slowed speed on the right‐arm finger‐to‐nose task (Video 1).
Despite a clinical impression of parkinsonism, the semiquantitative imaging assessment using DaTQUANT (Appendix S2) showed tracer uptake within the lower end of the normal range2 (Fig. 1), justifying a normal DAT‐SPECT report. Visual inspection, however, detected modest DAT signal reduction in the left posterior putamen, contralateral to the tremor side. At the time of assessment, the patient was taking levodopa (l‐dopa)/benserazide (100/25 mg), 1 tablet thrice daily. Although he reported no benefits, we conducted a clinical and kinematic evaluation before and after treatment discontinuation. The comparison between the on and off states is shown in Video 1, even if no significant differences in clinical scores were documented, likely due to a subtherapeutic dose (Appendix S1). Nevertheless, kinematic analysis3 showed a subclinical l‐dopa effect, with reduced re‐emergent tremor amplitude and improved movement velocity and sequence effect (Fig. 1; Table S1).
To the best of our knowledge, this is the first case where the clinical examination suggested PD, a kinematic analysis suggested a subclinical l‐dopa effect, a visual DAT‐SPECT interpretation supported such conclusion, but a quantitative analysis did not—in the end justifying the incorrect conclusion of a scan without evidence of dopaminergic denervation (SWEDD). This “pseudo‐SWEDD” case highlights the dissociation between qualitative and semiquantitative DAT‐SPECT appraisal and challenges the presumed superiority of the latter.
Collectively, the data point to a BTP presentation of PD. Prior studies have reported subtle bilateral DAT reduction in tremor‐dominant PD4 and relatively preserved caudate binding versus non‐tremor PD,5 suggesting milder dopaminergic deficits in such phenotypes, possibly shared by BTP. Common misdiagnoses include ET, dystonic tremor, or “SWEDD.”
Particularly, the kinematic analysis demonstrated a subclinical improvement in motor function with subtherapeutic doses of l‐dopa (a “sub‐on” state), whereas its discontinuation worsened the re‐emergent tremor and slowed movement execution without the patient's awareness, supporting the diagnosis of PD.
In conclusion, this case illustrates how integrated clinical and kinematic assessments, along with qualitative DAT‐SPECT inspection, can support the diagnosis of PD despite normal quantitative imaging reports.
Author Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical analysis: A. Design, B. Execution, C. Review and critique; (3) Manuscript: A. Writing of the first draft, B. Review and critique.
D.B.: 1A, 1B, 1C, 3A
L.A.: 1A, 3B
M.D.R.: 3B
S.A.: 3B
A.M.: 1C, 3B
S.A.G.: 3B
L.M.: 1A, 3B
R.C.: 1A, 3B
A.J.E.: 1A, 3A, 3B
M.B.: 1A, 1B, 3A, 3B
Disclosures
Ethical Compliance Statement: The authors confirm that approval of an institutional review board or ethics committee was not required for this case report. All procedures performed were in accordance with the ethical standards of our institution and with the Helsinki Declaration. Written informed consent was obtained from the patient for the publication of his data and the online distribution of the related video material. We confirm that we have read the journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflicts of Interest: This work was supported by the Italian Ministry of Health (Current Research 2025). The authors declare that there are no conflicts of interest relevant to this work.
Financial Disclosures for the Previous 12 Months: L.M. has received honoraria from the International Association of Parkinsonism and Related Disorders (IAPRD) Society for social media and web support. L.M.has received a grant (collaborative research agreement) from the International Parkinson and Movement Disorders Society for the MDS‐UTRS Validation Program (role: principal investigator), Non‐Profit. A.E.J. has received grant support from the NIH and the Michael J. Fox Foundation; personal compensation as a consultant/scientific advisory board member for Mitsubishi Tanabe Pharma America (formerly Neuroderm), Amneal, Acorda, AbbVie, Bial, Kyowa Kirin, Supernus (formerly USWorldMeds), NeuroDiagnostics, Inc. (SYNAPS Dx), Intrance Medical Systems, Inc., Merz, Praxis Precision Medicines, Citrus Health, and Herantis Pharma; Data Safety Monitoring Board (chair) of AskBio; and publishing royalties from Lippincott Williams & Wilkins, Cambridge University Press, and Springer. He is coinventor of the patent “Compositions and methods for treatment and/or prophylaxis of proteinopathies.” He cofounded REGAIN Therapeutics to fund preclinical studies but relinquished the right to any personal income from future treatments. The other authors declare that there are no additional disclosures to report.
Supporting information
Table S1. Kinematic measures during levodopa therapy (on state) and after treatment discontinuation (off state), including tremor amplitude and frequency, and finger‐tapping parameters, with reference values from healthy controls. Appendix S1. Additional clinical details, including past medical history and results of clinical assessments during levodopa therapy (on state) and after treatment discontinuation (off state), with clinical scores. Appendix S2. Description of the dopamine transporter single‐photon emission computed tomography (DAT‐SPECT) semiquantitative analysis using DaTQUANT, including software specifications, image processing methods, regions of interest analyzed, reference region used for normalization, and the normative database applied for z‐score calculation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deeb W , Hu W , Almeida L , Patterson A , Martinez‐Ramirez D , Wagle Shukla A . Benign tremulous parkinsonism: a unique entity or another facet of Parkinson's disease? Transl Neurodegener 2016;5:10. 10.1186/s 40035-016-0057-1.27213042 PMC 4874026 · doi ↗ · pubmed ↗
- 2Lanfranchi F , Arnaldi D , Miceli A , et al. Different z‐score cut‐offs for striatal binding ratio (SBR) of Da T SPECT are needed to support the diagnosis of Parkinson's disease (PD) and dementia with Lewy bodies (DLB). Eur J Nucl Med Mol Imaging 2023;50(4):1090–1102. 10.1007/s 00259-022-06069-0.36471041 · doi ↗ · pubmed ↗
- 3Angelini L , Paparella G , Cannavacciuolo A , et al. Clinical and kinematic characterization of parkinsonian soft signs in essential tremor. J Neural Transm (Vienna) 2024;131(8):941–952. 10.1007/s 00702-024-02784-0.38744708 PMC 11343963 · doi ↗ · pubmed ↗
- 4Clarimón J , Pagonabarraga J , Paisán‐Ruíz C , et al. Tremor dominant parkinsonism: clinical description and LRRK 2 mutation screening. Mov Disord 2008;23(4):518–523. 10.1002/mds.21771.18098275 · doi ↗ · pubmed ↗
- 5Kaasinen V , Kinos M , Joutsa J , Seppänen M , Noponen T . Differences in striatal dopamine transporter density between tremor dominant and non‐tremor Parkinson's disease. Eur J Nucl Med Mol Imaging 2014;41(10):1931–1937. 10.1007/s 00259-014-2796-5.24867256 · doi ↗ · pubmed ↗