Septic coronary embolism presenting as anterior STEMI: a stentless PCI strategy guided by clinical inconsistency and pathological confirmation—case report
Noriaki Iwahashi, Reiko Tanaka, Satoshi Fujii, Keiji Uchida, Kiyoshi Hibi

TL;DR
A man with a heart attack caused by a septic embolism was treated without a stent after tests confirmed bacterial infection.
Contribution
The paper presents a novel stentless PCI strategy based on clinical and pathological evidence of septic embolism.
Findings
Septic coronary embolism mimicked STEMI but was confirmed via thrombus analysis.
Stent implantation was avoided due to bacteremic risk, preventing potential complications.
Infective endocarditis led to aortic regurgitation requiring urgent valve replacement.
Abstract
Septic coronary embolism is an uncommon cause of acute myocardial infarction and may mimic atherosclerotic occlusion. Early distinction between these mechanisms is essential because routine stent implantation may be hazardous in bacteremic conditions. A 48-year-old man presented with an anterior ST-segment elevation myocardial infarction with high fever. Coronary angiography revealed abrupt mid–left anterior descending artery occlusion with a smooth vessel contour (Figure 1). Intravascular ultrasound showed a large intraluminal thrombus without underlying plaque (Figure 2). Because these findings were inconsistent with plaque rupture, stent implantation was intentionally avoided. Pathological analysis of the aspirated thrombus demonstrated bacterial colonies (Figure 3), confirming septic coronary embolism due to methicillin-sensitive Staphylococcus aureus infective endocarditis. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
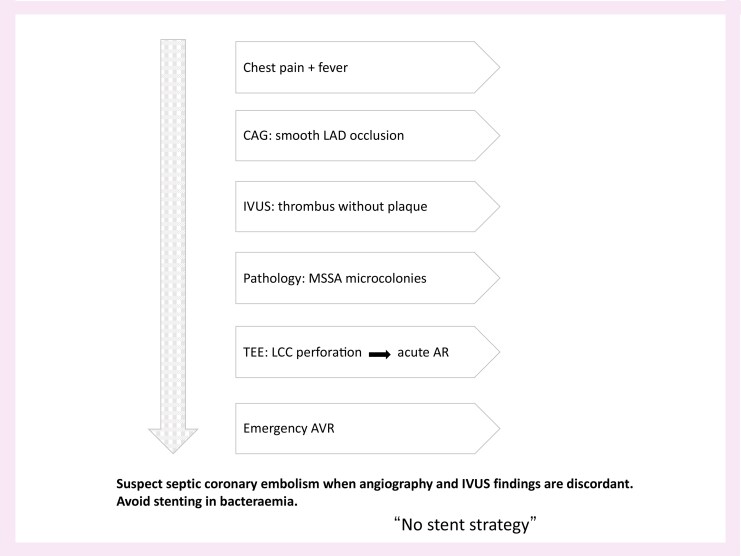 Figure 1
Figure 1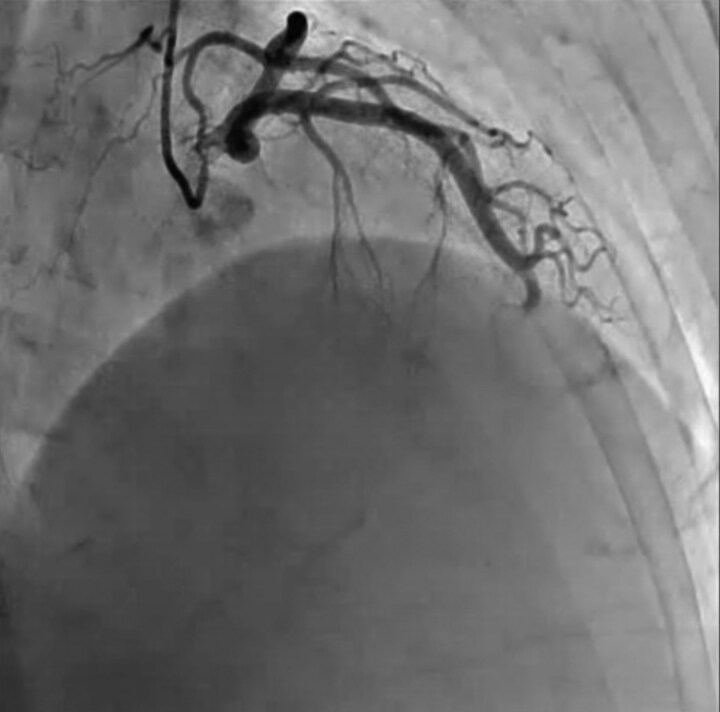 Figure 1
Figure 1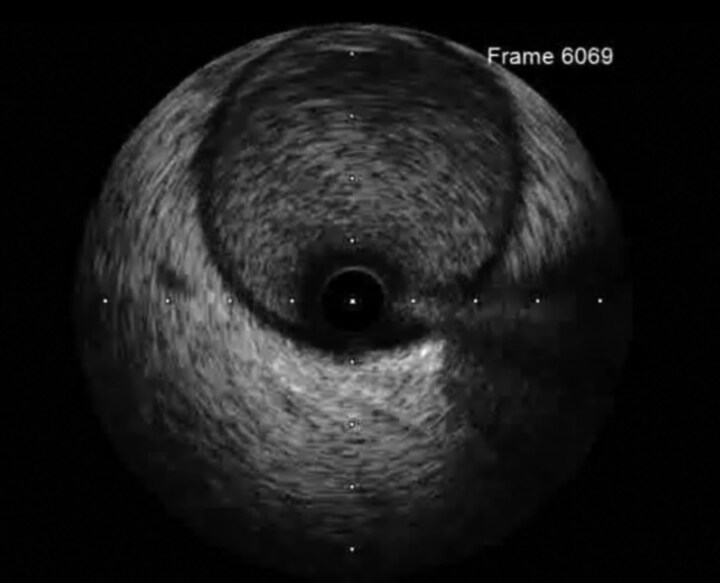 Figure 2
Figure 2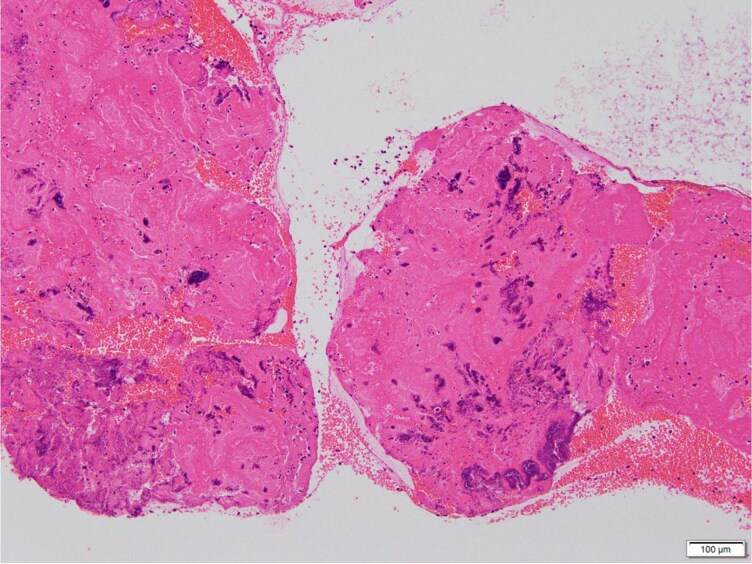 Figure 3
Figure 3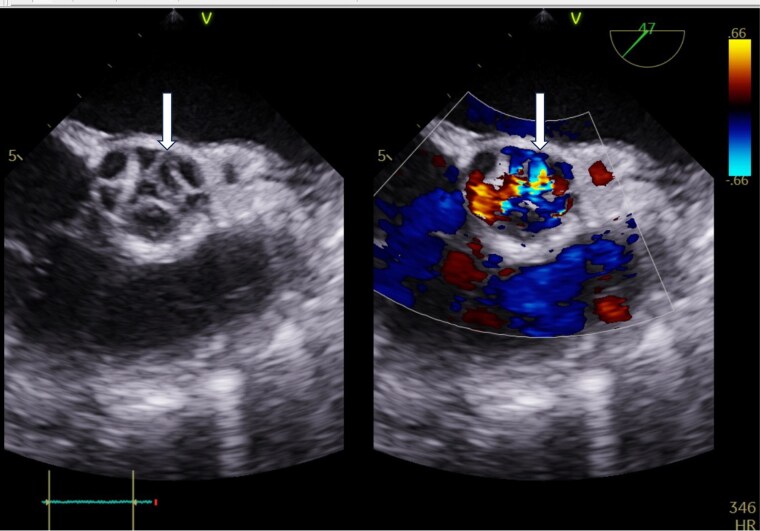 Figure 4
Figure 4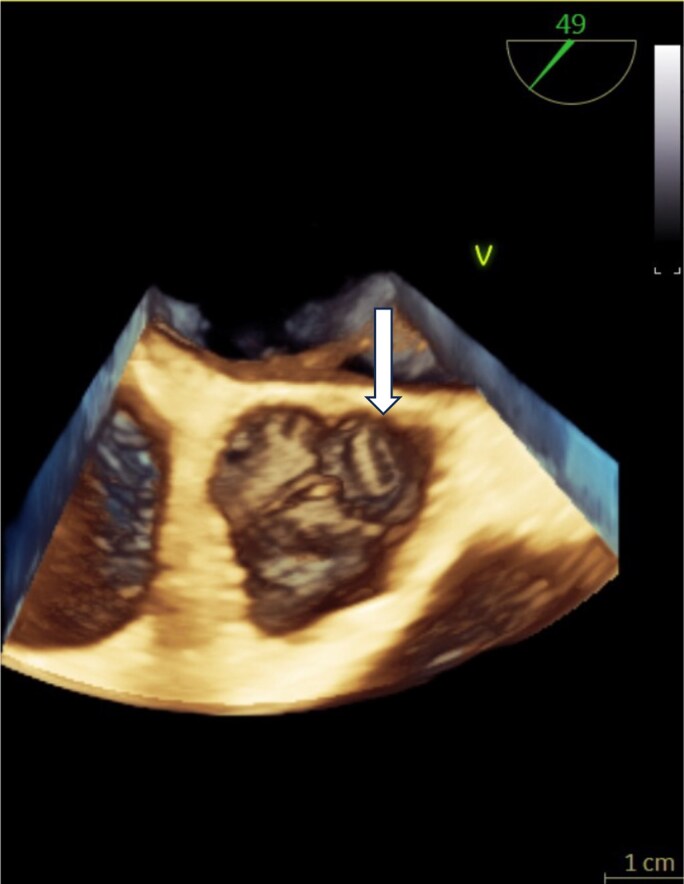 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Aortic Thrombus and Embolism · Cardiac Valve Diseases and Treatments
Introduction
Septic coronary embolism is a rare cause of acute myocardial infarction and may closely mimic atherosclerotic occlusion on angiography. Distinguishing these mechanisms during primary percutaneous coronary intervention is challenging but essential, as stent implantation in the setting of bacteremia carries substantial risks, including device infection or mycotic complications. We report a case of septic coronary embolism initially presenting as an anterior ST-segment elevation myocardial infarction, in which intravascular imaging and thrombus pathology were instrumental in reaching the correct diagnosis and guiding appropriate management. Septic coronary embolism has been reported as a rare but important cause of acute myocardial infarction.^1–3^
Summary figure
**
Case presentation
A 48-year-old previously healthy man presented with sudden-onset chest pain and persistent fever. Electrocardiography showed anterior ST-segment elevation, prompting emergent coronary angiography. Imaging demonstrated abrupt occlusion of the mid–left anterior descending artery with a smooth, tapering contour and no angiographic signs of plaque rupture (Figure 1).
Coronary angiography. Abrupt occlusion of the mid–left anterior descending artery with a smooth, tapering contour and no angiographic evidence of underlying atherosclerotic plaque, raising suspicion of a non-atherosclerotic mechanism.
Intravascular ultrasound revealed a large, homogeneous thrombus occupying the lumen without evidence of plaque rupture, calcification, or atherosclerotic burden (Figure 2). The discrepancy between the patient’s angiographic morphology and typical features of atherosclerotic occlusion raised suspicion of a non-atherosclerotic mechanism. Consequently, stent implantation was avoided, and thrombus aspiration was performed.
Intravascular ultrasound. A large, homogeneous intraluminal thrombus without calcification or atherosclerotic plaque. The vessel wall appears smooth and intact, inconsistent with plaque rupture or erosion.
Pathological examination of the aspirated thrombus demonstrated basophilic, grape-like microcolonies of bacteria embedded within fibrin (Figure 3), establishing the diagnosis of septic coronary embolism. Methicillin-sensitive Staphylococcus aureus was isolated from all blood culture samples obtained both during and after the catheterisation.
Pathological examination of the aspirated thrombus. Hematoxylin–eosin staining demonstrating basophilic (purple) microcolonies arranged in grape-like clusters within a fibrin-rich thrombus, consistent with Gram-positive cocci such as methicillin-sensitive Staphylococcus aureus.
Transesophageal echocardiography revealed a perforation of the left coronary cusp with a simultaneous eccentric aortic regurgitation jet, confirming acute valve destruction due to infective endocarditis (Figure 4). Three-dimensional transesophageal echocardiography further delineated the perforation from an en face perspective, providing structural confirmation of the anatomical defect (Figure 5).
Two-dimensional transesophageal echocardiography. (A) Mid-oesophagal long-axis view showing perforation of the left coronary cusp without colour Doppler, demonstrating the anatomical defect caused by infective endocarditis. (B) Colour Doppler imaging demonstrates a simultaneous eccentric aortic regurgitation jet originating from the perforation, indicating acute valve failure.
Three-dimensional transesophageal echocardiography. En-face 3D view clearly delineating perforation of the left coronary cusp, providing structural confirmation of the anatomical defect responsible for acute severe aortic regurgitation.
Discussion
Septic coronary embolism is a rare aetiology of acute myocardial infarction, often presenting with angiographic features that overlap with conventional thrombotic occlusion. The smooth tapering morphology of the coronary obstruction (Figure 1) and the absence of an atherosclerotic substrate on intravascular ultrasound (Figure 2) were key clues indicating an embolic mechanism rather than plaque rupture.
Avoiding stent implantation was an important decision in this case. Introducing intravascular prosthetic material during active bacteremia may lead to stent infection, peri-stent abscess, or mycotic aneurysm, all associated with high morbidity and mortality. The patient’s rapid progression to acute severe aortic regurgitation—confirmed by transesophageal echocardiography showing cusp perforation (Figures 4 and 5)—further emphasized the severity of disseminated infection.
Definitive etiologic diagnosis was achieved only through pathological analysis of the aspirated thrombus (Figure 3), which demonstrated bacterial colonies. This is rarely accomplished in clinical practice but provides critical information that guides antimicrobial therapy and the need for surgical intervention.
This case underscores the importance of correlating clinical features and intravascular imaging in atypical acute coronary syndromes. In the presence of fever, systemic inflammation, and imaging inconsistencies, septic coronary embolism should be strongly considered, and a stentless strategy may be preferable. These findings are consistent with previous reports and current guideline-based understanding of infective endocarditis and its complications.^4,5^
Conclusions
Septic coronary embolism must be recognized early when angiographic and intravascular imaging findings are discordant with typical plaque rupture. A stentless strategy supported by thrombus pathology is essential for appropriate antimicrobial and surgical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shibata T, Kawakami S, Noguchi T, Tomotaka T, Asaumi Y, Kanaya T, et al Prevalence, clinical features, and prognosis of acute myocardial infarction attributable to coronary artery embolism. Circulation 2015;132:241–250.26216084 10.1161/CIRCULATIONAHA.114.015134 · doi ↗ · pubmed ↗
- 2Holland TL, Baddour LM, Bayer AS, Hoen B, Miro JM, Fowler VG. Infective endocarditis. Nat Rev Dis Primers 2016;2:16059.27582414 10.1038/nrdp.2016.59PMC 5240923 · doi ↗ · pubmed ↗
- 3Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al 2015 ESC guidelines for the management of infective endocarditis. Eur Heart J 2015;36:3075–3128.26320109 10.1093/eurheartj/ehv 319 · doi ↗ · pubmed ↗
- 4Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, et al 2023 ESC guidelines for the management of endocarditis. Eur Heart J 2023;44:3948–4033.37622656 10.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 5Mazzotta R, Orlandi M, Scheggi V, Marchionni N, Stefàno P. Coronary embolism in left-sided infective endocarditis: a retrospective analysis from a high-volume surgical centre. P Lo S One 2024;19:e 0314718.39630824 10.1371/journal.pone.0314718 PMC 11616836 · doi ↗ · pubmed ↗