Dengue-induced pancarditis manifestation of young female with systemic lupus erythematosus: case report
Mochamad Rizky Hendiperdana, Muhammad Adityansah, Astrid Putri, Nugroho Sigit

TL;DR
A young woman with lupus and dengue developed severe heart inflammation, which improved with immunosuppressive treatment.
Contribution
This case report highlights dengue-induced pancarditis in a systemic lupus erythematosus patient with lupus nephritis and acute heart failure.
Findings
The patient showed valvulitis, myocarditis, and pericarditis confirmed by echocardiography.
Treatment with corticosteroids and cyclosporin led to significant clinical and functional improvement after three months.
Dengue was identified as a potential trigger for lupus flare and cardiac complications in this case.
Abstract
Lupus activity is associated with cardiac manifestation with varied clinical spectrum from asymptomatic disease-to-fulminant heart failure (HF) and cardiogenic shock. Pancardiac inflammation manifestation in systemic lupus erythematosus (SLE) patient with acute HF manifestation is relatively rare condition. Although, the most common cardiac involvement of SLE is pericarditis. However, cardiac involvement of SLE can affect all layers of the heart: endocardium as valvulitis, myocardium, and pericardium. Overt lupus myocarditis was a rare occurrence (5%–10%), but has a fatal outcome, and this was associated with worse prognostic. While, valvulitis manifestation of SLE is also rare compared to pericarditis, it accounts for less than 20% of SLE. A 39-year-old female presented with acute HF symptom with vasculitis sign phenomena and renal insufficiency. Laboratory result showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
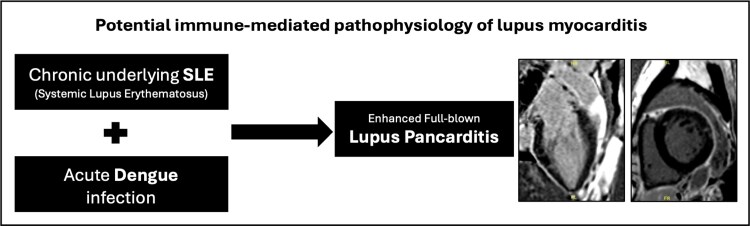 Figure 1
Figure 1 Figure 1
Figure 1 Figure 2
Figure 2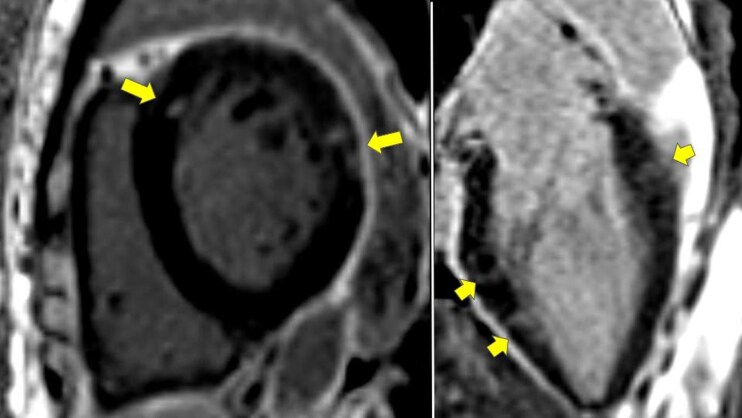 Figure 3
Figure 3| Anti-nuclear antibody profile | Class |
|---|---|
| Anti-RNP/SM | 0 (negative) |
| Anti-Sm | (+) (borderline) |
| Anti-SS-A native (SSA) | +++ (strongly positive) |
| Anti-R0-52 recombinant | +++ (strongly positive) |
| Anti-SS-B (SSB) | +++ (strongly positive) |
| Anti-Scl-70 (Scl) | 0 (negative) |
| Anti-PM Scl-100 (PM) | 0 (negative) |
| Anti-Jo-1 (Jo) | 0 (negative) |
| Anti-centromere B (CB) | 0 (negative) |
| Anti-PCNA | 0 (negative) |
| Anti-dsDNA (DNA) | 0 (negative) |
| Anti-nucleosomes (NUC) | +++ (strongly positive) |
| Anti-histones (HI) | +++ (strongly positive) |
| Anti-ribosomal protein (RIB) | 0 (negative) |
| Anti-AMA-M2 (M2) | + (positive) |
| Anti-DFS70 | 0 (negative) |
| Control (ko) | +++ (strongly positive) |
| 19 May (admission) | 22 May (discharge) | 17 June | 30 June | 24 July | |
|---|---|---|---|---|---|
| Haematology | |||||
| Haemoglobin (g/dL) | 10.8 | 10.5 | 10.4 | 10.4 | 12.1 |
| Leukocyte (cells/µL) | 3260 | 3300 | 2900 | 5570 | 4130 |
| Thrombocyte (cells/µL) | 65 000 | 59 000 | 106 000 | 102 000 | 149 000 |
| Blood chemistry | |||||
| Serum creatinine (mg/dL) | 2.3 | 3.1 | 2.1 | 1.8 | 1.6 |
| Estimated GFR (mL/minute) | 25.09 | 16.70 | 21.54 | 33.29 | 38.14 |
| Blood urea nitrogen (mg/dL) | 84 | 140 | 78 | 66 | 67 |
| SGOT (U/L) | 19 | ||||
| SGPT (U/L) | 5 | ||||
| Urinalysis | |||||
| Urine protein | + 3 | +3 | +3 | ||
| Blood | + 3 | +1 | +1 | ||
| Nitrite urine | Negative | Negative | Negative | ||
| Leukocyte esterases | Negative | Negative | Negative | ||
| Erythrocyte sediment | +2 | +1 | |||
| Epithelial sediment | +1 | +1 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Systemic Lupus Erythematosus Research · Viral Infections and Immunology Research
Introduction
Lupus activity is associated with cardiac manifestation with varied clinical spectrum from asymptomatic disease-to-fulminant heart failure (HF).^1–3^ Pancardiac inflammation manifestation in systemic lupus erythematosus (SLE) patient with acute HF manifestation is relatively rare condition. Although the most common cardiac involvement of SLE is pericarditis, cardiac involvement of SLE can affect all layers of heart: endocardium as valvulitis, myocardium, and pericardium.^4^ Overt lupus myocarditis (LM) was a rare occurrence (5%–10%), but has a fatal outcome, and this was associated with worse prognostic. While valvulitis manifestation of SLE is also rare compared to pericarditis, it accounts for less than 20% of SLE.^1–6^
Summary figure
Visual summary of pathophysiological process.
**
Case summary
A 39-year-old female presented to emergency ward with progressive shortness of breath that worsened 3 days prior to present admission. The patient complained peripheral leg oedema, abdominal pain that accompanied by constitutional symptom of febrile, joint pain, hair loss, progressive weight loss of 7 kg in a year, amenorrhoea for a year, and scattered painless redness on palmar and plantar fingers several weeks prior to recent admission. The patient has no remarkable medical history except for intermittent joint pain. The patient has no history of hypertension and no signs of suggestive SLE.
On admission, vital signs were as follows: blood pressure 160/100 mmHg, heart rate 86 b.p.m., peripheral oxygen saturation 98%, temperature of 38.5°C, and respiratory rate 22 x/minute. Physical examinations were notable for lung rales and early diastolic murmur at aortic valve area on auscultation with apical displacement on palpation and bilateral pretibial oedema with vasculitis erythematous sign on palmar and plantar fingers (Figure 1). Other findings were unremarkable. Electrocardiography showed sinus rhythm with non-specific R wave progression sign. Chest X-ray demonstrated cardiomegaly, bilateral pleural effusion, and pulmonary vascular cephalization (Figure 2).
Vasculitis erythematous sign on palmar (left) and plantar (right) fingers area.
Chest X-ray demonstrated cardiomegaly, bilateral pleural effusion, and pulmonary vascular cephalization.
Laboratory test remarkable findings were as follows: Hb 10.8 g/dL, leukocyte 3260/μL, thrombocyte 65 000/μL, erythrocyte sedimentation rate (ESR) 21 mm/h, serum creatinine 2.3 mg/dL, serum albumin 3.4 mg/dL, D-dimer 3032 ng/mL, euthyroid, non-reactive HBsAg, and positive anti-dengue IgM. Urinalysis finding was significant for haematuria and proteinuria. Echocardiography revealed dilatation of all heart chamber with reduced left ventricular ejection fraction (LVEF) of 25% and global hypokinetic and reduced TAPSE to 14 mm. Moderate aortic and tricuspid valve regurgitation were also observed with pericardial effusion also noted (see Supplementary material online, Video S1).
Due to high suspicious of cardiac involvement of autoimmune disease, the patient’s rheumatological work-up was performed. The patient ANA test was positive, and ANA profile showed high likelihood for SLE diagnosis (Table 1). Hence, the patient was diagnosed as dengue-induced SLE pancarditis with acute HF presentation and lupus nephritis (LN). The lupus diagnosis was based on EULAR/ACR criteria with total score of 22, whereas value > 10 is classified as SLE.^7^ Initial Mex-SLEDAI score was 27 which signify for severe disease activity.
Upon to this finding, patient was administered intravenous methylprednisolone 20 mg t.i.d., intravenous loop diuretic furosemide 20 mg/hour, and HF medication: ramipril 5 mg o.d., bisoprolol 2.5 mg o.d., and spironolactone 25 mg o.d. On the 3rd admission day, clinical improvement was observed. Heart failure medications were up-titrated to ramipril 10 mg o.d. and bisoprolol 5 mg o.d. The patient was discharged on the 5th admission day uneventfully. The oral methylprednisolone was continued with regimen 16 mg twice daily.
One week after discharge, cardiac magnetic resonance (CMR) imaging was performed, and we found reduced ejection fraction of 30% with global hypokinetic in LV segment with minimal myocardial oedema. Midwall late gadolinium enhancement (LGE) was also observed at the anteroseptal and anterolateral segments and subepicardial LGE at the basal lateral segment (Figure 3). This finding suggested non-ischaemic LGE and strengthened the myocarditis finding. The patient was administered cyclosporine 50 mg p.o. twice daily for additional immunosuppressive therapy. We observed improvement in renal function during follow-up course up to 2 months post discharge (Table 2).
Cardiac magnetic resonance imaging showed mid-wall late gadolinium enhancement at the anteroseptal and anterolateral segments and subepicardial late gadolinium enhancement at the basal lateral segment which signify for non-ischaemic LGE (yellow arrow).
In three months post-discharge evaluation, we observed remarkable clinical and functional improvement. There was no re-hospitalization period from HF during the follow-up time. Echocardiographic parameter improvement was also observed with LVEF of 60% and TAPSE 20 mm; no residual pericardial effusion was noted (see Supplementary material online, Video S2). Mex-SLEDAI score decreased to 4, demonstrating excellent treatment response with complete cardiac recovery and substantial disease activity reduction. Heart failure and immunosuppressive medication (methylprednisolone and cyclosporin) were continued.
Discussion
Systemic lupus erythematosus is a chronic systemic autoimmune disease, and the proposed mechanism of lupus flare in our case is related to dengue-triggered immunological activation.^1,2^ The recent admission of positive antibody for dengue is hypothetically induced hyperactivity of inflammation and causes pancarditis manifestation. Previous reports have reported the occurrence of dengue-induced SLE flare. Rajadhyaksha and Mehra^8^ described SLE with LN manifestation in dengue virus infection. It is important to consider SLE cardiac manifestation especially in young woman patients who developed acute HF that accompanied with vasculitis stigmata and nephritis.^6^
Lupus myocarditis has a poor prognosis with 40% of patients died or having persistent LV systolic dysfunction although adequately managed. The poor outcome and incomplete recovery were associated with the lower LVEF at initial presentation (LVEF < 35%).^2,3^ Furthermore, the presence of LN involvement, which accounts for 40%–70% of SLE and cutaneous signs of SLE like vasculitis, strengthens the association of lupus activity with our case clinical manifestation.^2,3^ Liu et al.^9^ reported that a higher Mex-SLEDAI score is an independent risk factor contributing to development of myocarditis in SLE patients. Our case also showed high Mex-SLEDAI score at initial presentation, and this is associated with high-risk feature of LM.^1^
Shabbir et al.^10^ reported an immediate SLE flares in young postpartum patient that manifest as cardiac tamponade and myocarditis. There were previous reported cases of life-threatening cardiogenic shock manifestation of SLE myocarditis.^6,11^ Furthermore, Durrance et al.^12^ also reported an acute HF presentation of myopericarditis with valvular dysfunction in SLE patient. Furthermore, isolated myocarditis manifestation of SLE without other system involvement was also been reported by Hutman-Zahler et al.^5^
Interestingly, auto antibodies that found in LM and general SLE patients has no different, except for anti-Ro/SSA antibody that reported to be high as 69% in LM compared to only 40% in general SLE patients and also high activity of anti-Ro/SSA predict the LGE finding from CMR in general SLE patients.^3^ This finding showed that anti-Ro/SSA activity is strongly related with myocardial involvement in SLE,^1,2,5^ as observed in our patient whereas the activity of anti-Ro/SSA antibody is very high. These patterns were also found in previous reports of SLE with cardiac manifestation.^5,11–13^
There were previous reported cases of complete myocardial recovery after several months of steroid therapy in LM patients.^5,6^ The significant and rapid improvement was observed after weeks of appropriate medical management with 60% of complete recovery, while 20% of partial recovery.^2^ We observed complete functional recovery of myocardial function in 3 months after initial immunosuppressive and HF medication in this case.
The clinical spectrum in our case is classified by World Health Organization (WHO) as expanded dengue syndrome (EDS). The EDS is a subset of dengue virus infection beyond the traditional classification with unusual clinical manifestation and multi organ involvement, for instance neurological, gastrointestinal, and renal failure, especially cardiovascular involvement such as myocarditis and pericarditis.^14^ This clinical subset occasionally progressed into serious and life-threatening outcome.^14^ As observed in our case with pancardiac involvement and acute HF. It is hypothesized that dengue cardiac manifestation is caused by direct viral attack and/or immune-mediated mechanism involved.^14^ As in our case context, dengue virus infection induced lupus flare that affect pancardiac inflammation. It is hypothesized that dengue and SLE relied on the same pathogenetic and genetic background.^15^ The EDS is under-recognized clinical spectrum. Hence, the vigilance consideration of EDS potentially addressed the appropriate management strategy for dengue with unusual manifestation.^14^
The association between dengue infection and risk of SLE activation had been described by Chen et al. from large population-based study. History of dengue infection is found more significantly associated with SLE (OR 4.55; P < 0.001) while was not found in other systemic autoimmune rheumatic disease such as Sjogren’s syndrome, systemic sclerosis, and rheumatoid arthritis. This finding had clinical significance concerning short- and long-term effect of dengue infection history for SLE flare that can affect end-organ target especially cardiac tissue.^15^ However, clinical diagnosis establishment of this direct relationship relies on histopathological data from renal and/or skin rash tissue.
With the lack of histopathology data of renal and skin rash, the clinical question emerged whether the clinical syndrome in our patient constitutes a self-resolved dengue-induced pancarditis with false-positive SLE laboratory test or a dengue-induced SLE flare that involves pancardiac inflammation and HF. This becomes the limitation of this case report. However, the establishment of dengue-induced lupus flare diagnosis in our case relied on several objective finding. Firstly, the skin vasculitis that concomitantly occurred during the acute cardiac decompensation strengthens the possibility of autoimmune-mediated clinical syndrome. Second, the EULAR/ACR and Mex-SLEDAI clinical score assessment were highly associated with lupus activity. Lastly, LN finding in our casestrenghtening the association with lupus activity.
Other limitation in our case report was the absence of dengue genomic and serotype identification due to resource constraint. However, to the best of our knowledge, this is a first case report of pancardiac involvement of dengue-induced SLE that responded well with immunosuppressive and HF therapy as recommended.^2^ This condition is potentially to be under-recognized and resulting in delaying diagnosis.^1,12^ Early detection and appropriate management of immunosuppressive for primary insult of SLE become the key management approach.
Supplementary Material
ytag211_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dawi J, Affa S, Misakyan Y, Fardeheb S, Kades S, Kiriaki A, et al Exploring cardiovascular implications in systemic lupus erythematosus: a holistic analysis of complications, diagnostic criteria, and therapeutic modalities, encompassing pharmacological and adjuvant approaches. Biomol Concepts 2024;15:10.1515/bmc-2022-0051.
- 2Guglin M, Smith C, Rao R. The spectrum of lupus myocarditis: from asymptomatic forms to cardiogenic shock. Heart Fail Rev 2021;26:553–560.33210224 10.1007/s 10741-020-10054-w · doi ↗ · pubmed ↗
- 3du Toit R, Karamchand S, Doubell AF, Reuter H, Herbst PG. Lupus myocarditis: review of current diagnostic modalities and their application in clinical practice. Rheumatology (Oxford) 2023;62:523–534.35861382 10.1093/rheumatology/keac 409 · doi ↗ · pubmed ↗
- 4Schulz-Menger J, Collini V, Gröschel J, Adler Y, Brucato A, Christian V, et al 2025 ESC guidelines for the management of myocarditis and pericarditis. Eur Heart J 2025;46:ehaf 192.
- 5Hutman-Zahler A, Goldstein J, Anderson T, Balatico M, Brophy DR, Aoki J, et al A rare case of fulminant myocarditis leading to the diagnosis of systemic lupus erythematosus. JACC Case Rep 2025;30:104049.40681274 10.1016/j.jaccas.2025.104049 PMC 12441452 · doi ↗ · pubmed ↗
- 6Liu L, Dong Y, Gao H, Yao D, Zhang R, Zheng T, et al Cardiogenic shock as the initial manifestation of systemic lupus erythematosus. ESC Heart Fail 2020;7:1992–1996.32515553 10.1002/ehf 2.12806 PMC 7373915 · doi ↗ · pubmed ↗
- 7Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis 2019;78:1151–1159.31383717 10.1136/annrheumdis-2018-214819 · doi ↗ · pubmed ↗
- 8Rajadhyaksha A, Mehra S. Dengue fever evolving into systemic lupus erythematosus and lupus nephritis: a case report. Lupus 2012;21:999–1002.22354536 10.1177/0961203312437807 · doi ↗ · pubmed ↗