68Ga-PSMA-11 PET/CT for Initial Staging of Unfavorable Intermediate-Risk and High-Risk Prostate Cancer Predicts Overall Survival: An IAEA Multicenter Study
Juliano J. Cerci, Stefano Fanti, Enrique E. Lobato, Rakesh Kumar, Jolanta Kunikowska, Akram Al-Ibraheem, Maisarah Nasir, Francisca Redondo Moneda, Osvaldo Garcia, Mohamad Haidar, Fuad Novruzov, Ozlem Kucuk, Umut Elboga, Murilo de Almeida Luz, Diana Paez

TL;DR
A study shows that 68Ga-PSMA-11 PET/CT scans can predict survival outcomes in men with high-risk prostate cancer, helping guide treatment decisions.
Contribution
This study demonstrates that 68Ga-PSMA-11 PET/CT is an independent prognostic tool for survival in high-risk prostate cancer patients.
Findings
Patients with NxM1 disease had significantly worse two-year overall survival (86.8%) compared to N0M0 (99.3%).
68Ga-PSMA-11 PET/CT status was the only significant prognostic factor for survival outcomes.
Higher biochemical recurrence rates were observed in N1M0 and NxM1 groups compared to N0M0.
Abstract
Although multiple studies have demonstrated the accuracy of 68Ga-PSMA-11 PET/CT, its ability to predict survival outcomes and treatment response remains unclear. This study assessed the prognostic value of 68Ga-PSMA-11 PET/CT in staging unfavorable intermediate- or high-risk prostate cancer (PCa) in patients who are candidates for radical prostatectomy. Methods: This prospective multicenter trial supported by the International Atomic Energy Agency enrolled 775 patients across 11 countries with newly diagnosed, unfavorable intermediate- or high-risk PCa. Patients underwent 68Ga-PSMA-11 PET/CT, after which their disease was categorized as N0M0 (no involvement of local nodes and no metastases), N1M0 (pelvic lymph node involvement), or NxM1 (distant metastases). These findings were then compared with clinical follow-up data. Results: Biochemical recurrence rates were 35.4% (N0M0), 68.2%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
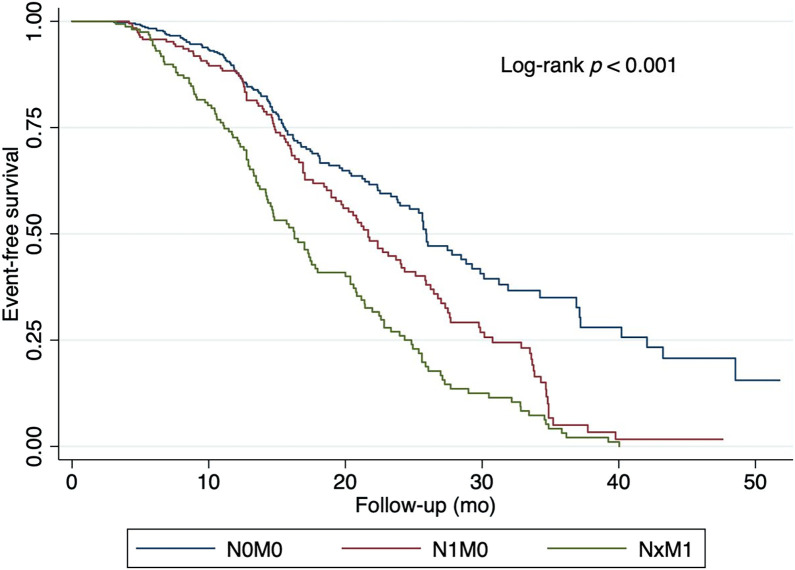 FIGURE 1
FIGURE 1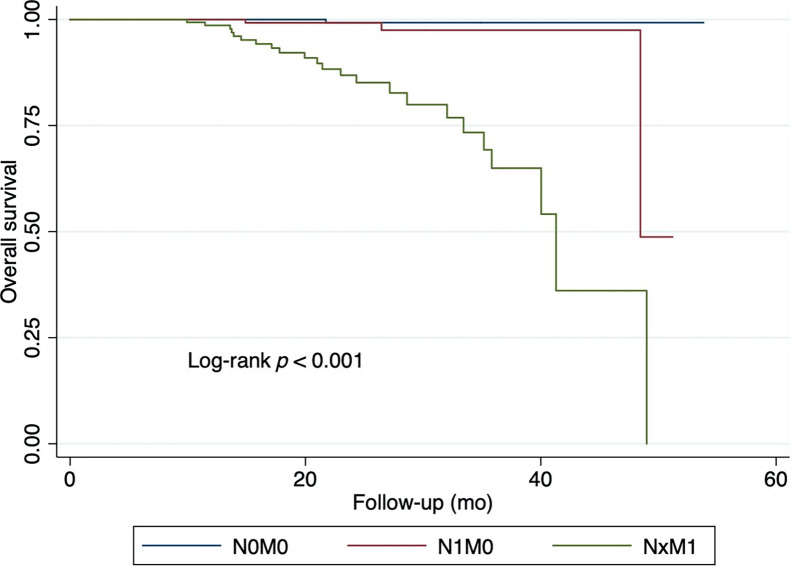 FIGURE 2
FIGURE 2| Characteristic | Value |
|---|---|
| Gleason score | |
| 3 + 4 | 102 (13.2) |
| 3 + 5 | 7 (0.9) |
| 4 + 3 | 231 (29.8) |
| 4 + 4 | 240 (31.0) |
| 4 + 5 | 123 (15.9) |
| 5 + 3 | 3 (0.4) |
| 5 + 4 | 42 (5.4) |
| 5 + 5 | 26 (3.4) |
| ISUP grade | |
| 2 | 73 (9.4) |
| 3 | 303 (39.1) |
| 4 | 280 (36.1) |
| 5 | 192 (24.8) |
| High-risk PCa | 555 (71.6) |
| Age (y) | 67.35 |
| PSA (ng/mL) | 15.8 |
| % | |||||
|---|---|---|---|---|---|
| Category |
| BCR | No. deaths | 2-y EFS | 2-y OS |
| N0M0 | 438 | 155 (35.4) | 1 | 56.6 | 99.3 |
| N1M0 | 337 | 230 (68.2) | 2 | 43.9 | 99.2 |
| NxM1 | 158 | 122 (77.2) | 23 | 26.0 | 86.8 |
| Variable | HR | 95% CI | |
|---|---|---|---|
| Univariate analysis | |||
| N1M0 | 1.57 | 0.00 | 1.22–2.02 |
| NxM1 | 2.59 | 0.00 | 2.03–3.31 |
| Multivariate analysis | |||
| Disease category | |||
| N1M0 | 1.59 | 0.00 | 1.22–2.06 |
| NxM1 | 2.65 | 0.00 | 2.03–3.46 |
| Age | 0.99 | 0.82 | 0.98–1.01 |
| ISUP grade | 1.15 | 0.66 | 0.99–1.33 |
| High-risk status | 0.78 | 0.14 | 0.57–1.08 |
| PSA level | 0.99 | 0.42 | 0.99–1.00 |
| Variable | HR | 95% CI | |
|---|---|---|---|
| Univariate analysis | |||
| N1M0 | 5.78 | 0.130 | 0.59–55.95 |
| NxM1 | 56.37 | 0.000 | 7.54–420.95 |
| Multivariate analysis | |||
| Disease category | |||
| N1M0 | 4.83 | 0.176 | 0.49–47.32 |
| NxM1 | 50.13 | 0.000 | 6.35–395.38 |
| Age | 0.99 | 0.777 | 0.95–1.03 |
| ISUP grade | 1.09 | 0.758 | 0.62–1.91 |
| High-risk status | 2.81 | 0.211 | 0.55–14.19 |
| PSA level | 0.99 | 0.630 | 0.99–1.00 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Prostate Cancer Diagnosis and Treatment · Radiopharmaceutical Chemistry and Applications
Prostate cancer (PCa) is the second most common malignancy in men and the fifth leading cause of cancer-related deaths worldwide (1). The prognosis of PCa varies widely, depending on the extent of disease at the time of diagnosis. Accurate initial staging is essential for differentiating between patients who may benefit from local therapies (e.g., radical prostatectomy or radiotherapy) and those requiring systemic treatment because of nodal or metastatic disease (2).
Conventional imaging modalities, including MRI, CT, and bone scintigraphy, are routinely used for staging, but their accuracy is limited, particularly in detecting micrometastases and small lymph node involvement. In the past decade, ^68^Ga-labeled prostate-specific membrane antigen (PSMA) PET/CT has emerged as a highly sensitive imaging technique, capable of identifying early metastatic disease that may not be detected by conventional imaging (3–6).
Although multiple studies have demonstrated the superior accuracy of ^68^Ga-PSMA-11 PET/CT, its ability to predict survival outcomes and treatment response remains unclear (7,8).
Determining whether ^68^Ga-PSMA-11 PET/CT can effectively differentiate disease states associated with distinct oncologic outcomes would support its use as a first-line staging tool, enhance treatment decision-making based on imaging findings, and facilitate informed patient counseling regarding the risk and timing of potential treatment failure.
Supported by the International Atomic Energy Agency, this multicenter worldwide trial aimed to evaluate the prognostic impact of ^68^Ga-PSMA-11 PET/CT staging in patients with unfavorable intermediate- or high-risk PCa who were candidates for radical prostatectomy.
MATERIALS AND METHODS
Study Design and Population
This prospective, multicenter, international trial enrolled patients with newly diagnosed, biopsy-confirmed, treatment-naïve unfavorable intermediate- or high-risk PCa (9) who were candidates for radical prostatectomy whose disease was staged as nonmetastatic on conventional imaging (MRI, CT, and bone scintigraphy). Patients with evidence of another malignancy, except nonmelanoma skin cancer, were excluded.
This study involved 12 centers from 11 countries, totaling 775 patients: Azerbaijan, 29 patients; Brazil, 180; Chile, 38; India, 160; Italy, 99; Jordan, 64; Lebanon, 30; Malaysia, 43; Mexico, 31; Poland, 69; and Turkey, 32.
Standard forms for data registration were developed and agreed on by the investigators. Data were collected for ^68^Ga-PSMA-11 PET/CT positivity rate, localization of positive findings, and impact on patient management. All centers obtained local ethical clearance for prospective recruitment of patients and data collection, in accordance with national regulations. The institutional review board of each center approved this study, and all patients provided written informed consent.
Studies were performed in accordance with existing procedural international guidelines. On the basis of procedure guidelines for PCa imaging, findings were classified as either positive or negative regarding prostate, seminal vesicle, lymph node, and metastatic involvement (10).
Either analog or digital tomographs were allowed; true whole-body imaging, including lower limbs, contrast-enhanced CT obtained with the application of a diuretic was also allowed. All centers had more than 5 y of experience reporting ^68^Ga-PSMA-11 PET/CT results.
Imaging and Risk Stratification
All patients underwent ^68^Ga-PSMA-11 PET/CT, and their disease was categorized as N0M0 (no involvement of local nodes and no metastases), N1M0 (pelvic lymph node involvement), or NxM1 (distant metastases).
Outcomes
The primary outcome was overall survival (OS). Death from any cause was treated as a censoring event. The secondary outcome was event-free survival (EFS), defined as the earliest occurrence of any of the following events: biochemical recurrence (BCR) after radical prostatectomy, defined as a prostate-specific antigen (PSA) level of 0.2 ng/mL or greater confirmed by a second measurement (11); BCR after radiotherapy, defined as an increase in PSA level of at least 2 ng/mL above the nadir, according to the Phoenix definition (12); radiologic progression, defined as local recurrence or the appearance of new metastatic lesions detected on imaging, including PSMA PET/CT (13); or death from any cause.
Statistical Analyses
A prespecified statistical analysis plan measured time-to-event outcomes from the date of study inclusion, with events recorded at the time of detection. Survival was estimated using Kaplan–Meier curves, with 2-y survival rates and 95% CIs reported. Cox proportional hazards regression models were used to compare the 3 groups in univariate and multivariate analyses unadjusted and adjusted for PSA, Gleason score, International Society of Urological Pathology (ISUP) grade, and age.
Categoric variables are presented as counts and percentages, and continuous variables as means with SDs and medians with ranges. Analyses were conducted using SPSS (IBM) and independently reviewed by a statistician.
RESULTS
Outcomes Based on 68Ga-PSMA-11 PET/CT Staging
The clinical characteristics of patients are summarized in Table 1. Most patients (71.6%) met the criteria for high-risk PCa. Detailed treatment data and the impact of PSMA PET findings on surgical management have been previously reported (14).
Survival outcomes differed markedly across PSMA PET–defined staging groups. Patients with N0M0 disease had the highest 2-y EFS and OS rates, whereas those with distant metastases (NxM1) had substantially poorer outcomes (Table 2; Figs. 1 and 2).
Association between 68Ga-PSMA-11 PET/CT and EFS.
Association between 68Ga-PSMA-11 PET/CT and OS.
EFS
Univariate analyses found that ^68^Ga-PSMA-11 PET/CT was the only factor significantly associated with treatment failure, with 2-y EFS rates of 56.6% for those with N0M0 disease, 43.9% (hazard ratio [HR], 1.57) for those with N1M0 disease, and 26% (HR, 2.59) for those with metastatic disease (P < 0.001) (Table 3).
In the multivariate analysis, the HR for patients with N1M0 disease was 1.59 (P < 0.001), significantly associated with worse EFS rates (Table 3; Fig. 1). Patients with metastatic disease had a HR of 2.65 (P < 0.001), which was more strongly associated with poor EFS rates. Age, ISUP grade, high-risk status, and PSA level were not significant predictors of EFS in this model.
OS
Univariate analyses found that ^68^Ga-PSMA-11 PET/CT was the only factor significantly associated with OS, with 2-y OS rates of 99.3% for patients with N0M0 disease, 99.2% for patients with N1M0 disease, and 86.8% for patients with NxM1 disease (P < 0.001) (Table 4). The HR for patients with N1M0 disease was 5.78 (P = 0.130), whereas patients with NxM1 disease had a HR of 56.37 (P < 0.001).
In the multivariate analysis, patients with N1M0 disease had a HR of 4.83 (P = 0.176), which was not associated with worse OS rates. Those with NxM1 disease had a HR of 50.13 (P < 0.001), which had a stronger association with poor OS rates (Table 4; Fig. 2). Age, ISUP grade, high-risk status, and PSA were not significant predictors of OS in this model.
DISCUSSION
To the best of our knowledge, this is the first trial to demonstrate the prognostic value of ^68^Ga-PSMA-11 PET/CT for determining OS as an independent parameter in a large international multicenter cohort of patients with unfavorable intermediate- or high-risk PCa who were candidates for prostatectomy. Our findings confirm that staging of PCa with ^68^Ga-PSMA-11 PET/CT is a strong predictor of treatment outcomes, including OS. Beyond improving staging, ^68^Ga-PSMA-11 PET/CT provides meaningful prognostic information that may guide treatment decisions. Patients classified as having N0M0 disease exhibited significantly better EFS and OS rates compared with those with NxM1 disease, underscoring the prognostic utility of ^68^Ga-PSMA-11 PET/CT.
A few studies have shown that PSMA-defined tumor burden correlates with EFS and OS across various clinical contexts, particularly in patients undergoing salvage radiotherapy after radical prostatectomy. Wenzel et al. demonstrated in more than 1,500 patients that locoregional PSMA-positive findings were highly prognostic for 5-y metastasis-free survival in the setting of salvage radiotherapy in patients with recurrent PCa (HR, 13.8; 95% CI, 7.5–25.2; P < 0.001) (15). Emmett et al. (16) similarly reported that PSMA PET/CT was highly predictive of 3-y freedom from progression in men undergoing salvage radiotherapy for BCR of PCa.
In contrast, prognostic data in the initial staging setting remain limited. Hofman et al. (17) evaluated approximately 300 patients with intermediate- to high-risk PCa using baseline ^68^Ga-PSMA-11 PET/CT and found that PSMA-positive nodal disease was associated with a significantly higher risk of treatment failure. Reported EFS rates were 75% for patients with N0M0 disease and 57% for those with N1M0 disease, higher than our findings of 56.6% and 43.9%, respectively. These discrepancies may reflect differences in patient populations. Our cohort consisted exclusively of patients with unfavorable intermediate- or high-risk PCa from a broad international sample, whereas the sample evaluated by Hofman et al. included those with favorable intermediate-risk disease.
Xiang et al. (18) retrospectively evaluated a PSMA PET/CT–derived risk stratification tool in patients with high-risk or very high-risk PCa, categorized as localized and nonlocalized PCa, demonstrating that PSMA PET/CT nomogram classification was significantly associated with long-term oncologic outcomes, such as BCR, development of distant metastases, and PCa-specific mortality. Our results align with these findings but in a wider clinical context, using only PSMA PET–derived disease extent rather than a composite nomogram. PSMA-detected N1M0 and NxM1 disease remained independent predictors of worse EFS rates, even after adjustment for age, ISUP grade, high-risk status, and PSA level. For OS, PSMA-detected metastatic disease was the only significant predictor, with patients with metastatic disease exhibiting a nearly 50-fold higher risk of death.
Sweere et al. (19) also demonstrated the prognostic value of PSMA PET/CT, showing that the clinical tumor stage assessed by PSMA PET was independently associated with BCR-free survival in a multivariate analysis, adjusting for clinical parameters and MRI-derived staging. Karpinski et al. (20) found that combining PSMA PET information with PROMISE criteria improved disease risk classification. While these approaches—such as molecular imaging TNM classification, uptake quantification, and PSMA tumor volume—provide additional refinement, their implementation requires specialized software, standardization, and expertise not widely available. Thus, our use of simple PSMA-based staging categories allows broad clinical applicability across diverse practice settings.
As ^68^Ga-PSMA-11 PET/CT becomes the standard practice for PCa staging, its prognostic implications are expected to increasingly influence treatment paradigms. Incorporating PSMA PET–based risk stratification into treatment planning may support more personalized management, including metastasis-directed therapy and intensified systemic therapy for high-risk patients. Ongoing prospective trials are evaluating whether PSMA PET–guided treatment escalation improves long-term outcomes (8). As evidence expands, PSMA PET/CT is likely to redefine risk-adapted management strategies, further solidifying its role as a fundamental tool in initial PCa staging.
Clinical Implications
In practical terms, ^68^Ga-PSMA-11 PET/CT clearly differentiates patients with a high likelihood of treatment success (N0M0) from those with markedly poorer prognosis (NxM1) who may benefit from intensified systemic therapy. These results highlight the potential of PSMA PET/CT to guide timely and appropriate treatment selection, particularly for patients with PSMA-detected metastatic disease.
Limitations
This study had several limitations. First, the absence of a randomized control group limits direct comparison with patients staged using conventional imaging alone. Second, treatment regimens varied across centers, introducing potential heterogeneity in outcomes. Third, although the median follow-up time of 36 mo is informative, longer-term data are needed to fully assess the prognostic impact of ^68^Ga-PSMA-11 PET/CT, particularly for patients with more favorable disease who may experience late events.
CONCLUSION
^68^Ga-PSMA-11 PET/CT is a robust and independent prognostic marker in patients with unfavorable intermediate- or high-risk PCa who are candidates for radical prostatectomy. These findings support routine integration of ^68^Ga-PSMA PET/CT into initial staging for survival predictions, opening the possibilities to more tailored treatment and potentially better outcomes.
DISCLOSURE
This research was partially funded by the International Atomic Energy Agency. No other potential conflict of interest relevant to this article was reported.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1James ND Tannock IN’Dow J. The Lancet Commission on prostate cancer: planning for the surge in cases. Lancet. 2024;403:1683–1722.38583453 10.1016/S 0140-6736(24)00651-2PMC 7617369 · doi ↗ · pubmed ↗
- 2Schaeffer EM Srinivas S Adra N. NCCN Guidelines insights: prostate cancer, version 3.2024. J Natl Compr Canc Netw. 2024;22:140–150.38626801 10.6004/jnccn.2024.0019 · doi ↗ · pubmed ↗
- 3Gillessen S Bossi A Davis ID. Management of patients with advanced prostate cancer. Part I: intermediate-/high-risk and locally advanced disease, biochemical, and side effects of hormonal treatment: report of the Advanced Prostate Cancer Consensus Conference 2022. Eur Urol. 2023;83:267–293.36494221 10.1016/j.eururo.2022.11.002PMC 7614721 · doi ↗ · pubmed ↗
- 4Perera M Papa N Christidis D. Sensitivity, specificity, and predictors of positive 68Ga-prostate-specific membrane antigen positron emission tomography in advanced prostate cancer: a systematic review and meta-analysis. Eur Urol. 2016;70:926–937.27363387 10.1016/j.eururo.2016.06.021 · doi ↗ · pubmed ↗
- 5Hope TA Aggarwal R Chee B. Impact of 68Ga-PSMA-11 PET on management in patients with biochemically recurrent prostate cancer. J Nucl Med. 2017;58:1956–1961.28522741 10.2967/jnumed.117.192476 · doi ↗ · pubmed ↗
- 6Hofman MS Lawrentschuk N Francis RJ.; pro PSMA Study Group Collaborators. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (pro PSMA): a prospective, randomised, multicentre study. Lancet. 2020;395:1208–1216.32209449 10.1016/S 0140-6736(20)30314-7 · doi ↗ · pubmed ↗
- 7Roberts MJ Morton A Donato P. 68Ga-PSMA PET/CT tumour intensity pre-operatively predicts adverse pathological outcomes and progression-free survival in localised prostate cancer. Eur J Nucl Med Mol Imaging. 2021;48:477–482.32696091 10.1007/s 00259-020-04944-2 · doi ↗ · pubmed ↗
- 8Roberts MJ Maurer T Perera M. Using PSMA imaging for prognostication in localized and advanced prostate cancer. Nat Rev Urol. 2023;20:23–47.36473945 10.1038/s 41585-022-00670-6 · doi ↗ · pubmed ↗