Foetal Reduction in a Cornual Heterotopic Pregnancy With Potassium Chloride Administration
Yi Hui Liu

TL;DR
This paper presents a case of a rare heterotopic pregnancy managed by preserving the intrauterine pregnancy and using potassium chloride for the ectopic pregnancy.
Contribution
The paper introduces a specific case management approach using potassium chloride for ectopic pregnancy in a heterotopic scenario.
Findings
A heterotopic pregnancy was successfully managed with potassium chloride administration.
The intrauterine pregnancy was preserved during the procedure.
The case highlights the potential of KCl as a management option for ectopic pregnancies.
Abstract
Heterotopic pregnancy is the simultaneous occurrence of an intrauterine pregnancy with an extrauterine pregnancy. Heterotopic pregnancies remain a diagnostic challenge, as many can be asymptomatic, or clinicians could be falsely reassured once an intrauterine pregnancy is sighted on an ultrasound. Given their rarity, there is also no global consensus on management guidelines. In this study, we illustrate a case of a heterotopic pregnancy with preservation of the intrauterine pregnancy and management of the ectopic pregnancy with potassium chloride (KCl) administration.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
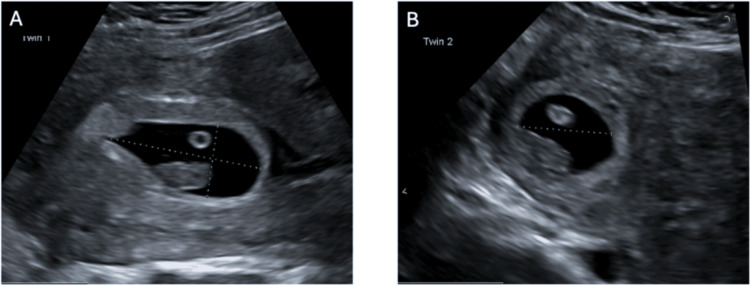 Figure 1
Figure 1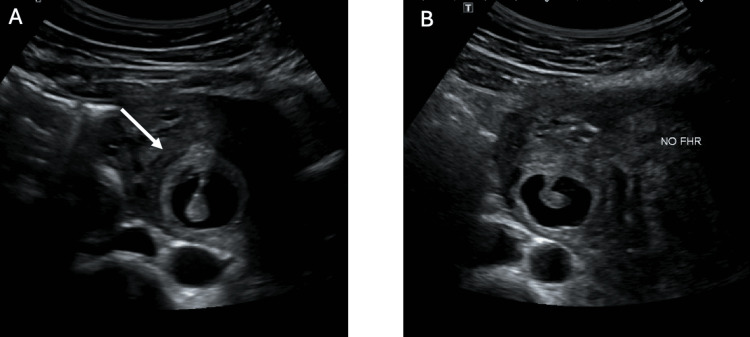 Figure 2
Figure 2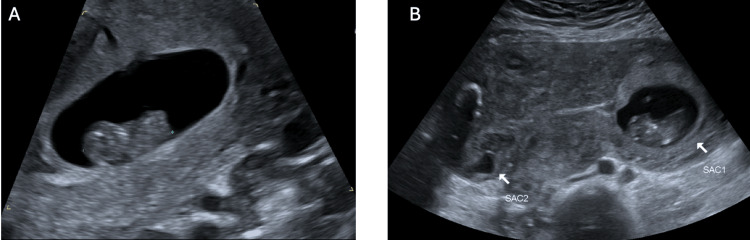 Figure 3
Figure 3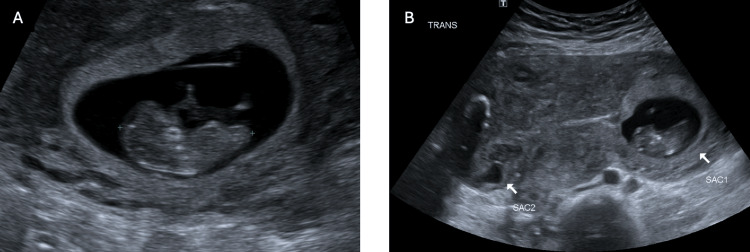 Figure 4
Figure 4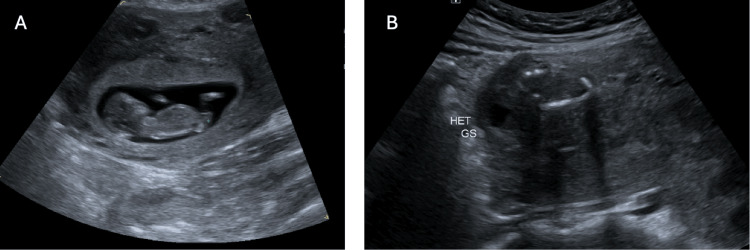 Figure 5
Figure 5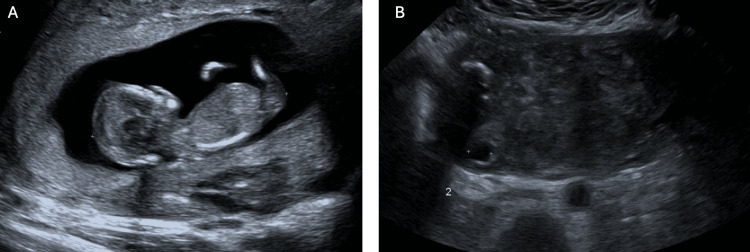 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Gestational Trophoblastic Disease Studies · Gynecological conditions and treatments
Introduction
Heterotopic pregnancy is a rare condition in which there is the simultaneous conception of an intrauterine and an ectopic pregnancy. The incidence is reportedly 1 in 30,000 spontaneous conceptions but increases to as high as 1 in 100 pregnancies in patients undergoing assisted reproductive technology (ART) [1,2]. The significant difference in incidence is likely secondary to multiple embryo transfers in ART [3,4]. The most common extrauterine sites include the fallopian tubes, which account for approximately 90% of all heterotopic pregnancies, and less commonly cornual, cervical, caesarean, and abdominal sites [5]. Heterotopic pregnancies typically manifest with abdominal pain, peritoneal irritation, and vaginal bleeding, but a minority of patients can be asymptomatic. Heterotopic pregnancies remain a diagnostic challenge, as symptoms can range widely, and the presence of a confirmed intrauterine pregnancy can delay diagnosis [6]. In this study, we present a case of a naturally conceived heterotopic pregnancy and the management of the ectopic pregnancy using KCl with conservation of the intrauterine viable pregnancy.
Case presentation
The patient is a female in her 40s, gravidarum 2 parity 1, who was sent in from an outpatient ultrasound facility to the emergency department with a confirmed heterotopic pregnancy at approximately seven weeks of gestation (Figure 1). The ultrasound was initially completed as a dating scan. She was haemodynamically stable and asymptomatic, including nil abdominal pain. Her blood results were unremarkable with a BHCG of 189,910 IU/L.
Transvaginal ultrasound demonstrating a heterotopic pregnancy(A) Intrauterine pregnancy with a gestational sac corresponding to approximately 7+5 weeks gestation.(B) Cornual ectopic pregnancy with a gestational sac corresponding to approximately 7+5 weeks gestation.
Her obstetric history included one previous elective lower segment caesarean section in 2022. She had regular 28-day menstrual cycles. Her gynaecological history was significant for a known multifibroid uterus with a previous laparoscopic myomectomy in 2013 for an intramural fibroid. She had a history of genital herpes with no flare-ups in the last few years. She had an up-to-date cervical screening test and nil history of sexually transmitted infections or pelvic inflammatory diseases. Her past medical history was significant for Hashimoto's thyroiditis, asthma, and mild mitral regurgitation, which she regularly follows up with a cardiologist. Her regular medications include 50 micrograms of thyroxine daily and Symbicort (budesonide-formoterol) and salbutamol as needed. She had no known drug allergies.
The impression is a heterotopic cornual pregnancy with a viable intrauterine pregnancy. The management options were provided to the patient for either preservation of the intrauterine pregnancy with ultrasound-guided KCl injection into the cornual ectopic pregnancy or laparoscopic removal of the cornual ectopic pregnancy, or termination of both the cornual and intrauterine pregnancies with laparoscopic removal of the ectopic pregnancy, a dilatation of the cervix, and curettage of the uterus.
A shared decision was made for ultrasound-guided KCl injection into the cornual ectopic pregnancy with attempted preservation of the intrauterine pregnancy. The procedure was completed with a 22-gauge needle into the ectopic gestational sac with mechanical disruption of the foetal pole, 5 mL of the gestational sac fluid aspirated, and 0.75 g of potassium chloride injected into the foetal pole/gestational sac. A short-interval progress ultrasound after the procedure demonstrated a foetal heartbeat in the intrauterine pregnancy and no foetal heartbeat in the extrauterine pregnancy, presuming foetal demise (Figure 2). The patient was well and able to go home the same day. She was followed up through the early pregnancy outpatient service with weekly pelvic ultrasounds, demonstrating a progressive viable intrauterine pregnancy with the demise of the cornual ectopic pregnancy (Figure 3-6). Since the time of publication, she continues to have a progressive pregnancy with regular antenatal care.
Ultrasound-guided administration of potassium chloride (KCl)(A) Ultrasound demonstrating disruption of the gestational sac and injection of the KCl.(B) Ultrasound post-administration of KCl demonstrating subsequent asystole in the cornual ectopic pregnancy.
Pelvic ultrasound seven days post KCl administration(A) Progressive intrauterine pregnancy that is approximately 9+2 gestation by crown rump length.(B) Sac 1 illustrating progressive intrauterine pregnancy and Sac 2 demonstrating previous right cornual ectopic pregnancy with nil further growth.KCl: Potassium chloride
Pelvic ultrasound 14 days post KCl administration(A) Progressive intrauterine pregnancy that is approximately 10+1 weeks gestation by crown rump length.(B) Sac 1 illustrating progressive intrauterine pregnancy and Sac 2 demonstrating previous right cornual ectopic pregnancy with nil further growth (approximately 1.0 x 8.0 x 1.2 cm).
Pelvic ultrasound 21 days post-KCl administration(A) Progressive intrauterine pregnancy that is approximately 11+4 weeks gestation by crown rump length.(B) Previous right cornual ectopic pregnancy with nil further growth (approximately 1.7 x 0.9 x 1.1 cm).
Pelvic ultrasound 28 days post-KCl administration(A) Progressive intrauterine pregnancy that is approximately 13+3 weeks gestation by crown rump length.(B) Previous right cornual ectopic pregnancy with nil further growth (1.4 x 1.1 x 0.9 cm).
Discussion
This case contributes to the growing literature on heterotopic pregnancies while also demonstrating two important points. Heterotopic pregnancies remain a diagnostic challenge for clinicians, as they could manifest asymptomatically or in vague symptoms that often occur in early pregnancy. There could also be a delay in diagnosis with false reassurance when ultrasounds confirm an intrauterine pregnancy. Thus, it is important for clinicians to have a high degree of suspicion and be aware of the risk factors for heterotopic pregnancy. These risk factors include assisted reproductive technologies, particularly in vitro fertilisation and embryo transfer, tubal pathology, history of pelvic inflammatory disease, history of multiple abortions, previous abdomino-pelvic or tubal surgery, and family history of multiple gestations [3,7-10]. In this study, we demonstrate a patient with some risk factors, including a history of previous laparoscopic myomectomy and a previous caesarean section. However, she did not have any other risk factors, including previous tubal pathology, did not have any classic symptoms, and had naturally conceived without the use of ART. The diagnosis was made from a routine antenatal dating scan at a tertiary centre. Thus, it is important for clinicians to be aware of this rare but serious condition and to consider it as a possible differential diagnosis for any pregnant woman.
Second, this case shares a unique management process for a heterotopic pregnancy to preserve a viable intrauterine pregnancy. The current mainstay management of a heterotopic pregnancy is surgical removal of the extrauterine gestation [11,12]. However, with the advent of readily accessible ultrasound imaging and multidisciplinary teams with interventional radiologists, there should be further consideration of the use of medical management with KCl. The advantages of medical management over surgical management include faster recovery, reduction in blood loss, shorter hospital stays, and less invasive procedures. Previous studies have demonstrated more favourable outcomes for surgical management of cornual heterotopic pregnancies, with only half of those with KCl administration achieving a live birth [13]. However, this is more likely due to the lack of patient risk stratification. In stable patients with early detection of a heterotopic pregnancy and low risk of abscondment, there is less risk of rupture; thus, medical management can arguably be more beneficial than surgical management. Fernandez et al. developed a scoring system that evaluated the success of non-surgical management with heterotopic cornual pregnancies by looking at gestational sac, beta-human chorionic gonadotrophin level, progesterone level, presence of abdominal pain, volume of hemoperitoneum, and ultrasonographic diameter of hematosalpinx. This study found that if the total score was ≤12, then the likelihood of success of medical treatment was >80% [14]. This case demonstrates the same principles in which a stable patient with an early diagnosis was able to achieve selective foetal reduction with KCl and continue with a progressive pregnancy.
Currently, there is no consensus for the treatment of heterotopic pregnancies. Further large-scale studies will need to be completed to demonstrate maternal and foetal outcomes that may help further guide management in these cases and to differentiate parameters in which medical management may be more advantageous than surgical management.
Conclusions
Heterotopic pregnancies are rare but serious conditions that clinicians should be aware of and rule out in early pregnancy, particularly with the increase in incidence with ART. This case illustrates a patient who was able to have a successful reduction of an ectopic pregnancy with preservation of the intrauterine pregnancy using KCl. Simultaneously, this case also illustrates the need for further research to help develop international guidelines on the management of heterotopic pregnancies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Simultaneous intrauterine and extrauterine pregnancy Am J Obstet Gynecol De Voe R.W Pratt J.H 5690357569035323194810.1016/s 0002-9378(48)90357-318893768 · doi ↗ · pubmed ↗
- 2Heterotopic pregnancy after in vitro fertilization and embryo transfer Acta Obstet Gynecol Scand Ikeda SI Sumiyoshi M Nakae M 4634647719989598960 · pubmed ↗
- 3The rising incidence of heterotopic pregnancy: Current perspectives and associations with in-vitro fertilization Eur J Obstet Gynecol Reprod Biol Maleki A Khalid N Rajesh Patel C El-Mahdi E 13814426620213465391810.1016/j.ejogrb.2021.09.031 · doi ↗ · pubmed ↗
- 4Heterotopic pregnancy after ovulation induction and assisted reproductive technologies: a literature review from 1971 to 1993 Fertil Steril Tal J Haddad S Gordon N Timor-Tritsch I 11223199610.1016/s 0015-0282(16)58378-28752602 · doi ↗ · pubmed ↗
- 5ACOG practice bulletin no. 193: tubal ectopic pregnancy Obstet Gynecol Committee on Practice Bulletins—Gynecology 0131201810.1097/AOG.000000000000256029470343 · doi ↗ · pubmed ↗
- 6Heterotopic pregnancy J Obstet Gynaecol Talbot K Simpson R Price N Jackson SR 7123120112128098510.3109/01443615.2010.522749 · doi ↗ · pubmed ↗
- 7Tubal infertility and pelvic adhesion increase risk of heterotopic pregnancy after in vitro fertilization: A retrospective study Medicine (Baltimore) Pi R Liu Y Zhao X 099202010.1097/MD.0000000000023250 PMC 766844133181716 · doi ↗ · pubmed ↗
- 8The risk factors and pregnancy outcomes of 48 cases of heterotopic pregnancy from a single center J Korean Med Sci Jeon JH Hwang YI Shin IH 109410993120162736600810.3346/jkms.2016.31.7.1094 PMC 4901002 · doi ↗ · pubmed ↗